
Abstract
Augmentation rhinoplasty is one of the most common plastic surgery procedures performed in Asia. Most Asian patients desire not only a natural-looking nose but also a nose with natural feel. Achieving such rhinoplasty outcomes with grafts has been a challenge for surgeons due to rigidity of grafting material. We propose a novel technique to address this limitation. A total of 200 healthy adult patients aged from 18 to 25 years were randomly chosen and classified into 5 groups: A, B, C, D, and control. Each group included 40 patients. The patients assigned to conventional grafting underwent rhinoplasty with L-shaped silicone prosthesis (group A) or expanded polytetrafluoroethylene (e-PTFE; group B), using traditional carving methods. The patients assigned to dynamic rhinoplasty underwent silicone (group C) or e-PTFE grafts (group D) using the modified double “V” method, which involves removing bilateral wedges from the graft to decrease rigidity. Patients in control group do not undergo the surgery. A 3-dimensional raster surface scanner was used to capture the images of the patients accurately and nasal mobility was measured. Subjective evaluations were carried out by a series of questionnaires asked to the patients. The angle α of nasal mobility was significantly lower in conventional grafting (23.09 [5.34] mm for silicone and 17.88 [4.96] mm for e-PTFE) versus the “V” carving (30.53 [3.76] mm for silicone and 23.77 [4.53] mm for e-PTFE; P < .05). The double “V” carving method is a simple, effective, and practical method for improving dynamic nasal outcomes in patient undergoing augmentation rhinoplasty.
Introduction
Cosmetic surgery is one of the fastest growing types of elective surgeries in Asia, and augmentation rhinoplasty is gaining in popularity. Reports indicate that the number of rhinoplasty patients has multiplied in the recent years. 1,2 Most rhinoplasty patients desire a natural-looking nose with good symmetry, appropriate length, and rotation. In order to achieve such great results in rhinoplasty, more advancements should be made in this field. An optimal aesthetic outcome consists of both anatomical static beauty and functional dynamic beauty.
Our previous study has shown that augmentation rhinoplasty with alloplastic grafting impairs postoperative nasal mobility, and the degree of rigidity depends on type of different prosthesis used. 3 As a whole, the L-shaped silicone implants seemed to bring better nasal mobility compared with expanded polytetrafluoroethylene (e-PTFE) after rhinoplasty. However, the implant lacked stability because when the nasal tip was moved, the entire nose followed, especially near the nasion. This leads to an unnatural nasal appearance. The present study aims to improve the dynamic beauty of rhinoplasty by applying a new carving method of the prosthesis double “V” method.
Patients and Methods
In this study, we chose 200 healthy adult patients who were all Chinese Han females without any previous nasal surgeries. Their age ranged from 18 to 25 years. All the patients were blinded for the study but understood whether the carving method of the prosthesis was modified and whether silicone or e-PTFE was implanted. All patients were divided randomly into 5 groups: A, B, C, D, and control. Groups A and B underwent rhinoplasty through vestibular incision with the traditional carving method of L-shaped silicon (WanHe; WanHe Plastic Materials Co, Ltd, Guangzhou, China) and e-PTFE (Tisuthes; SuoKang Medical Materials Co, Ltd, Shanghai, China) graft, respectively. On the other hand, double “V” method was used to carve L-shaped silicon and e-PTFE in groups C and D, as a new method. Patients in control group do not undergo the surgery. Only the person who performed the surgeries knows about the study; other investigators including those doing the measurements were all blinded. Power calculation has been performed after we collected all the data to verify sample collection and reliability of data. All the patients were followed for 6 months postoperatively during which they had no complaints about the static nasal morphology.
Carving Process of Nasal Prosthesis
The prostheses used in this study were L-shaped silicone and e-PTFE grafts. A vertical marking was placed in the midline of the nose. A horizontal marking was made between 2 eyebrows and between inner canthus at the nasion, corresponding to the superior border of the prosthesis. The junction of the mobile part and the fixed part on the patient’s nasal dorsum was designated as point “m.” The nasal tip was taken as point “o.” The medical ruler was used to measure the distance between “o” and “m,” and this distance was designated as “E.” A bilateral wedge incision was made at the distance “E” from the nasal tip of the silicone or PTFE prosthesis with the angle β of 25° to 45° and the width of the incision was one-third of the prosthesis. The final bilateral incision was V-shaped (Figure 1). According to the specific characteristics of each patient’s nose, the length, thickness, width, and radian of the prosthesis were adjusted. After finishing the carving of the prosthesis, it was immersed in chloramphenicol solution.
