
Abstract
The aim of the present study was to evaluate the clinical practice patterns in maximal medical therapy (MMT) before endoscopic sinus surgery for chronic rhinosinusitis (CRS) by Chinese otolaryngologists. An anonymous web-based survey of MMT was performed. This survey assessed types of therapies, the frequency of use, duration of use, and demographic data of respondents. A total of 134 (26.8%) questionnaires were completed and returned. The majority (62.69%) of respondents would consider surgery less than 3 months after commencing MMT, 33.58% would wait 3 to 6 months. Intranasal corticosteroid sprays, saline irrigation, oral antibiotics, oral mucolytics, and oral Chinese herbals were the most commonly used therapies and listed as “often (>70%)”. Macrolides were most commonly antibiotics prescribed among the clinicians surveyed (51.49%). Intranasal corticosteroid sprays, oral antibiotics, oral mucolytics, nasal saline irrigations, and oral Chinese herbals are most commonly prescribed by the majority of Chinese otolaryngologists as MMT for CRS. Current practice patterns of MMT among Chinese otolaryngologists are not uniformly based on evidence-based guidelines.
Introduction
Statements of numerous chronic rhinosinusitis (CRS) guidelines regarding indications for sinus surgery invariably cite “failure of maximal medical therapy” (MMT) as a prerequisite; 1 -7 However, the definition of “MMT” still seems to vary greatly among CRS guidelines and clinicians. Maximal medical therapy is also known as “appropriate or optimal medical therapy.” There are no clinical trials evaluating the optimal combination of drugs for MMT. There are several CRS guidelines where recommendations are made, and these demonstrate consistency in regard to the inclusion of oral antibiotics, intranasal corticosteroid sprays (INCS), nasal saline irrigation, selective use of oral corticosteroids, oral antihistamines, and oral antileukotriene agents.
Two previous survey studies revealed the prescription patterns for CRS. 8,9 A survey of otolaryngology consultants in the United Kingdom (UK) showed that most respondents used triple therapies of oral antibiotics, steroid nasal spray, and saline irrigations to some extent, “MMT” for CRS seems to vary greatly among consultants and frequently does not reflect the recent guidelines. 9 The other study of American Rhinologic Society (ARS) member survey on “MMT” for CRS showed that MMT is most commonly used by the majority of respondents included oral antibiotics, nasal steroids, nasal irrigations, oral steroids, and allergy testing. 8 Similar studies have not been conducted in China regarding MMT prescribing habits. The purpose of our study is to determine the clinical practice patterns of MMT for CRS by Chinese otolaryngologists.
