
Abstract
Silicone implants are commonly used alloplastic materials for rhinoplasty in Asia, as they are easy to manipulate, provide adequate volume augmentation, and exhibit excellent biocompatibility. However, they are associated with complications such as infection, displacement, and extrusion. Recently, we encountered an interesting complication in a 53-year-old woman presenting with palpable and visible stepping of the nasal dorsum. The patient had previously undergone rhinoplasty with an L-shaped silicone implant, and symptoms had been noticeable for approximately 1 year. Lateral nasal computed tomography revealed a fractured silicone implant. Because the patient reported no history of nasal trauma since rhinoplasty, we assumed that the silicone implant might have fractured spontaneously. The findings in this case suggest that spontaneous implant fracture can be a late complication of rhinoplasty with silicone implant.
Introduction
Planning dorsum-augmentation rhinoplasty for Asian patients is challenging. 1 Among various augmentation materials, silicone implants are the material of choice for many surgeons, because they are easily manufactured, provide sufficient volume, and are free from resorption and deformation. 1 However, silicone implants used for rhinoplasty are associated with several complications, including infection, contracture, calcification, and dislocation. 2 Compared to early-onset complications, extremely long-term complications occurring >20 years after surgery have rarely been reported. Recently, we encountered a patient who had undergone rhinoplasty with an L-shaped silicone implant 25 years prior to visiting our clinic. She presented with visible transverse lines on the dorsal skin and step-like discontinuity of the nasal dorsum, which was recognized 1 year prior to presentation. We suspected that this occurred owing to extremely delayed fracture of the previously inserted L-shaped silicone implant. Here, we report the findings and lessons learned from this case.
Case Report
A 53-year-old woman complained of palpable and visible nasal dorsal stepping, recognized 1 year prior to visiting our clinic. The patient had undergone rhinoplasty 25 years prior to visiting our institute, and reported that the previous rhinoplasty consisted of dorsal augmentation using a silastic implant material and nasal-tip augmentation using autologous conchal cartilage. Apart from rhinoplasty, the patient had no other medical history, including trauma.
Physical examination revealed a transverse line on the skin at the mid-portion of the nasal dorsum. The lesion was perceived as a step on palpation, and the nasal dorsum was divided by the transverse stepping lesion (Figure 1A). In the basal view, columellar deviation to the right and consequent nostril asymmetry were noted. Lateral radiography revealed fracturing of the previously inserted implant material (Figure 1B). Because the cause of the fracture could not be identified, we hypothesized that the previously inserted silicone material had spontaneously fractured in the mid-dorsal region. We planned a revision rhinoplasty, including removal of the previously inserted implant, redesigning of the silastic implant, and appropriate nasal-tip plasty. After making bilateral alar marginal and inverted-V-shaped transcolumellar incisions, the previously inserted implant material was identified inside the surrounding capsule. The L-shaped silastic implant was fractured at the mid-portion of the nasal dorsum (Figure 2A), and upon removal, the material was found to be partly calcified with a whitish discoloration (Figure 2B). We designed a new I-shaped silastic implant and performed nasal-tip augmentation with a 3-layer onlay graft using the septal and conchal cartilages. The patient’s surgical outcome was satisfactory.