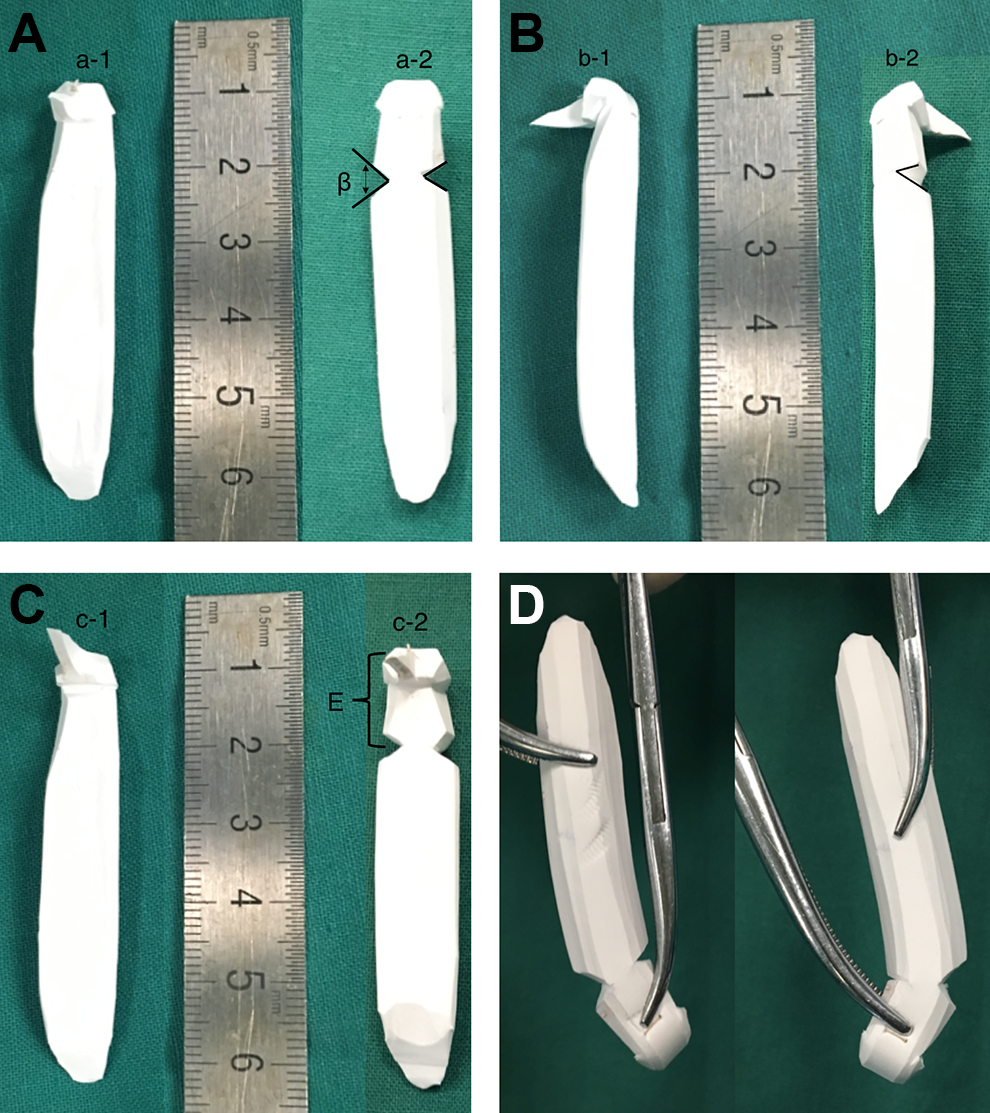
Comparison of the prosthesis between traditional carved and the new modified version; β is angle of the “V” shaped incision, and E represents the distance between the fixed part on the patient’s nasal dorsum and nasal tip. Different angles of view: (A) front of the prosthesis, (a-1) front of the traditional carved implant, (a-2) front of the new modified version, (B) lateral of the prosthesis, (b-1) lateral of the traditional carved, (b-2) lateral of the new modified version, (C) back of the prosthesis, (c-1) back of the traditional carved, (c-2) back of the new modified version, and (D) mobility of the new prosthesis.
