
Abstract
Objective:
Chronic rhinosinusitis (CRS) is an inflammatory disease of the paranasal sinuses and mucosa. Topical nasal corticosteroids are a mainstay treatment for CRS by reducing sinonasal inflammation and improving mucociliary clearance. However, topical corticosteroids have limited paranasal distribution, and patient response to treatment has been variable in randomized controlled trials (RCT). Thus, there is significant interest in evaluating the efficacy of nasal steroids delivered by nasal irrigation in order to improve penetration and absorption of topical steroids into the sinonasal mucosa. In this review, we discuss the use of off-label nasal steroid irrigations in the management of CRS.
Methods:
A review of clinical trials evaluating the use of nasal steroid irrigations for CRS in the PubMed electronic database was performed.
Results:
Of the 12 clinical studies identified, 10 evaluated budesonide irrigations while the remaining 2 focused on mometasone. The overwhelming majority of studies for both budesonide and mometasone supported the use of nasal irrigations with corticosteroids over nasal corticosteroid sprays alone. However, the heterogeneity in study design, patient cohort, and volume of steroid irrigation limit the interpretations of these studies.
Conclusions:
Nasal irrigation with corticosteroids is beneficial and safe for the treatment of CRS. Future RCTs controlling for type of surgical intervention, CRS pheno- and endo-type, as well as dosing and duration of nasal corticosteroid irrigations are warranted.
Keywords
Introduction
Inflammation of the paranasal sinuses and sinonasal mucosa is the hallmark of chronic rhinosinusitis (CRS). 1 -5 Chronic rhinosinusitis affects up to 16% of the US population and is associated with a significant personal and public health burden. 6,7 Patients with CRS can have severely impaired quality of life that is comparable to or even worse than that of patients with chronic pulmonary or cardiac diseases. 8 -10 Furthermore, due to increased medical visits, prescription medications, and surgeries as well decreased work productivity, the annual direct and indirect costs of CRS in the United States exceeds US$20 billion. 11,12
Because of the chronic nature of the disease, medical therapy for CRS is focused on symptomatic management. Current first-line therapies include antibiotics, oral and topical nasal corticosteroids, and saline irrigations with the goal of reducing mucosal inflammation, bacterial colonization, and host response to environmental triggers to improve overall sinonasal anatomy and function. 13
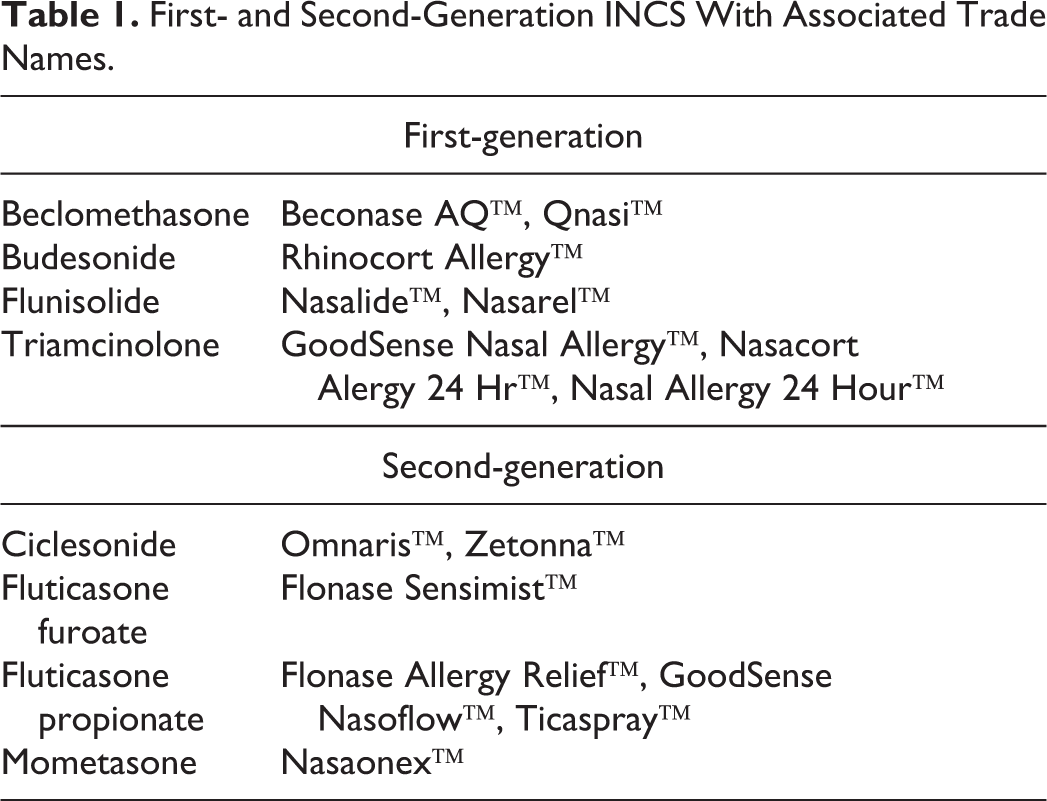
Steroids are the mainstay treatment for CRS, and the use of intranasal corticosteroids (INCS) is widely recommended (Table 1). While many patients experience symptomatic relief from systemic corticosteroids, due to major side effects such as hypothalamic–pituitary–adrenal (HPA) axis suppression, mood disturbance, and hyperglycemia, long-term use of oral corticosteroids for CRS is avoided. Intranasal corticosteroids exert an anti-inflammatory effect on sinonasal mucosa by inhibiting recruitment of inflammatory cells, upregulating anti-inflammatory genes, such as interleukin-10, and inhibiting proinflammatory genes and mediators, such as nuclear factor-kappa B. 13 -15
First- and Second-Generation INCS With Associated Trade Names.