Patients and Methods
This study consisted of an anonymous, web-based survey to practicing otolaryngologists. This anonymous nationwide survey (Rhinocare Survey) was conducted through an online survey program (www.wjx.cn) and was electronically distributed to all active members of the Chinese Otolaryngology-Head and Neck Surgeons Alliance by sending Weixin pushed message. The members received the message through the Weixin groups. When the member received and read the follow-up Weixin pushed message, then the message was considered as successfully sent. The survey results were collected through an online survey program. The questionnaire was a 20-item single-choice questionnaire. The design of our questionnaire was referred to the previous CRS guidelines (Table 1). 1 -7 The study was performed over a 1-month period (November 24 to December 24, 2016). A cover letter disclosed the study’s goal of characterizing prescribing habits of MMT of CRS among Chinese otolaryngologists.
Maximal Medical Therapy Defined by Published Gudelines.
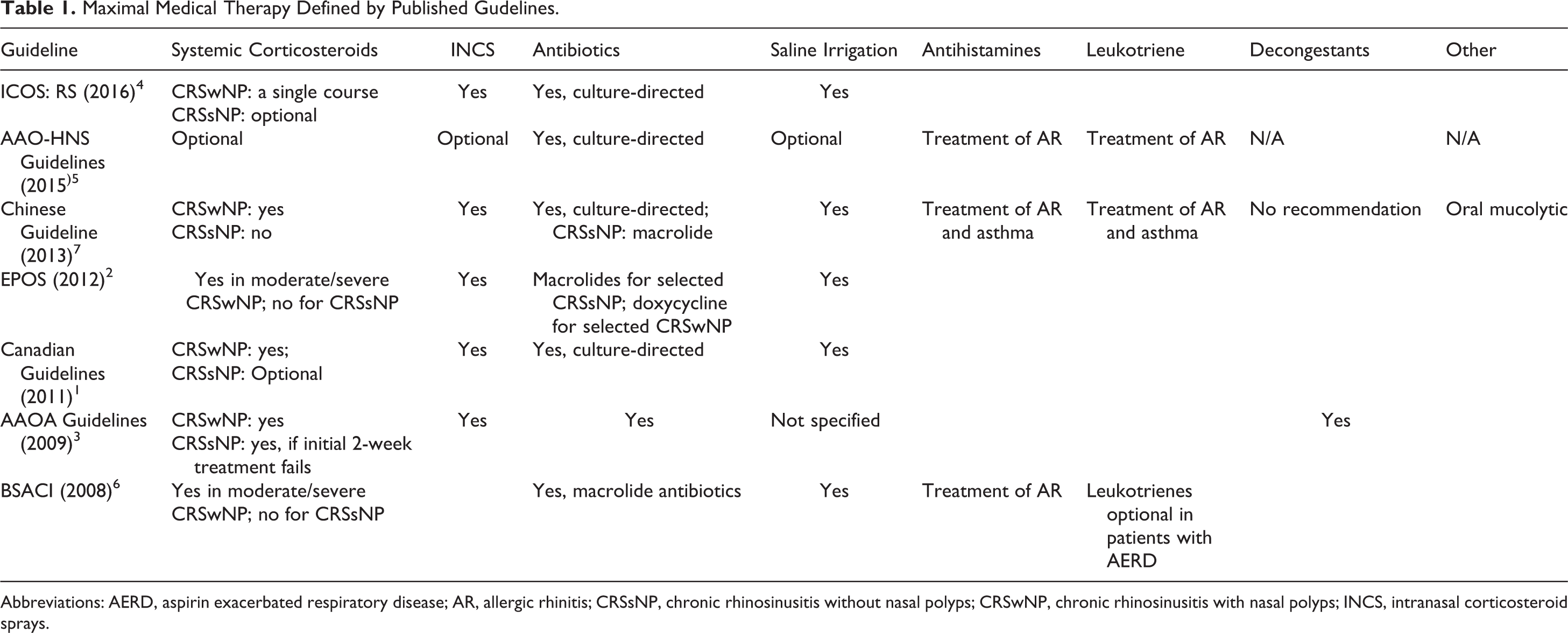
Abbreviations: AERD, aspirin exacerbated respiratory disease; AR, allergic rhinitis; CRSsNP, chronic rhinosinusitis without nasal polyps; CRSwNP, chronic rhinosinusitis with nasal polyps; INCS, intranasal corticosteroid sprays.
In terms of the answer choices, “always” was defined as 100% of the time, “often” as >70% of the time, “sometimes” as 30% to 70% of the time, “infrequent” was defined as <30% of the time, and “never” was defined as 0%. Percentages of each response were calculated on the basis of the number of respondents for each question. The method was prescribed in our previous survey study. 10
Results
Demographics of Respondents
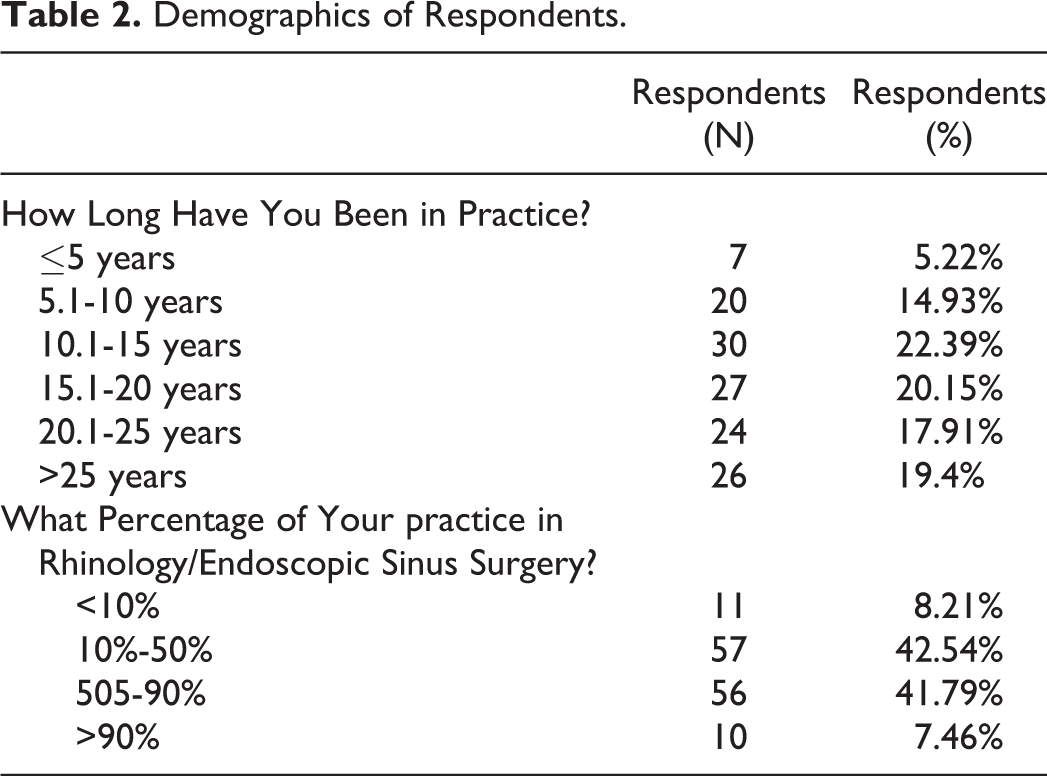
A total of 500 questionnaires were sent. One hundred thirty-four were returned, with a response rate of 26.8%. Demographics of respondents are summarized in Table 2. Of respondents, 22.39% and 20.15% had been in practice between 10.1 and 15.1 years and 15.1 and 20 years, respectively. Fifty-six (41.79%) and 10 (7.46%) respondents stated that 50% to 90% and >90% of their practice was rhinology based, respectively (Table 2).