Surgical Procedures
The positions of the nasal tip, the nasion, and the median line were marked before the operation. Then, the patients were injected local anesthesia with 2% lidocaine and 100 000 epinephrine. The medial marginal incision at the right nasal alar was performed for all patients. The nasal alar and upper lateral cartilages, the upper perichondrium, and the lower aponeurosis were widely stripped to the upper part of the pyriform aperture. The fascia between nasal bone and lateral nasal cartilage was excised. Then, the lacunar space was isolated along the nasal lateral midline of the periosteum to accommodate the portion of the prosthesis using a detachment device.
Under the guidance of nasal introducer, the prosthesis was implanted into the lacunae with the vascular forceps. Then the positions of the prosthesis and nasal tip were evaluated, ensuring that there was no blanching of the skin at the nasal tip. Lastly, the incision was sutured with 5-0 nylon. Oral antibiotics were prescribed for 3 days after the operation.
Method of Data Collection
The study was conducted prospectively. All patients were scanned using Axis 3-D scanner (Axis Three XS-400; Axis Three, Belfast, United Kingdom), and assessments were carried out in the raster scan image. In order to reduce the variable pressure based on a swab, the maximum dynamic degree of the nasal tip was pushed by the same blinded researcher with the same force. Outcomes were evaluated by both objective and subjective measures of cosmetic and functional (mobility) outcome. The following data were collected and analyzed: mobility of the nose, the length of the mobile part, the nasal length, and report of subjective outcome for all the patients at final evaluation. Images were obtained according to standardized techniques of clinical photography. Before taking the images, hair covering the face and eyeglasses were removed. The patient sat up and was instructed to keep her eyes level with the horizontal line. For a standard clinical image, a constant brightness and exposure were used. The distance between the patient and the scanner was 80 to 120 cm. The scanning area was from hairline to the thyroid cartilage. The patients were instructed to hold a swab and put the tip to the position between the nasal tip and the edge of the right (or left) alar groove. The swab was pressed to contralateral sides to check maximum skewing (Figures 2 and 3). Measurements were carried out on the images using the software Axis Three versions 2.7.2 and were used to simulate the plastic surgery procedures by Rose Bellingham. Along the dorsal midline, “n” stands for the nasion, “m” for the turning point of the nose, “o” for the nasal tip, and the angle α indicated the mobility of the nose. The length of the d (mo, the mobile length of the nose) as well as the whole nasal length L was calculated. The proportion of d in L was calculated, as well. These measurements were carried out twice, and the average values were recorded (Figure 4).
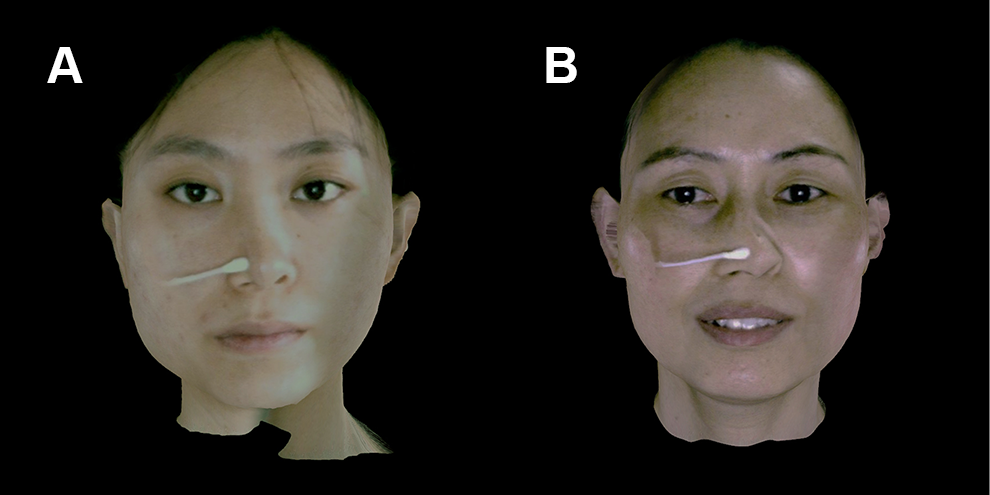
Comparative status of the nasal shape and mobility in postoperative patients with traditional carved prosthesis (A) and the double “V” method of L-shaped-carved prosthesis (B).
