
Abstract
Asthma has been implicated as a driving force in lower airway remodeling; however, its effect on upper airway development has not been studied. Clinical disease, particularly cystic fibrosis (CF), has been associated with anatomical paranasal sinus variation, although the mechanism for these variations remains unclear. The purpose of this study was to determine whether asthma is associated with altered sinus pneumatization. Five hundred ninety-one computed tomography scans, including 303 adolescents (age 13-18) and 288 adults (age > 18), were evaluated using the Assessment of Pneumatization of the Paranasal Sinuses (APPS) instrument. The APPS score is validated for assessing anatomical variation and total sinus volume. A diagnosis of asthma was ascertained from the medical record, and patients with CF were included as a positive control group. Patients with asthma had mean APPS score of 9.66, compared to 9.85 for participants without asthma (P = .585). Subgroup analysis demonstrated similar findings among adults (P = .817) and adolescents (P = .585). Patients with a diagnosis of CF had significant sinus hypoplasia according to a mean APPS scores of 3.50 (P < .001). Sinus hypoplasia persisted in both adults (P < .001) and adolescents (P < .001) with CF. The presence of asthma is not associated with altered paranasal sinus pneumatization. In contrast, CF is associated with significantly reduced sinus pneumatization. These findings suggest that aberrant sinus pneumatization may not be a feature of asthma and that chronic mucosal respiratory disease is not a generalizable cause for altered paranasal sinus pneumatization.
Introduction
Paranasal sinus anatomy varies considerably among patients, 1 –3 and this variation has been associated with clinical disease in certain instances. 4 –8 Sinus hypoplasia has been well-documented in cystic fibrosis (CF), 4 –7 and similar sinus pneumatization patterns have been observed in primary ciliary dyskinesia and Kartagener syndrome. 8 Sphenoid aplasia has been demonstrated to occur in sickle cell anemia. 9 The mechanisms by which sinonasal or respiratory diseases account for altered paranasal sinus pneumatization remain unclear. Several theories have been suggested for this effect and include chronic sinus inflammation and infection, 10,11 genetic mechanisms, 4 –6,12,13 regional blood flow anomalies, 9,14 and increased serum erythropoietin. 9
Separately, the unified airway theory postulates that the respiratory tract consists of an integrated whole rather than a series of independent anatomic sites. 15 The pathophysiological mechanisms that affect one site may impact the entire functional unit. 15 –19 Furthermore, treatment of one site has been found to mitigate disease processes at distant anatomical airway sites. 20,21 Chronic respiratory disease, including asthma, has been shown to result in lower airway remodeling. 19,22 Previous studies of the sinonasal effects of asthma have been confined to the presence of paranasal sinus disease, particularly chronic rhinosinusitis (CRS). 23 The relationship between sinus pneumatization and asthma has not been studied and may help to elucidate clinical disease states underlying aberrant sinonasal anatomy. This in turn may have implications for the surgical management of the sinonasal manifestations of these entities.
Paranasal sinus pneumatization has been difficult to quantify and therefore has precluded the study of the relationship between clinical parameters and sinus anatomy. Sinus hypoplasia has been documented in CF using metrics that were not completely validated for use in other disease processes. 5 –7 Alternatively, sinus pneumatization has been quantified with volumetric or dimensional analysis, but these methods are typically difficult to apply to large study populations. 10,24,25 The Assessment of Pneumatization of the Paranasal Sinuses (APPS) instrument has been validated for clinician evaluation of paranasal sinus pneumatization on sinus computed tomography (CT). 26 The APPS score tracks 9 anatomic variants bilaterally (Table 1), for a comprehensive score with a possible range of 0 to 18. The APPS score correlates with total sinus volume and can be performed by clinicians in less than 1 minute. 27 This may allow for the detection of subtle differences in sinus pneumatization which require larger study populations.
APPS Score Items.