Demographics of Respondents.
The Frequency of Use of MMT in CRS
Oral therapies
Oral corticosteroids were not commonly prescribed, with 21.64% respondents, stating that they “never” prescribed these medications. Oral antibiotics were commonly prescribed, over one-third of respondents would often (34.33%) or sometimes (34.33%) prescribe oral antibiotics, whereas 18.66% always prescribe oral antibiotics.
Over one-third of respondents would often (35.07%) or sometimes (39.55%) prescribe oral antihistamines. The use of oral antileukotriene agents for CRS varies: 35 (26.1%), 36 (26.87%%), 30 (22.39%), 27 (20.15%) prescribe oral antileukotriene often, sometimes, infrequently, and never, respectively.
Oral mucolytics were commonly prescribed, over one-third of respondents would always (52, 38.31%) or often (54, 40.3%) prescribe oral mucolytics. Nearly half of the respondents would often (62, 46.27%) prescribe oral Chinese herbals.
Topical therapies
Intranasal corticosteroid sprays were commonly prescribed, over 90% of respondents (91.5%) would always or often prescribe INCS. Nasal saline irrigations would be “always” or “often” prescribed by 47 (35.07%) or 60 (44.78%) respondents, respectively. The use of nasal antihistamines and topical decongestants varied greatly (Table 3).
Frequency of Use of Maximal Medical Therapy in CRS.
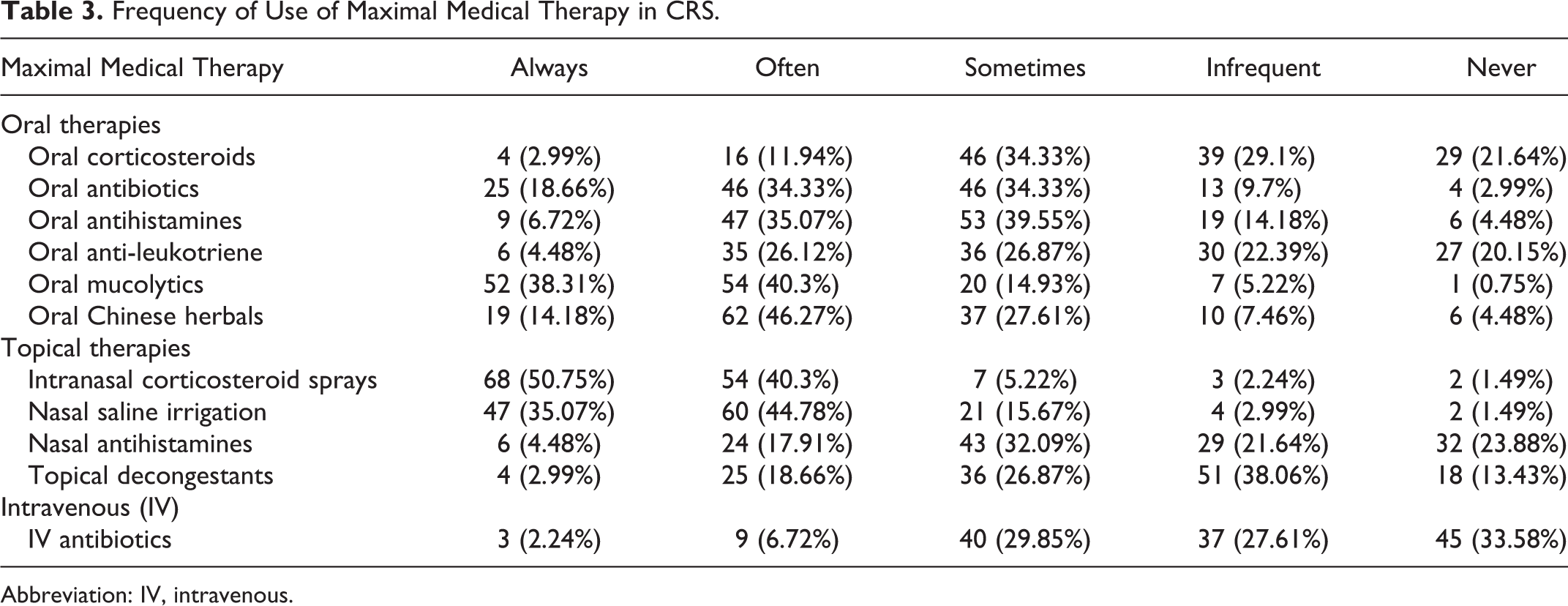
Abbreviation: IV, intravenous.