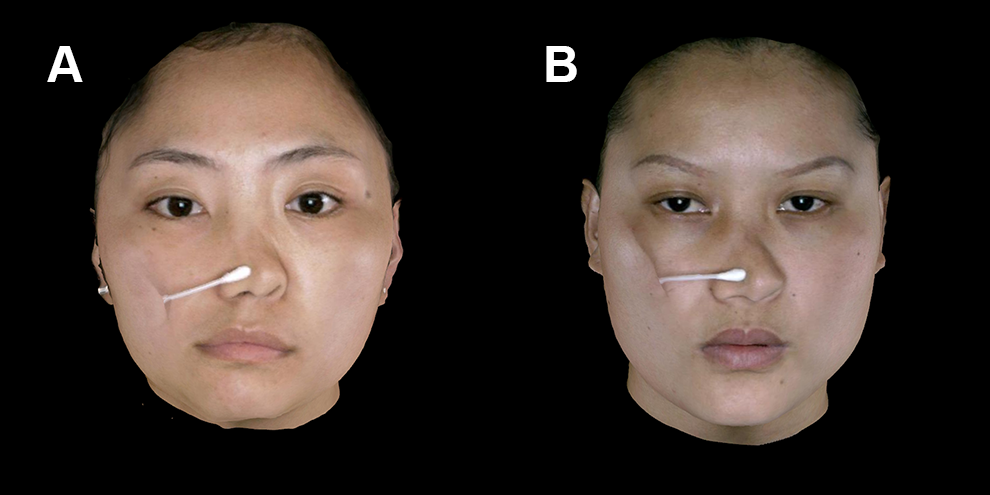
Comparative status of the nasal shape and mobility in postoperative patients with traditional (A) and the double “V” method of expanded polytetrafluoroethylene (e-PTFE) implants (B).
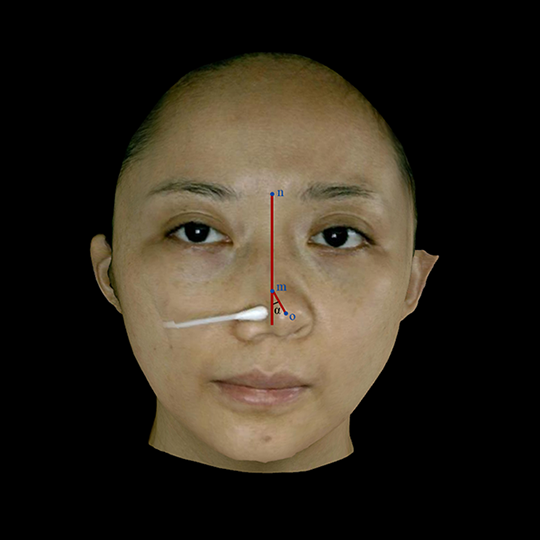
Nasal measurements used in this study. Along the dorsal midline, “n” stands for the nasion point, “m” stands for the turning point of the nose, “o” stands for the nasal tip, and the angle α indicated the mobility of the nose. d is the mobile length of the nose and L is the nasal length.
Subjective measures were carried out by a series of questionnaires administered to all patients. The questionnaires queried whether they noticed any changes postoperatively to mobility and appearance of the nose. The patients were also asked whether the operation influenced their social life.