To date, there is no consensus regarding the best route of delivery for INCS, whether by nasal spray alone or large-volume irrigations. The ability of particles to penetrate and be absorbed by the sinonasal mucosa is dependent on the size of the sinus ostia as well as the size and volume flow rate of the particle matter themselves. Studies have shown that the ideal size of topical nasal particles is between 5 and 10 µm as particles less than 5 µm enter the lungs directly while those larger than 10 µm remain in the anterior nasal vestibule. 16,17 While nasal sprays have gained increasing popularity due to their ease of use and availability, the penetration of nasal sprays to the sinonasal cavities is limited by the size and clearance of the generated droplets. The average droplet size generated by nasal sprays ranges from 50 to 70 μm. Furthermore, over half of the nasal spray is eliminated from the sinus cavities within 15 minutes with negligible activity observed within 6 hours of adminstration. 18 As a result of these characteristics, the amount of nasal spray delivered to the paranasal sinuses accounts for less than 1% of the total amount of spray retained within the nasal cavity. 19 While nebulizers that deliver topical nasal steroids in a mist form may allow for more penetration into the posterior nasal cavity and reduce clearance time, data to support their efficacy are limited. 20
Large volume, low pressure nasal irrigations have emerged as an important adjunct in the treatment of CRS. In addition to providing symptomatic relief, nasal irrigations with INCS are thought to improve the distribution of topical steroids throughout the sinonasal cavity and facilitate increased removal of mucin and bacterial biofilms. In this review, the most recent literature regarding the off-label use of topical corticosteroid nasal irrigations for CRS with a focus on budesonide and mometasone furoate are presented.
Budesonide Nasal Irrigation
Budesonide is a first-generation INCS, and the use of budesonide in nasal lavages has become increasingly widespread for CRS. Multiple clinical trials have been conducted evaluating the efficacy and safety of budesonide nasal irrigations for CRS patients with and without nasal polyps.
In a double-blind placebo controlled, randomized clinical trial (RCT) by Tait et al, 21 the use of budesonide nasal irrigation was compared to saline irrigation alone. Chronic rhinosinusitis participants performed nasal daily irrigation with budesonide capsules (1.0 mg) or placebo capsules dissolved in 480 mL of isotonic saline daily for 4 weeks. The average change in sino-nasal outcomes test (SNOT-22) scores was 20.7 and 13.6 for participants randomized to the budesonide and control group, respectively, with a mean difference of 7 points in favor of the budesonide arm (95% CI: −2 to 16). Furthermore, 79% of participants in the budesonide group had a clinically meaningful reduction in SNOT-22 scores compared to 59% in the control group. When exploratory subgroup analysis was performed, a greater benefit was observed for CRS patients with no prior history of functional endoscopic sinus surgery (FESS) compared to those with prior FESS. Interestingly, only a minor improvement in SNOT-22 scores was observed for CRS patients with nasal polyps (CRSwNP) who received budesonide.