Intravenous therapies
Intravenous (IV) antibiotics were not commonly recommended for treatment of CRS, with 2.24% or 6.72% of respondents would always or often prescribe IV antibiotics. For empirical usage of oral antibiotics, macrolides were the most commonly prescribed agents by 51.49% of consultants. Cephalosporins and penicillins were prescribed by 35.07% and 10.45% of respondents, respectively (Figure 1). The use of culture-directed antibiotics was not commonly recommended by the majority of the respondents, with 33.58% and 29.85%, stated that they would “Never” or “Infrequent” prescribed those (Figure 2).
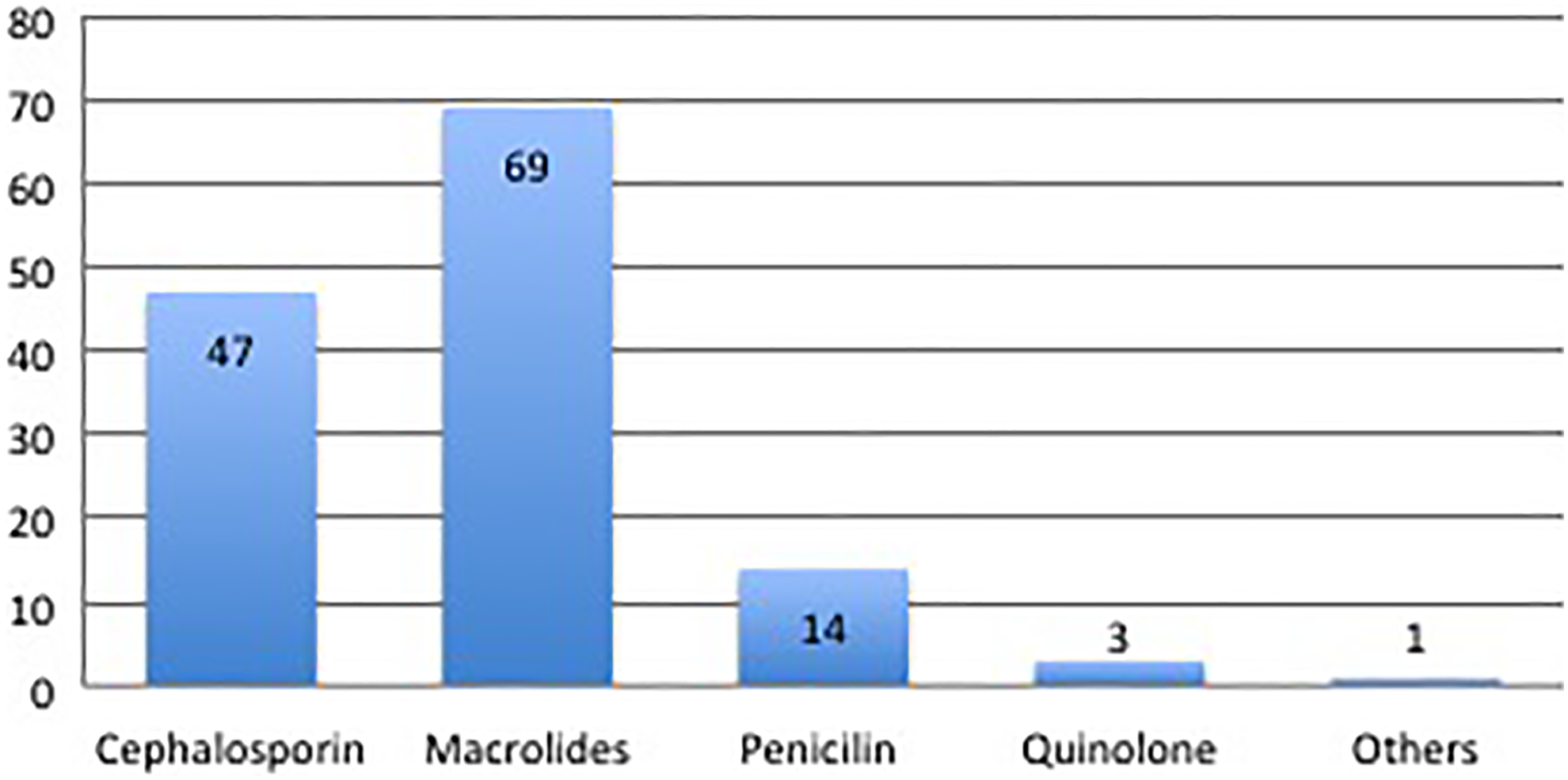
Type of antibiotic prescribed.