Statistical Analysis
Data were presented as average values with standard deviations. Data were analyzed using 1-way analysis of variance test. P value of less than .05 was considered statistically significant (SPSS, version 16.0; SPSS, Inc, New York, United States).
Results
The outcomes are demonstrated in Table 1. The mobile nasal length in group C (23.76 [2.78] mm) and group D (12.10 [2.21] mm) was shorter than that of group A (27.09 [3.21] mm) and group B (13.96 [1.8] mm). The mobile angle in group C and D was increased compared to group A and B. In contrast to group D, the nasal mobility of group C was similar to normal patients who did not undergo rhinoplasty. Some patients did not show any significant changes in the mobile length and angle of the nose. All the patients showed decreased nasal mobility compared to the control group, and there were significant differences between group A and control, group B and control, group C and control, and group D and control (P < .05; Table 2). The range of nasal mobility in control group was 34.23 ± 3.14 degrees, and the length of mobile part was 17.22 ± 0.81 mm, the length of whole nose was 45.59 ± 7.34 mm. As shown in Table 3, P values are statistically significant (P < .05) between groups C and D, groups A and C, and groups B and D. The images taken from groups A, B, C, and D are shown in Figures 2 and 3. Our questionnaire results revealed that only 13.5% patients in group C and 17% in group D noticed the decline of nasal mobility, whereas more patients noticed nasal mobility in group A (28%) and group B (30%). This suggested better nasal mobility in groups C and D. In group C (n = 40), about 21.5% complained that their postoperative social life was influenced as they were afraid of touching their nose in public, whereas the result for group D (n = 40) was only 17%; 15% of group C were unsatisfied with postoperative rigid and unnatural-looking nose, whereas that of group D was just 8%; 5% of group A were scared to rub and clean the nose’s skin daily, whereas that of group D was 4.5%. The results showed that patients in group D were most satisfied with postoperative appearance, suggesting that this double “V” method of rhinoplasty had a positive outcome.
Group Wise the Relative Assessment and Association of Nasal Measurements in Postoperative Patients.a
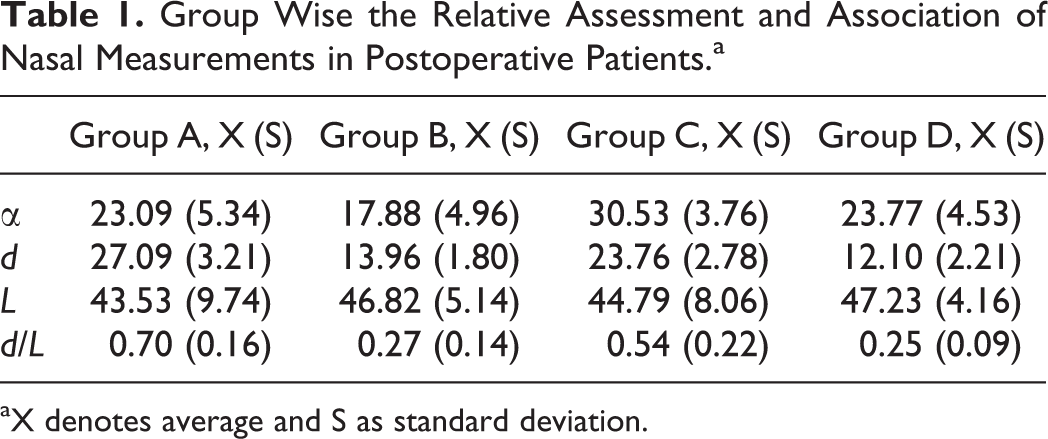
aX denotes average and S as standard deviation.
Comparative View of P Values Between Groups and Control With the Nasal Measurements Parameters.