In another study, Snidvongs et al 22 examined the efficacy of budesonide nasal irrigation for CRS patients post-FESS. Patients with CRS who underwent FESS after failed maximal medical therapy were randomized to perform daily irrigations with either budesonide (1 mg) or betamethasone (1 mg) dissolved in a 240 mL saline lavage for 3 consecutive months; the dose of budesonide or betamethasone was then tapered off. Compared to baseline, patients receiving budesonide or betamethasone had improved patient-reported post-symptom scores (2.6 ± 1.1 vs 1.2 ± 1.0; P < .001), SNOT-22 scores (2.2 ± 1.1 vs 1.0 ± 0.8; P > .001), and Lund-Kennedy endoscopy scores (6.7 ± 3.0 vs 2.5 ± 2.0; P < .001). In addition, patients with high tissue eosinophilia (>10/high power field) showed significant improvement on mean symptom scores (1.9 ± 1.4 vs 1.1 ± 1.0, P = .04), mean SNOT-22 scores (1.6 ± 1.3 vs 1.0 ± 0.8, P = .03), and mean Lund-Kennedy endoscopy scores (5.12 ± 3.4 vs 3.06 ± 3.0, P = .01).
Rawal et al, 23 however, performed a study comparing budesonide nasal irrigation to saline irrigation alone in CRSwNP patients post-FESS and found no significant differences in objective or subjective outcome measures. In their study, CRSwNP patients who underwent FESS were instructed to perform 60 mL irrigations twice daily with either saline alone or saline with 1 mg of budesonide. Patients were then evaluated at 3 different time intervals: 1 to 2 weeks, 3 to 8 weeks, and 3 to 6 months post-FESS. At all 3 study time points, there was no statistically significant difference in the Rhinosinusitis Outcomes Measurement Test, SNOT-22, Rhinosinusitis Disability Index, and University of Pennsylvania Smell identification Test scores.
For refractory CRS patients, defined by the European Position Paper on Rhinosinusitis and Nasal Polyps 2012 24 as persistent symptoms despite surgery, corticosteroids, and antibiotics, Kosugi et al 25 reported that daily use of budesonide (1 mg) dissolved in 500 mL of nasal saline for 3 months improved mean SNOT-22 and Lund-Kennedy endoscopy scores in 75% of study patients. Compared to baseline, SNOT-22 and Lund-Kennedy scores showed significant improvement by the end of 3 months of treatment (50.2 ± 19.3 vs 29.6 ± 20.4; P = .006 and 8.8 ± 3.3 vs 5.1 ± 4.4; P = .01, respectively).
CRS patients with nasal polyps patients with steroid dependent asthma were also shown by Kang et al 26 to derive significant clinical improvement following the use of budesonide nasal irrigations, as reflected by improvements in SNOT-22 and Lund-Kennedy endoscopy scores. 26 Participants performed twice daily irrigations of budesonide (0.5 mg/2 mL of budesonide respules dissolved in 250 mL of saline) for 6 months. At the completion of the study, budesonide nasal irrigations not only improved SNOT-22 and Lund-Kennedy endoscopy scores but also reduced the concomitant intake of oral steroids (397.8 ± 97.6 mg vs 72.7 ± 99.7 mg; P < .001). Furthermore, 50% of patients did not require continued oral corticosteroid treatment after completing budesonide irrigations.