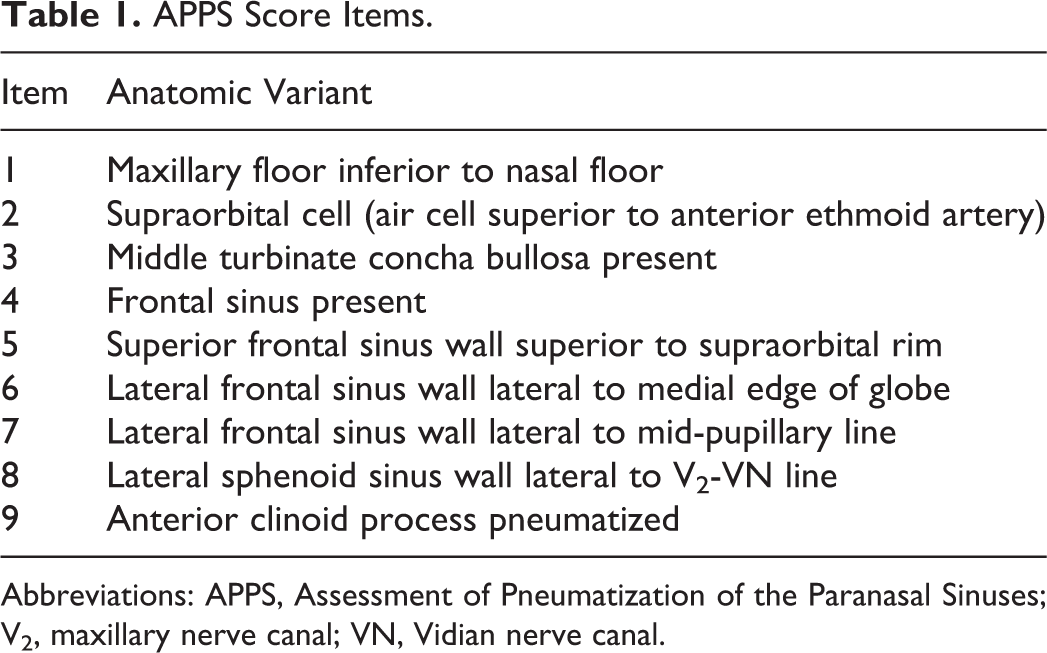
Abbreviations: APPS, Assessment of Pneumatization of the Paranasal Sinuses; V2, maxillary nerve canal; VN, Vidian nerve canal.
Methods
Paranasal sinus and maxillofacial CT scans were considered for inclusion in the study. An adolescent cohort, defined as patients aged 13 to 18 years at the time of CT acquisition, included all CT scans performed between January 1, 2010, and December 31, 2014. Patients without scans in both axial and coronal images were excluded from the study. A similarly sized cohort of adults, defined as patients older than 18 years at the date of service, included all CT scans acquired from July 6, 2015, to August 6, 2015. Sample size was estimated to be 788 patients using Cohen d method, with the assumptions of small effect size (d = 0.2), significance level of .05, and power of 0.8. All CT scans were evaluated for APPS and Lund-Mackay scores. A diagnosis of asthma or CF, as determined by the treating physician, was gathered from the medical record for each scored CT scan. Patients without a diagnosis of asthma, CF, or CRS were included in the control group. Control scans were typically acquired for the diagnostic evaluation of facial trauma or CRS without positive findings. Radiographic scoring and diagnostic information were stored in a secure, web-based Research Electronic Data Capture database (version 6.6.2; REDCap, Nashville, Tennessee) for compilation and analysis. 28
Assessment of Pneumatization of the Paranasal Sinuses and Lund-Mackay scores of individuals with asthma and CF were compared separately to controls by 2-sample independent t tests. Subgroup analyses were performed for adult and adolescent patients. P values less than .05 were considered significant. Statistical analysis was completed using SAS software (version 9.3, SAS Institute Inc, Cary, North Carolina). The institutional research board approved the study.
Results
A total of 930 participants met the inclusion criteria, of which 339 did not have usable axial and coronal images available and were therefore excluded. Ultimately, 591 participants were included in the study, with 303 adolescents and 288 adults. Demographic characteristics of the study population are shown in Table 2. Patients diagnosed with asthma were younger than controls in the overall study population (P < .001). There were no significant age differences between patients with asthma and controls within either the adult or adolescent subgroups. Patients with CF were also younger than controls in the total study population (P < .001). This also reached significance in the adult subgroup (P < .001), but not the adolescent subgroup. There were no significant gender differences between the asthma group and the control group for the total study population or within the adolescent or adult subgroups. The CF group also did not have any significant gender differences when compared to the control population for all patients or within the adolescent or adult subgroup.
Demographics of Study Population.