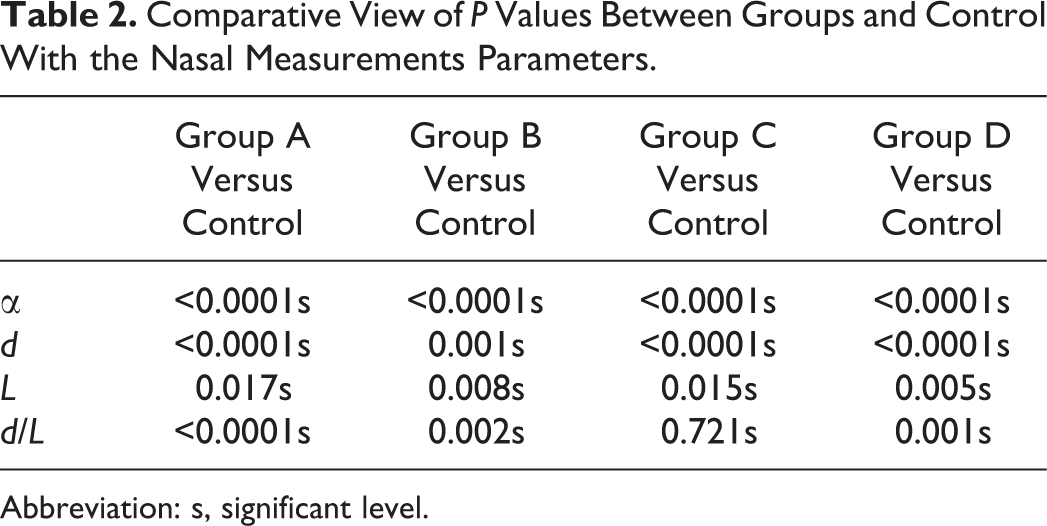
Abbreviation: s, significant level.
Comparative View of P Values Among Groups A, B, C, and D With the Nasal Measurements Parameters.

Abbreviation: s, significant level.
Discussion
Rhinoplasty is the most common facial surgery performed in Asia. Different continents have their own unique nasal structures. The Asian nose has characteristic anatomy that requires appropriate rhinoplasty technique to achieve optimal aesthetic outcomes. 4 Most Asian noses are characterized by thick skin with an abundant subcutaneous fat tissue, wide dorsum, and bulbous nasal tip. 5 In order to achieve a natural-looking nose, features such as certain lines, shadows, specific proportions, and breakpoints should be evaluated. The size and proportion of the nose is often compared with the face. In recent years, dynamic beauty has received increasing attention in rhinoplasty. 6 Nasal beauty is not only limited to repairing defects but also ideally brings expression in harmony with other units on the face. A strategic point in rhinoplasty is complex interaction between the soft tissue and the nasal bone frame. Understanding this interaction is mandatory for proper design and execution of the aesthetic surgical plans. 7
Two components can be augmented in rhinoplasty: the rigid dorsal component and the mobile nasal component. Nasal bones, frontal process of the maxilla, and the nasal process of the frontal bone support part of the rigid dorsal component. The other parts such as lateral nasal and alar cartilages represent flexible and mobile nasal components. Many studies reported that nasal tip dynamics are related to facial aesthetics. 6 The movement of the nasal tip is associated with the dimensions of the columella, septum, alar cartilages, nasal spine, or with the shape of the lip. 8 Nonetheless, these dynamic factors are largely unknown to many surgeons specializing in rhinoplasty, leading to unsatisfactory results and relapses.
Many researchers have reported that surgical alteration of the nasal tip remains one of the most difficult and challenging aspects of rhinoplasy. 9 Therefore, many surgical techniques are used for improving tip refinement and projection, such as a septal extension grafts, medial crural sutures, and medial crura to septum sutures. However, the majority of these surgical procedures only focus on changing the shape, rotation, projection, and integrity of the nasal tip, such as decreasing the length of the upper 2 legs (alar cartilages) to increase tip rotation. 10 None of these procedures emphasize dynamic beauty of nasal tip after rhinoplasty.
Our previous study showed that the most widely used L-shaped implants reduced the nasal mobility in the Asian population, 3 which were also verified by data in Tables 1 and 2. The e-PTFE implants decreased the nasal mobility, whereas the silicone implants tended to result in a rigid nose. Hence, our simple and effective modified carving technique in augmentation rhinoplasty can improve postoperative nasal mobility. As “V” incisions are given in the prosthesis bilaterally, it can be rotated within a certain angle, leading to increased mobility of the nose. The results from our questionnaires also indicated that our modified rhinoplasty improved the patient satisfaction. Merely 21.5% patients in group C and 17% in group D mentioned that the cosmetic nose influenced their social life in contrast to 35% in group A and 28% in group B. The number of patients who were not pleased with the change of nasal mobility has reduced to 13.5% and 17% in groups C and D, respectively. However, 2 patients from group A and 1 patient from group C complained about the rigid and unnatural appearance of the nose.