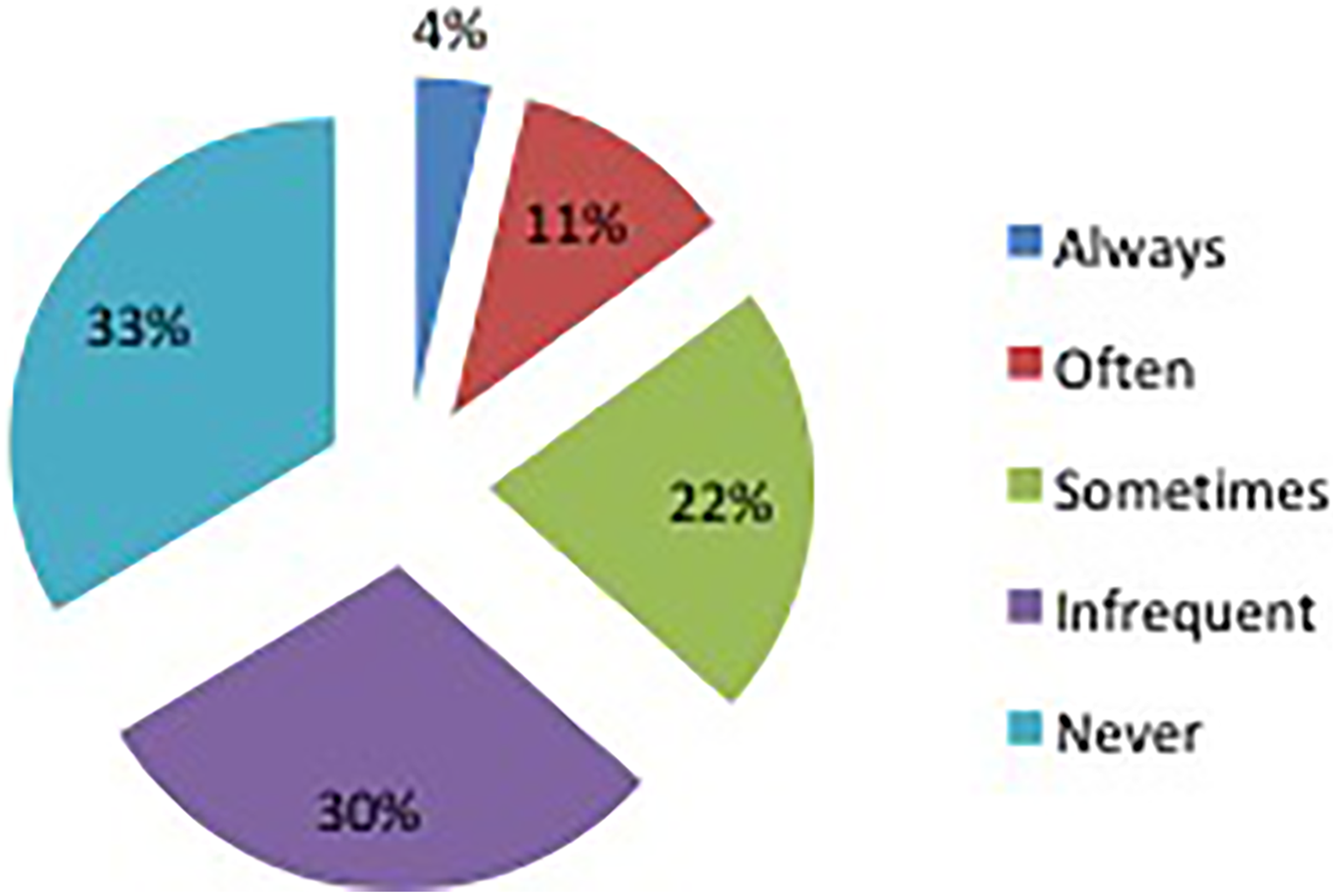
Culture directed antibiotic usage.
Length of Medication
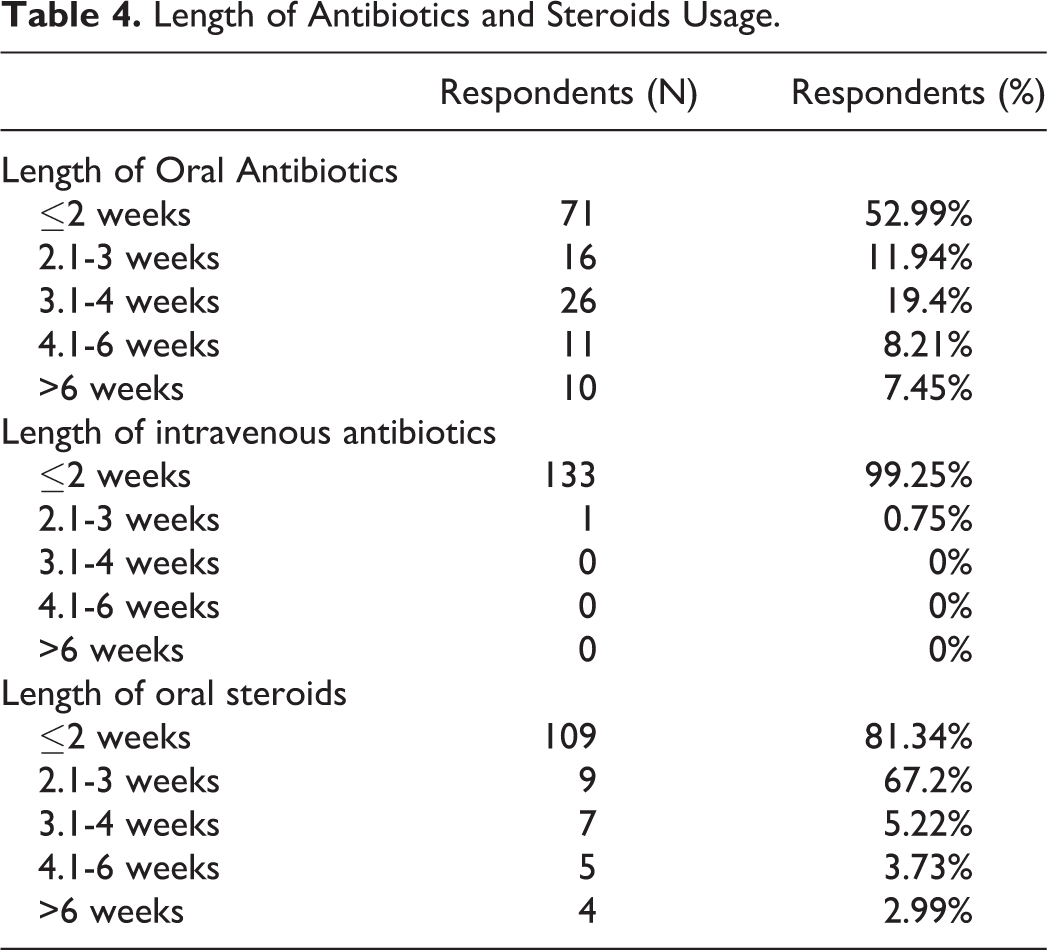
Regarding the length of oral antibiotics before surgery, 71 (52.99%) respondents stated that the length of oral antibiotics was less than 2 weeks (Table 4). Nearly most respondents (133, 99.25% and 109, 81.34%) stated that the length of IV antibiotics and oral steroids were less than 2 weeks (Table 3).
