
Abstract
A case of a 32-year-old female with a known diagnosis of Turner syndrome who presented with complaints of chronic progressive right-sided facial pain and sinus pressure and who was afebrile. On physical examination, there was eye proptosis on the right and significant increased fullness in the right infraorbital and maxillary regions. Computed tomography and magnetic resonance imaging demonstrated a large expansile space-occupying lesion in the right maxillary area that histologically turned out to be a giant cell reparative granuloma. The lesion was completely removed, and of interest, the patient was followed up both clinically and on imaging for 10 years with no signs of recurrence. A discussion on this entity, as well the clinical and imaging differential diagnoses, is discussed.
A 32-year-old female with a known diagnosis of Turner syndrome presented to our institution with complaints of chronic progressive right-sided facial pain and sinus pressure and was afebrile. On physical examination, there was eye proptosis on the right and significant increased fullness in the right infraorbital and maxillary regions.
Computed tomography and magnetic resonance examinations (Figure 1) revealed a soft tissue mass centered in the right maxillary sinus. The medial portion of the mass involves the right side of the nasal structures, including the turbinates and nasal septum. There was also involvement of the right ethmoid sinuses and significant erosion of the superior wall of the right maxillary sinus with involvement of the inferior orbit. The osseous erosion of the maxilla with soft tissue extended anteriorly and to a lesser degree inferolaterally with involvement of the roots of multiple teeth of the superior alveolar ridge.
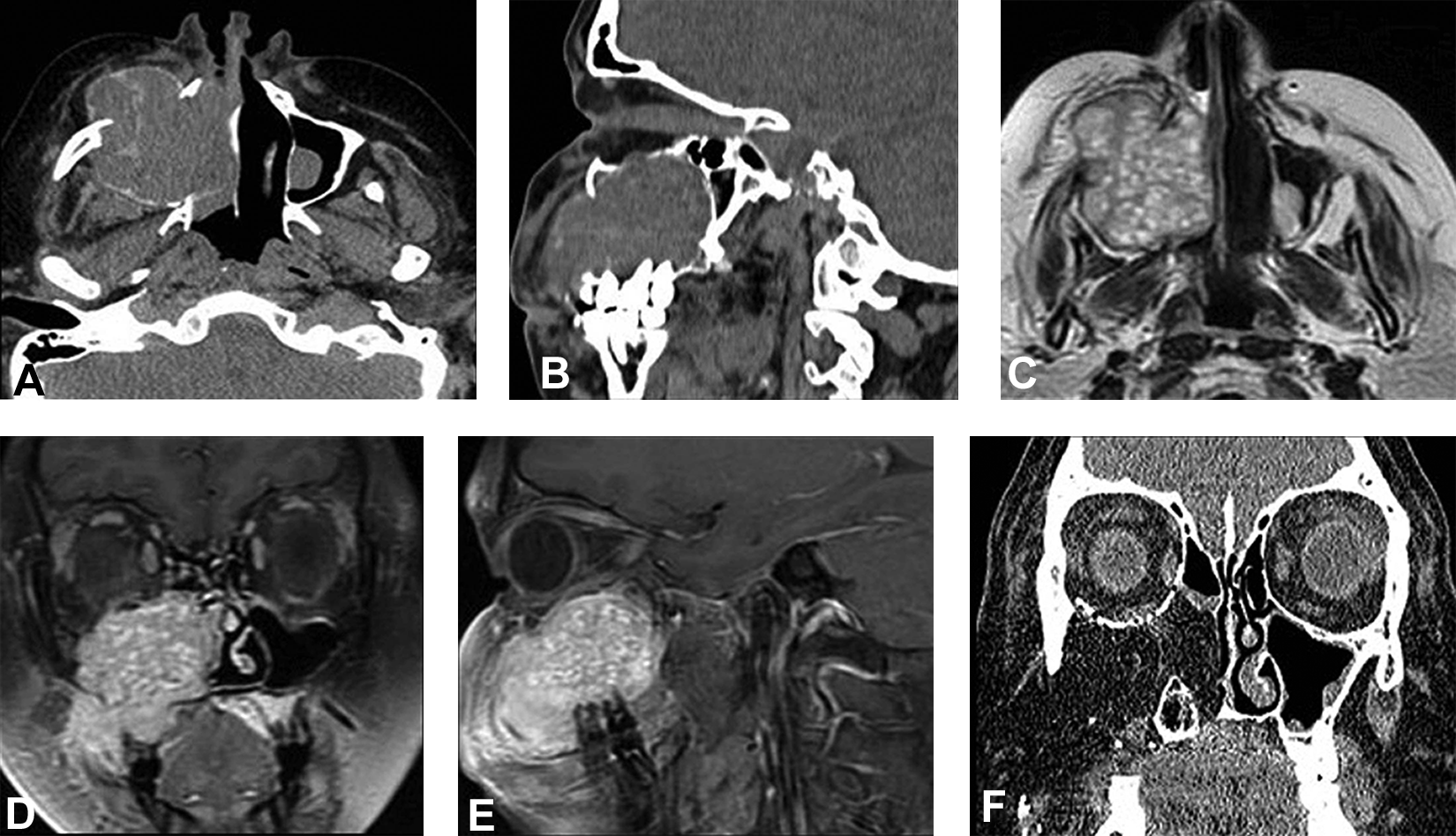
Computed tomography (A and B) axial and sagittal images revealed an expansile soft tissue mass centered in the right maxillary sinus with significant remolding of the adjacent bone. The mass extends into the nasal cavity and ethmoid sinus. Magnetic resonance imaging (C) axial T2W and (D and E) coronal and sagittal postcontrast revealed a multilobular pattern with enhancement of the soft tissue mass which extends into the nasal cavity and anterolaterally into the masticator space. Computed tomography (F) coronal image was obtained as a follow-up 10 years later after surgical resection. Fat graft placement and inferomedial reconstruction of the right orbit is noted without evidence of lesion recurrence.