In a retrospective study by Jang et al, 27 post-FESS patients who had a lapse of at least one month of budesonide irrigation postoperatively were restarted on budesonide irrigations (0.5 mg/3 ounces of isotonic saline) twice daily. The median duration of therapy was 13.4 months (range 1-80 months). Overall, there was no statistical improvement in SNOT-20 scores following budesonide irrigations. However, on subgroup analysis, patients with eosinophilic CRS had improvement in SNOT-20 scores and Lund Kennedy endoscopy scores following resumption of budesonide nasal irrigation (12.5 ±10.4 vs 15.1 ± 12.1; P < .05 and 11.7 ±11.6 vs 15.3 ± 13.0; P = .04, respectively). Furthermore, patients with Samter triad also demonstrated reduction in SNOT-20 scores following use of budesonide irrigation (14.9 ± 8.4 vs 21 ± 10.3; P = .04) when compared to not using irrigations. Allergic fungal sinusitis patients, however, showed no difference in SNOT-20 or Lund Kennedy endoscopy scores (12.3 ± 7.4 vs 8.7 ±7.2; P = .13 and 2.9 ± 2.3 vs 2.5 ± 2.6; P = .6, respectively). Rotenberg et al 28 performed a placebo-controlled randomized clinical trial for Samter triad patients and reported no difference in budesonide irrigation compared to placebo for symptom control after 1 year of treatment. All patients enrolled had undergone FESS and were randomized post-surgery to saline irrigation alone, saline irrigation with generic budesonide nasal spray (256 ug dose), or budesonide irrigation (2 mL of 0.5 mg/mL) alone. There was no difference in SNOT-22 (42.5 vs 47.9 vs 42.2), Lund Kennedy endoscopy (3.7, 4.1, 4.4), or Lund McKay scores (11.8, 12.7, 13.4) among the 3 groups (P > .05) but there was improvement compared to baseline (P < .0167) within each group. 28
Budesonide irrigation and HPA axis function
While systemic corticosteroids can cause suppression of the HPA axis with long-term use, multiple studies have shown no evidence of adrenal suppression with either short- or long-term use of budesonide nasal irrigation. Sachanandani et al 29 performed an open-label prospective study to evaluate adrenal function in CRS patients using budesonide lavage (0.25 mg/5 mL) once daily for 4 weeks and found no significant difference in mean cortisol levels pre- and posttreatment (33.9 μg/dL, 95% CI: 30.50-37.28 vs 35.2 μg/dL, 95% CI: 30.66-39.70, respectively). In a slightly longer prospective study of CRSwNP patients by Welch et al, 30 10 patients performed 0.5 mg/240 mL of budesonide lavage twice daily for 6 weeks and had serum cortisol and 24-hour urinary cortisol levels collected at baseline and at follow-up. There was no significant difference in mean cortisol levels pre- and postintervention (9.8 ± 5.4 μg/dL at baseline and 12.8 ± 3.5 μg/dL, respectively). In addition, no significant decrease in urinary cortisol levels was observed. In another study, Smith et al 31 examined the effect of at least 12 months of budesonide nasal irrigation (2 mg) on HPA axis function. Nineteen (54%) of the 35 patients in the study had ACTH stimulation testing performed and none had abnormal values. In a cross-sectional, retrospective case series of 48 postsurgical CRS patients who performed long-term budesonide irrigation (mean use 22 months, range 6-66 months), Soudry et al 32 found that 11 (23%) of the patients had abnormally low stimulated cortisol levels. However, all 11 patients were asymptomatic. Furthermore, the concomitant use of steroid nasal sprays or pulmonary inhalers was associated with an increased risk of subclinical HPA axis suppression (odds ratio [OR], 30.4; 95% CI: 1.57-588; P = .024).
Budesonide Irrigations and IOP
Although the data are limited on the effect of budesonide nasal irrigations on intraocular pressure (IOP) and cataracts, no study to date has shown an increase in either IOP or formation of posterior subcapsular cataract. Seiberling et al 33 compared IOP in 2 groups of CRSwNP patients. The first group used budesonide irrigations for at least 1 month during which time they had their IOP measured once while the second group had their IOP measured before and after at least 4 weeks of budesonide irrigation use. For both groups, the total daily amount of budesonide was 0.5 mg. In group 1, the mean duration use of budesonide was 6.9 months (range 1-22 months) and only 1 patient had an elevated IOP (>21 mm Hg) but was found to have normal eye examination on subsequent ophthalmologic follow-up. Patients in the second group had a mean use of budesonide of 5.89 weeks (range 4-8 weeks) and none had an elevated IOP. In a larger study by Soudry et al, 32 46 postsurgical CRS patients who performed budesonide nasal irrigations (mean daily dose of 0.75 mg) had their IOP measured and all were within normal limits (mean 16 mm Hg, range 13-18). Similarly, Rotenberg et al 28 found no effect on IOP in post-surgical CRSwNP patients with Samter triad following 12 months of daily budesonide (1 mg) irrigation use. While the use of inhalant/nasal corticosteroid has been reported to be associated with an increased risk of central serous chorioretinopathy (CSC), 34 none of these studies examined or reported the incidence of CSC. However, this risk should be considered in patients presenting with decreased vision following initiation with corticosteroid therapy.