Length of Antibiotics and Steroids Usage.
Regarding the duration of MMT before consideration of surgical intervention, 33.58% of respondents would consider surgery 3 to 6 months after undergoing MMT, the majority (62.69%) would wait less than 3 months. The remaining 5% of respondents would treat medically for longer than 6 months before considering surgery (Figure 3).
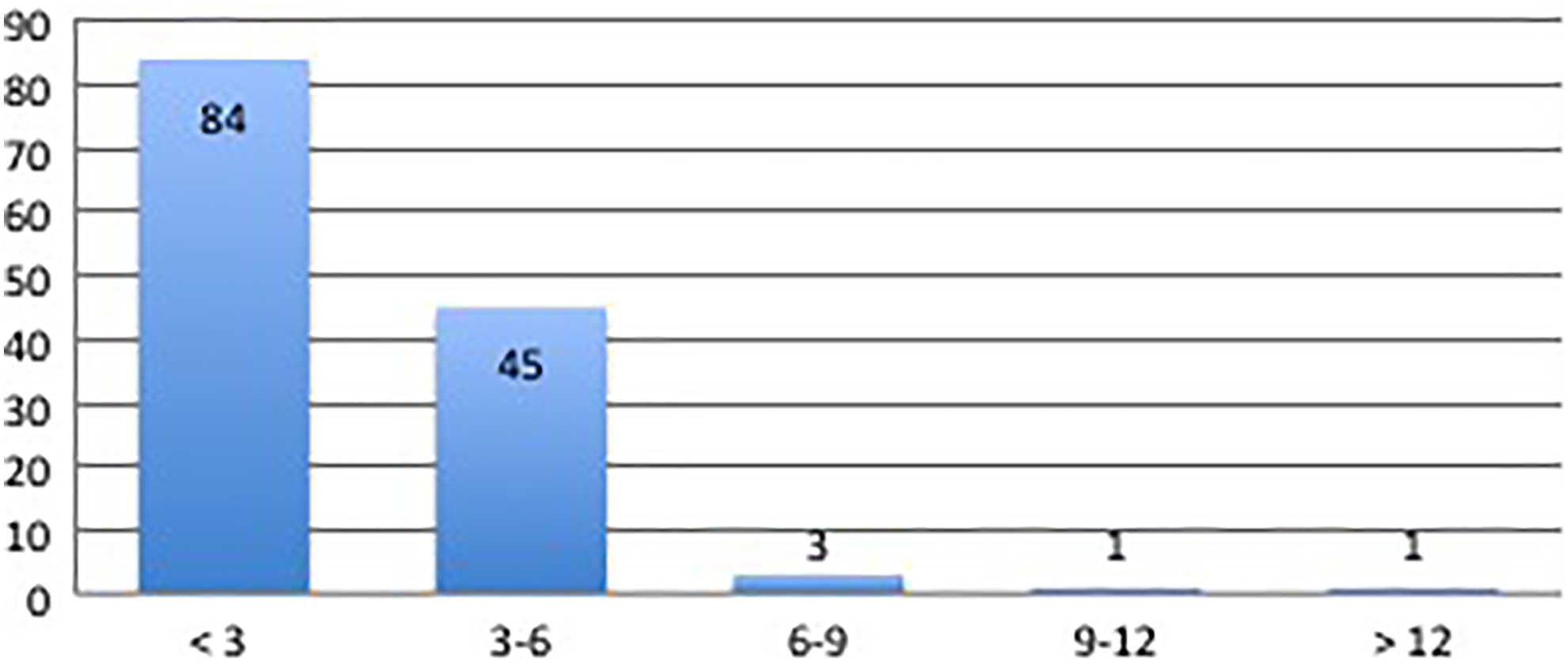
Length of maximal medical therapy.