In general, cartilage grafts are preferred in rhinoplasty. Autogenous grafts carry the least risk of complications and can be harvested in great quantity. However, there are many limitations that should be addressed, including unpredictable bending of nose, prolonged operation, significant donor site infection, and scarring. For all these complications, our method can be an attractive alternative for congenital nasal deformations, trauma, or revision rhinoplasty. Many plastic surgeons have described a technique of placing only a dorsal silicone implant and using an auricular cartilage graft as a cap graft to elevate the nasal tip. 11,12 But, this method prolongs the surgery time, adds additional bulk to the structure of the nose, and may create extra thickness, especially in patients with a thick nasal tip.
Porous high-density polyethylene (Medpor, Porex Surgical Inc, Newnan, United States) is also an implant used in rhinoplasty since the 1980s. 13 Although it has great biocompatibility, it also has many complications, such as extrusion, fistula, and high rigidity. In recent years, microautologous fat transplantation has become increasingly popular, 14 but it is associated with improper projection of the nasal tip and nasal dorsum. Therefore, silicon and e-PTFE implants are still the optimal implants. This clinical experience is why we used these 2 implants in our study to achieve a better dynamic beauty after rhinoplasty. As shown in Table 1, the nasal mobility in groups C and D were 30.33 (3.76) and 23.77 (4.53) mm, respectively, whereas that of groups A and B were 23.76 (2.78) and 12.10 (2.21) mm, respectively. These data suggested higher nasal mobility in groups C and D and the mobile length of the nose was shorter in these 2 groups. These significant findings provided strong evidence that the double “V” way of carving prosthesis could increase nasal mobility and prevent the nose from moving with the whole prosthesis.
We have enlisted a blinded researcher to perform all the measurements, although there are still possibilities that the force may be applied differently by the same person. More accurate and precise methods are required to eliminate the errors and address these limitations. In our study, group C patients’ nasal rotation reached to 34° to 35°, which near to a natural nose. However, the nasal mobility in group D didn’t increase significantly compared to group C, which is only 23.77 (4.53) mm. The length (d) in group C was longer than that of group D as shown in Table 2, which may result from different prosthesis. It is reported that calcification and capsule formation are 2 major late complications of silicone. 13 The possible reasons are: (1) silicon being a foreign implant, it cannot adhere tightly to the bone surface; and (2) intraoperative large empty space formation may result in movement of the implant. In case of e-PTFE implant, capillaries, collagen, and connective tissues including fibroblasts grow into the pores as e-PTFE pore size is 10 to 30 μm, resulting in strong adherence with surrounding tissue. 13 Therefore, the probability of nasal displacement is relatively lower in e-PTFE implant.
The study also has some limitations. Our double “V” methods enhanced the rhinoplasty outcomes, but the study was only carried out to 6 months. It is possible that at later time points, over the course of years, the modification may result in untoward consequences, such as fracture of silicone or e-PTTFE tip. Such damage to the implant may lead to replacement and extrusion of the prosthesis, and the appearance of nose may be influenced if the tip loses its mechanical support. We plan to report outcomes at 1 year or longer in future research. Further studies are required to improve and eliminate the limitations of the double “V” method.
Conclusion
This study designed a simple and an effective double “V” carving method of L-shaped silicon and e-PTFE. This method enhanced dynamic rhinoplasty outcomes by increasing nasal mobility and improved patient satisfaction compared to traditional methods of rhinoplasty. As cosmetic surgeons, we understand that patient demands a symmetrical, natural nose. Further improvements are required in cosmetic surgery, and we believe that our study has contributed to the field of dynamic beauty in rhinoplasty.
Footnotes
Authors’ Note
Shan-shan Bai and Dong Li contributed equally to this work and share first authorship. All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No. 81471886).