Mometasone Nasal Irrigation
Mometasone furoate is a second-generation INCS that has increased lipophilicity and more rapid hepatic metabolism compared to budesonide. Thus, compared to budesonide, mometasone has more favorable pharmacokinetics and significantly less systemic absorption (<0.1% vs 34%, respectively) and less systemic bioavailability (15% vs 39%). 35,36 In a double-blind placebo-controlled RCT by Harvey et al 37 evaluating the efficacy of mometasone nasal spray versus mometasone irrigation (2 mg capsule dissolved in 240 mL isotonic saline) in CRS patients post-FESS, both groups had improvement in subjective and objective outcome measures compared to baseline following 1 year of treatment. However, by 1 year, patients who were randomized to mometasone nasal irrigation had a greater improvement in nasal blockage using the visual analogue scale (−69.91 ± 29.37 vs −36.12 ± 42.94; P = .029), Lund-Mackay scores (−12.07 ± 4.43 vs −7.39 ± 6.94; P = .031), and modified Lund-Kennedy scores (7.33 ±11.55 vs 21.78 ± 23.37; P = .018). More recently, Jiramongkolchai et al 38 examined the use of mometasone nasal irrigation (2.4 mg in 240 mL) compared to mometasone nasal spray in CRS patients without nasal polyps with no history of sinus surgery in a double-blind placebo-controlled RCT. While both arms improved in SNOT-22 scores following 8 weeks of irrigation, the proportion difference was 17% in favor of the mometasone irrigation arm (95% CI: −9% to 44%).
Mometasone Nasal Irrigation and HPA axis function
Only one study has examined the effect of mometasone nasal irrigation on HPA axis function. Jiramongkolchai et al 38 evaluated the impact of 8 weeks of mometasone nasal irrigation on adrenal function in CRSwNP patients who had not undergone prior sinus surgery. There was no significant difference observed in mean serum cortisol levels before or after treatment (mean difference −0.04, 95% CI: −3.83 to 3.75). To date, no study has evaluated ocular changes in patients using mometasone lavage.
Limitations
While there have been numerous studies evaluating the off-label use of corticosteroid nasal irrigations for CRS patients, the heterogeneity of patient population, variation in steroid dosing and volume of lavage, and range in treatment duration limit the interpretation of these studies.
Improving access to the sinonasal corridor through surgery can enhance delivery of topical medications. Prior cadaveric and computational dynamic studies have shown increased delivery and absorption of topical steroids following frontal, maxillary, and sphenoid sinusotomy. 39 -41 Left unopen, the paranasal sinuses receive limited distribution of topical agents regardless of head position, delivery device, or volume. 20,42 -45 With the exception of Harvey et al, 37 the studies reviewed here did not completely describe their surgical interventions or included nonsurgical patients in their study cohort. Although sinus surgery is guided in large part by patient anatomy and underlying pathology, the efficacy of corticosteroid nasal irrigations is difficult to evaluate when the surgical status of the paranasal sinuses is not well defined.
Heterogeneity in the dosing of steroid and volume of solution as well as frequency of irrigations also limit interpretation of the studies reviewed here. Delivery of at least 100 mL has been shown to be required to adequately penetrate the sinus cavities after surgery in order to fill the existing dead space within the nasal cavity. 46 However, the studies reviewed above reported an inconsistent volume of corticosteroid irrigation, ranging anywhere from 5 to 480 mL.
Duration of therapy is another potential confounding factor for these clinical trials. Two studies showed no statistically significant improvement in patient symptoms using nasal steroid irrigations; however, patients were treated for less than 6 months in both studies. 21,23 Given the wide range in treatment duration, the optimal duration for nasal steroid irrigation use remains unclear.
Conclusion
In the management of CRS, the literature supports the use of nasal irrigation with corticosteroids for improvement of objective and subjective outcome measures. The overwhelming evidence suggests that large volume nasal irrigation with corticosteroids offers improved benefits over nasal corticosteroid spray alone. However, these findings should be kept in the context that most patients who demonstrated improvement with nasal corticosteroid irrigations had undergone previous sinus surgery. Safety studies have demonstrated that long-term use of nasal steroid irrigations is not associated with an increase in IOP or adrenal insufficiency. Nasal irrigation with corticosteroids should be considered as part of the armamentarium in the treatment of CRS. Future larger RCTs controlling for surgical intervention, CRS pheno- and endo-type as well as volume, type, and dosing of corticosteroids will help establish nasal corticosteroid irrigations as the standard of care for CRS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.