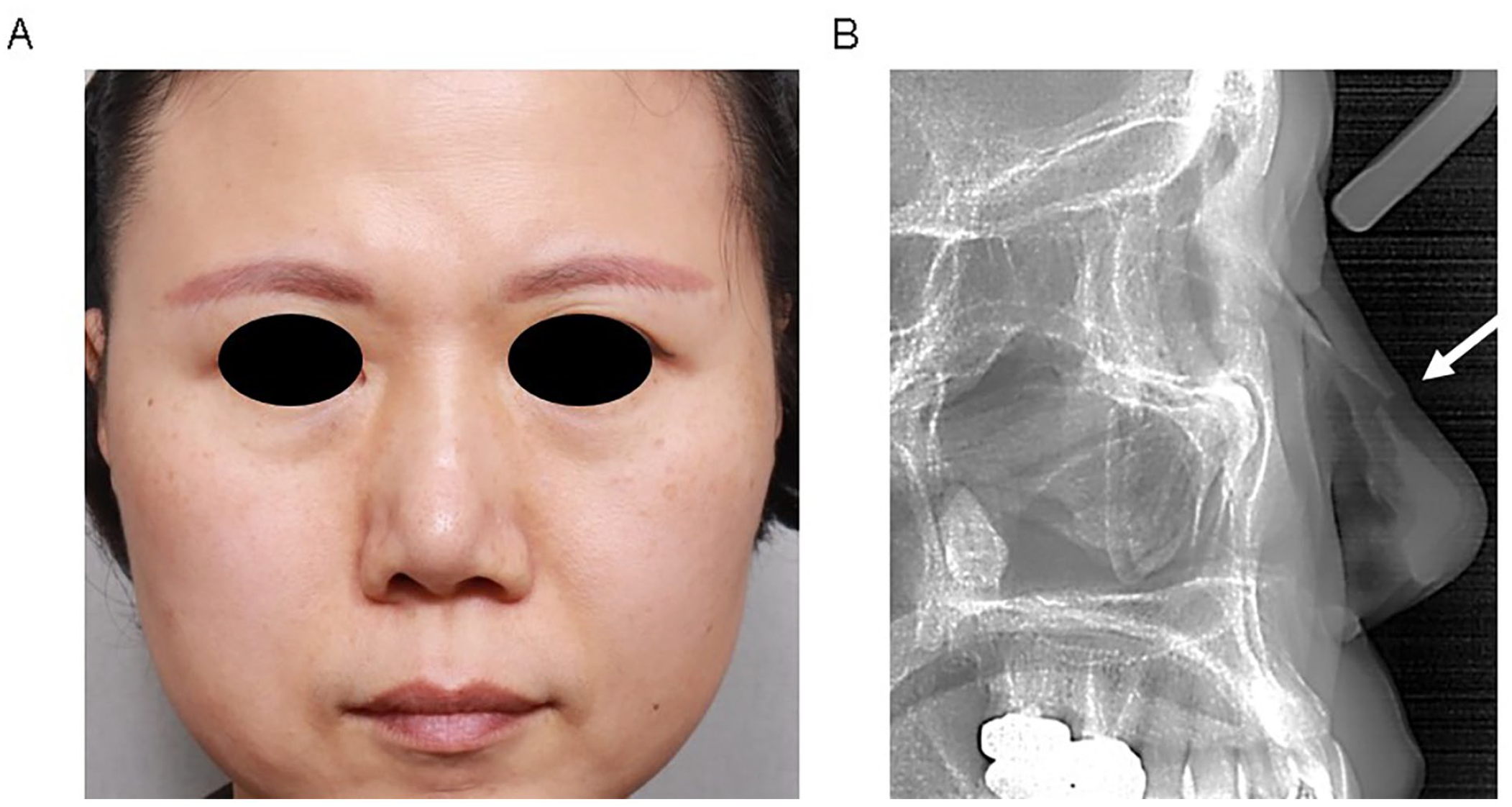
(A) Preoperative frontal photograph. (B) Lateral radiography demonstrating fracture line.