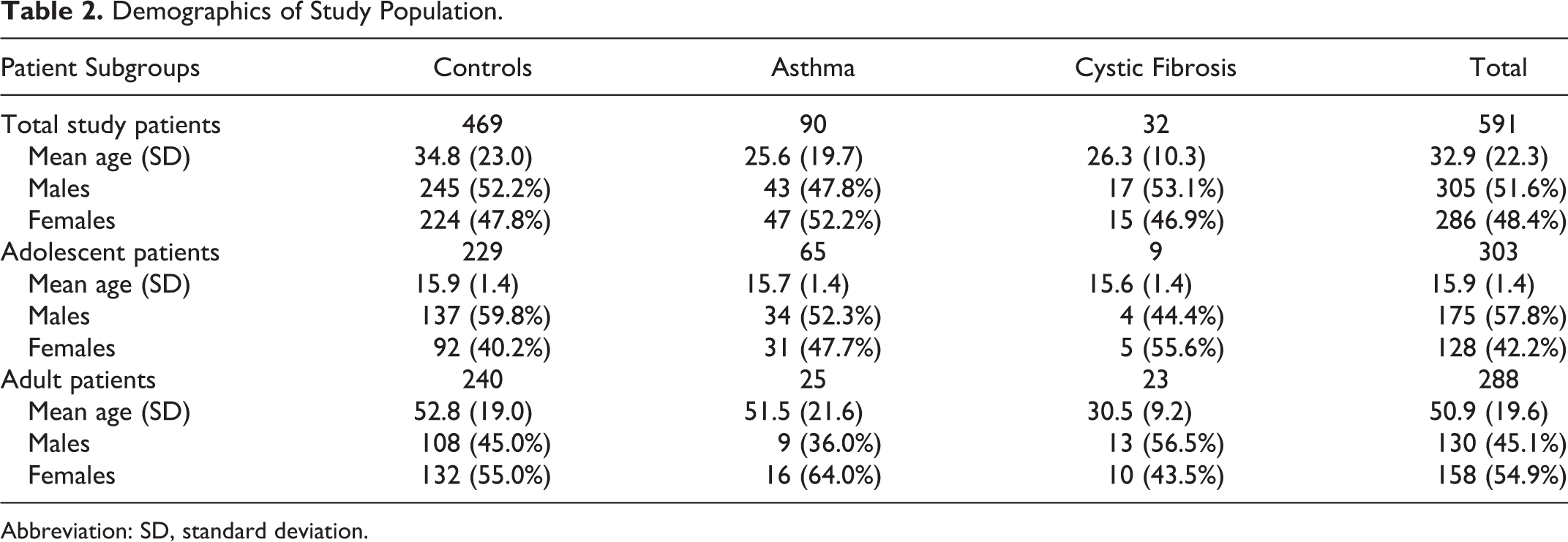
Abbreviation: SD, standard deviation.
Assessment of Pneumatization of the Paranasal Sinuses scores were not statistically different between patients with asthma and the control group, while patients with CF had lower APPS scores than controls (Table 3). These results were replicated in adolescent and adult subgroups. Asthma patients had Lund-Mackay scores that were not statistically different from healthy controls, and this was consistent in age-dependent subgroup analysis. As expected, patients with CF had a significantly higher Lund-Mackay score than the control group (Table 3). These results were also replicated in adolescent and adult subgroup analysis.
APPS and LMS Between Study Groups.
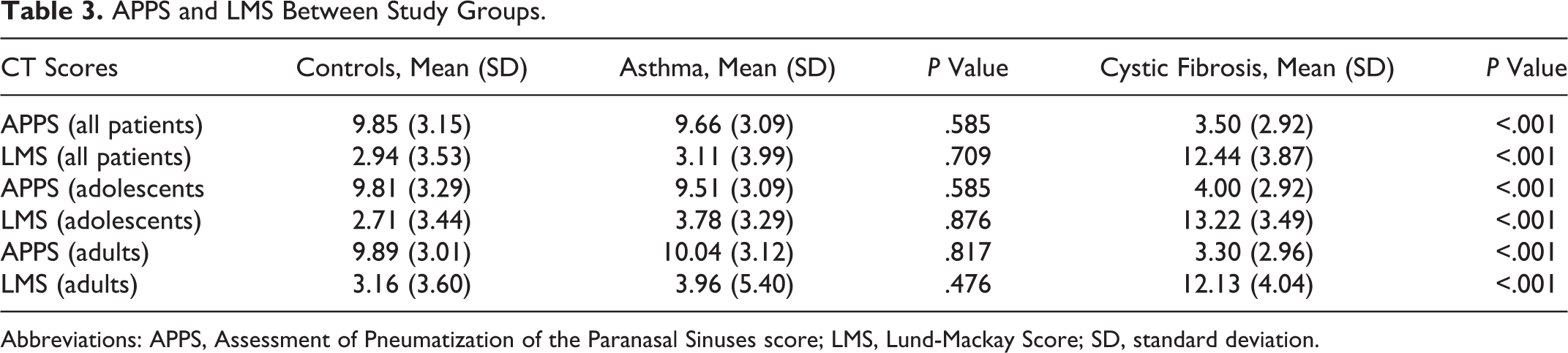
Abbreviations: APPS, Assessment of Pneumatization of the Paranasal Sinuses score; LMS, Lund-Mackay Score; SD, standard deviation.