The majority (113, 84.3%) of respondents would “always” order pretreatment computed tomography (CT) scan for the patients who were considered surgical candidates (Figure 4). None of the consultants would “Never” order a pretreatment CT scan for patients who were considered for surgical intervention (Figure 4).
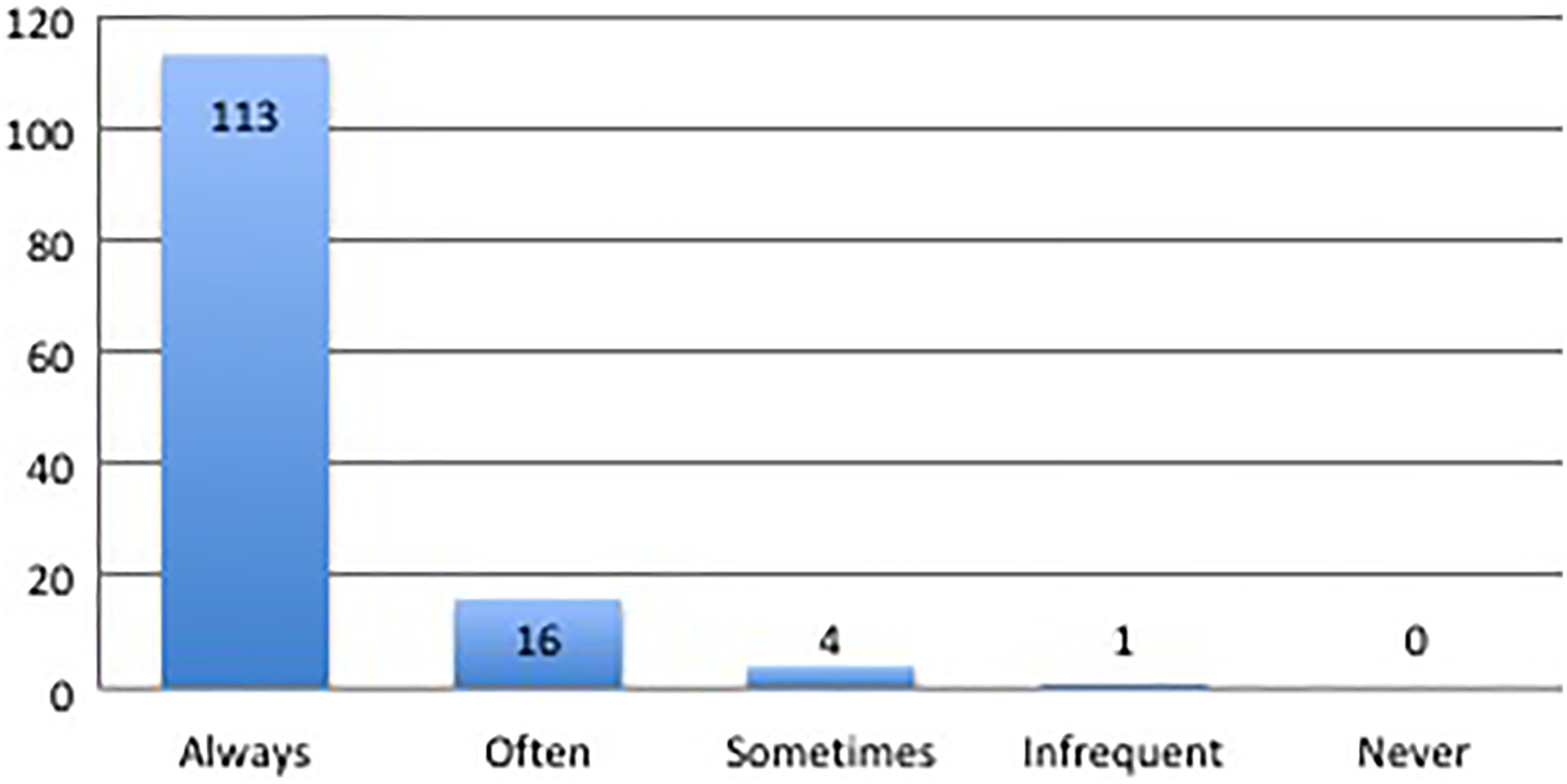
Use of preoperative CT scans. CT indicates computed tomography.