Histologically, there were areas of bone trabeculae with osteoblastic activity with proliferation of osteoclast-like giant cells intermixed with cytologically benign spindle cells, scattered mitoses, and hemorrhage foci. The changes were consistent with a giant cell reparative granuloma.
Discussion
Diagnostic considerations for a soft tissue mass predominantly within the maxillary sinus with osseous destruction would include a malignancy, such as squamous cell carcinoma, the most common sinonasal malignancy in 80% of the cases. Fungal sinusitis, an aggressive infection in immunocompromised or debilitated patients, and non-Hodgkin’s lymphoma should also be considered, as well as granulomatosis, such as sarcoidosis. 1
Given our female patient’s young age and otherwise good health, most of the above differential considerations are not a good fit. The fact that the mass does involve nasal structures could implicate a carcinoma in inverted papilloma; however, the patient’s young age and female gender may argue against this possibility.
On biopsy, the mass in our case turned out to be a giant cell granuloma, formally called giant cell reparative granuloma, which is a distinct entity from a giant cell tumor and in fact is not considered a tumor, but a reactive process, originally thought to be a response to trauma. 2 Post-traumatic etiology, however, cannot be demonstrated consistently; therefore, the term reparative is omitted. 3,4 Giant cell granuloma shares close histologic characteristics with brown tumors in hyperparathyroidism. Other diagnostic considerations based upon histology include aneurysmal bone cyst, ameloblastoma, and odontogenic myxoma. 4
Giant cell granulomas occur in the second and third decades of life and have a predilection for the mandible and maxilla. 5 Other locations are in small bones of the hands and feet. Involvement of the paranasal sinuses, temporal bone, skull, spine, and other bones is rare. Giant cell granulomas are classified as central type, involving the bone, or peripheral type, involving the gingival and alveolar mucosa. Peripheral lesions tend to be pedunculated or sessile, while central lesions are endosteal and present as unilocular or multilocular expansile lesions that are divided according to clinical behavior into aggressive and nonaggressive. 6
Mandibular lesions are more common than in the maxillary area involving the portions anterior to the first molar in the mandible and anterior to the cuspids in the maxilla. 4 -6 The lesions are expansile with bone remodeling and with occasional pathological fractures. Soft tissue extension has been described with a density similar to muscle with occasional calcifications. Curettage as a management is carried out to treat well-defined localized lesions and radical surgical excision in more extensive lesions, as in our case. 3 Medical treatment as an adjunct to surgery includes steroids, calcitonin, interferon-α, and bisphosphonates. 3 Recurrence usually occurs in the first 2 years in 12.5%: 46% with curettage and 11.5% with surgical resection.
Our case was that of a very aggressive peripheral giant cell granuloma in the maxilla involving the maxilla sinus, extending into the orbit, nasal cavity, and masticator space. Interestingly, clinically and on imaging follow-up up to 10 years, there has not been evidence of lesion recurrence as in Figure 1F.
It should be noted that Noonan syndrome is a rare genetic disorder characterized by features such as short stature, hypertelorism, short neck, widely spaced nipples, and cryptorchidism. Noonan syndrome is occasionally seen with multiple giant cell lesions or so-called Noonan-like/multiple giant cell lesion syndrome. 7 In our case, the patient had a known diagnosis of Turner syndrome (a similar phenotype to Noonan syndrome) and had only one known giant cell lesion at the time of writing this case.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.