Discussion
Paranasal sinus pneumatization differs widely between patients, and certain pneumatization variants have been linked to specific clinical entities. 1 –9 Nevertheless, the mechanism for sinus pneumatization is incompletely understood, and the role of sinonasal and respiratory disease in this process is unclear. The unified airway theory has suggested that pathophysiological mechanisms in sinonasal or respiratory disease may have effects at distant airway sites. 15 –23 Cystic fibrosis results in concomitant lung and sinonasal pathology and has also been demonstrated to result in lower airway remodeling 29,30 and sinus hypoplasia. 4 –6 Asthma has been implicated as a driving force in lower airway remodeling, but its effect on upper airway anatomy and sinus pneumatization has not been studied. 22,31,32
In CF, for which sinus hypoplasia has been thoroughly described, the underlying etiology remains poorly understood. Sinus hypoplasia also appears to be present in primary ciliary dyskinesia and Kartagener syndrome, 8 which share phenotypic ciliary motility dysfunction with CF. Nevertheless, there have been studies which suggest that the sinus hypoplasia seen in CF is independent of clinical manifestations of the disease. In a porcine CF model, sinus hypoplasia was found to precede clinical sinonasal disease. 4 Similar findings have been reported in a rat model as well. 13 Sinus hypoplasia was significantly more pronounced in patients with delta F508 homozygosity compared to other mutations. 5 Temporal bone pneumatization, on the other hand, was not impaired by homozygous delta F508 mutations, even though these aerated spaces are lined by respiratory mucosa. 6 Separately, sickle cell anemia is associated with sphenoid aplasia, and regional blood flow anomalies or elevated serum erythropoietin have been described as potential etiologies. 9,12 Ultimately, it remains undetermined to what extent paranasal sinus pneumatization is influenced by disease phenotype, underlying genetic mechanisms, or comorbid processes.
The present study seeks to determine whether there are analogous effects on paranasal sinus pneumatization in asthma, which have previously gone undetected due to difficulty in quantifying total sinus volume. The current data do not support global differences in paranasal sinus pneumatization between patients with asthma and controls. Therefore, decreased sinus pneumatization cannot be considered as a universal feature of respiratory mucosal inflammatory disease. However, this does not exclude respiratory mucosal disease as an inciting event for sinus hypoplasia. Disease onset at particular points in sinonasal development may result in the anatomical changes associated with CF. Additionally, CF and primary ciliary dyskinesia may represent more sustained or a higher degree of inflammatory disease necessary to arrest sinus pneumatization. Nevertheless, it does not seem that this effect can be extrapolated to all types of respiratory or sinonasal mucosal inflammatory disease.
There are several limitations identified in the current study. Because the effect of asthma on sinus pneumatization has not been investigated in past studies, sample size calculations were inevitably imprecise. Initial estimated sample size of 788 patients was calculated using Cohen d method based on an assumption of small effect size (d = 0.2). In reality, the current results indicate a much smaller effect size (d = 0.06) and would require a sample size of approximately 7000 patients to achieve adequate power. Therefore, even if a statistical difference in sinus pneumatization between patients with asthma and control exists, it may not be of clinical relevance. Second, the diagnosis of asthma was ascertained retrospectively from the records of different practitioners across a large health system. This may lead to inconsistency in the assignment of the diagnosis, as was evident in incomplete data on asthma severity. A third limitation was that the patients with asthma in this study did not have a statistically higher Lund-Mackay score than the control population. As previously noted, CRS is more common in patients with asthma, and radiologic CRS severity has been shown to be correlated with asthma severity. 21 This suggests that the diagnosis of asthma may not have been assigned consistently or that the patients in this study had predominantly intermittent or mild persistent asthma. On the other hand, radiologic sinus opacification is not diagnostic for CRS alone. 33 Future study would benefit from a cross-sectional or prospective design with consistent diagnosis of asthma and disease severity by a small group of physicians.
Asthma is not associated with altered paranasal sinus pneumatization, even though it has been implicated in lower airway remodeling. Cystic fibrosis, by comparison, is associated with marked sinus hypoplasia. Decreased paranasal sinus pneumatization does not appear to be a universal feature of respiratory or sinonasal mucosal inflammatory disease.
Footnotes
Authors’ Note
Poster presentation at the Combined Otolaryngology Spring Meeting; May, 2016; Chicago, IL.
Acknowledgments
The authors thank Martha Gastanaduy, BA, MPH, for biostatistical consultation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.