Discussion
This study has characterized the MMT prescribing habits of Chinese Otolaryngologist for CRS. The 26.8% response rate, which is similar to previous survey studies of American and English Otolaryngologists, provides MMT prescribing habits for CRS. 8,9 Our results showed that INCS, oral antibiotics, oral mucolytics, nasal saline irrigation, and oral Chinese herbals are most commonly prescribed by a majority of Chinese otolaryngologists for MMT of CRS. The use of decongestants, oral antileukotriene, and nasal antihistamines was generally limited. The results demonstrate the significant variability in prescribing habits according to CRS guidelines. The grade of evidence of MMT is low, leading to weak strength of recommendation, may be the reason for wide variety of prescribing habits observed in this study.
On the other hand, regarding the length of MMT, CRS guidelines recommendations diverge. American CRS guidelines recommend that a trial of 3 to 4 weeks of MMT should be considered as the minimum. 4 European Position Paper on Rhinosinusitis and Nasal Polyps 2012 (EPOS 2012) and 2013 Chinese CRS guideline recommended that a trial of 12 weeks of MMT should be considered as the maximal. 2,7 Our results revealed that 33.58% of respondents would consider sinus surgery 3 to 6 months after undergoing MMT, the majority (62.69%) would wait less than 3 months. The remaining 5% of respondent would treat medically for longer than 6 months. Our results indicate the length of MMT was influenced mainly by personal clinical experiences rather than evidence in the literature.
Most CRS guidelines or consensus documents stated that INCS are highly recommended as part of MMT for CRS. Ear Nose Throat (ENT) UK survey and ARS survey revealed that 61% and 41.6% of ENT consultants always prescribe INCS as part of MMT for CRS, respectively. 8,9 These findings were echoed in our survey study that we found that 50.75% of respondents would always prescribe INCS in the treatment of CRS. Our survey’s results are consistent with the previous 2 survey studies, which reflect recent CRS guidelines and consensus.
Of note, our results showed that 33.58% and 29.85% of respondents would “never” and “infrequent” use the culture-directed antibiotics while only 3.73% of respondents would “always” use the culture-directed antibiotics. Our results didn’t reflect the most of CRS guidelines or consensus documents, especially 2013 Chinese CRS guideline in that aspect. 7 We speculated that the main reason that culture-directed antibiotics are less commonly used by Chinese otolaryngologists is because the physicians prefer the empirical usage of oral antibiotics.
EPOS 2012 and 2013 Chinese CRS guideline recommended the use of long-term oral macrolides antibiotic therapy longer than 12 weeks. 2,7 Our results showed that the majority (51.49%) of respondents prescribed oral macrolides antibiotic for CRS. Interestingly, there were only 7.46% of respondents who stated that they would prescribe longer than 6 weeks-course of oral antibiotics. Taken together, short-term oral antibiotics, including macrolides, were prescribed by the majority of Chinese otolaryngologists. Although, the current trials have inconsistent findings on the effect of macrolide for CRS. Our systematic review and meta-analysis revealed adding oral clarithromycin to topical nasal steroid spray with or without saline irrigation may achieve better effects than topical nasal steroid spray with or without saline irrigation alone, without increasing the risk of adverse events (unpublished data).
One unique finding of our study is the Chinese herbals are one of the very commonly prescribed medicines for MMT of CRS. We should point out that nearly half of the respondents in our study often (62, 46.27%) prescribe oral Chinese herbals. With Chinese CRS guideline recommendations (Chinese herbals is optional) in mind, 7 it is not surprising that oral Chinese herbals are commonly prescribed by a majority of Chinese otolaryngologist for MMT of CRS. Cochrane systematic review showed that Chinese herbals may shorten the symptomatic phase in common cold patients. However, because of the lack of high-quality clinical trials, the authors were unable to recommend any kind of Chinese herbal preparation for the common cold and CRS. 11
One limitation of this study is that we did not investigate MMT for clinical phenotype separately (ie, CRS with and without nasal polyps). This study also failed to investigate the practice type of respondents (academic vs private practice). Additionally, the survey response rate (26.8%) of our study was low, but this is often a function of web-based online surveys programs. Similar surveys on MMT for CRS have ranged from 26.3% to 43%.
Conclusion
Our study demonstrates that current practice patterns of maximal medical therapies among otolaryngologists are not uniformly based on evidence-based outcomes research. Intranasal corticosteroid sprays, oral antibiotics, oral mucolytics, nasal saline irrigation, and oral Chinese herbals are the most commonly prescribed agents by Chinese otolaryngologists as part of maximal medical treatment for CRS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Natural Science Foundation of China (No. 81271063 and 81500770), Beijing Municipal Administration of Hospitals’ “Dengfeng” (DFL20150202) and “Qingmiao (Youth)” (QML20160201) Program, the priming scientific research foundation for junior researcher (2016-YJJ-BJRC-003) and clinical Medicine Development of Special Funding Support from Beijing Tongren Hospital, Capital Medical University (No.trzdyxy201702).