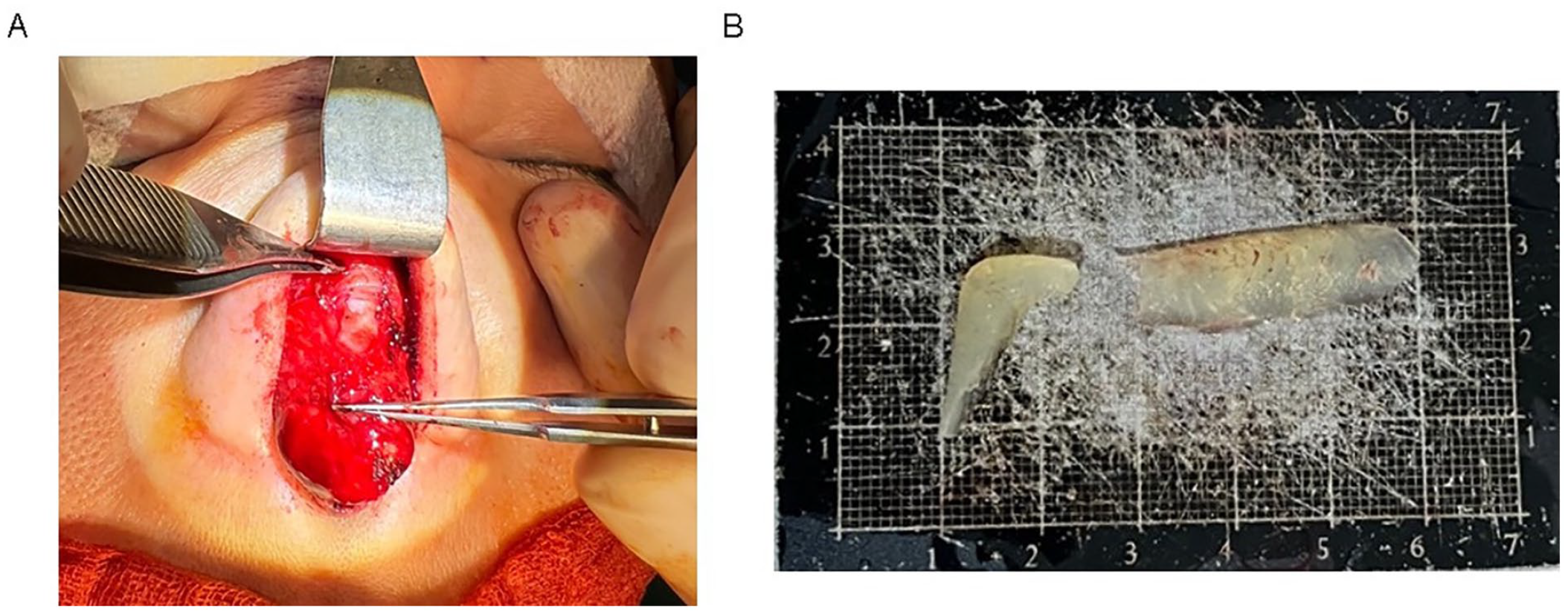
(A) Intraoperative photograph of the nasal dorsum shows transverse fracture of the previously inserted implant on the mid-portion of nasal dorsum. (B) Photograph of the removed fractured L-shaped silicone implant.
Written informed consent was obtained from the patient.
Discussion
Various surgical techniques and graft materials have been developed for rhinoplasty. In the Asian population, augmentation rhinoplasty is the most frequently performed procedure, and silicone implant materials have long been applied. The use of silicone implants reduces operation time, because of their ease of handling and ability to provide sufficient volume augmentation. Silicone is free from resorption and deformation and does not harbor bacteria internally owing to its non-porous nature. Moreover, it can be easily sterilized using an antiseptic solution.1,3 Silicone implants can be classified into L-shaped and I-shaped implants. L-shaped silicone implants have been widely used in Asian countries because they provide smooth and undisrupted nasal dorsal contours from the radix to the nasal tip, and reduce the difficulties associated with tip plasty. 1 Although these implants may be an attractive choice, particularly for cosmetic reasons, they are associated with increased risks of tip problems, such as extrusion, over rotation, and abnormal narrowing. In our patient, an L-shaped silicone implant was inserted during a previous surgery. Although the implant did not induce complications such as infection, dislocation, or extraction, it spontaneously fractured long term after insertion. As it was firmly attached to the surrounding tissues, the normal soft-tissue structures were slightly destroyed during dissection and removal. For revision rhinoplasty, due to the weakened remnant nasal structure, we chose an I-shaped silicone implant to reduce potential complications associated with L-shaped silicone implants.
Complications associated with silicone implants include high rates of cutaneous erythema, extrusion, infection, and displacement.4,5 However, long-term complications, such as those occurring >20 years after insertion, have rarely been reported. Extrusion of silicone implants into the nasal septum and associated inflammation has been reported 25 years after rhinoplasty. 4 A study reviewed the medical records of 221 patients who underwent revision rhinoplasty after rhinoplasty with silicone implants and reported that most complications occurred within the first few years after surgery, with capsular contracture and calcification being the most delayed complication. 6 We add another delayed complication: implant fracture, which occurred at least 20 years after surgery. Regarding the cause of fracture, the patient did not report a definite history of nasal trauma after the previous surgery. Therefore, we hypothesized that the fracture might have occurred spontaneously due to minor mechanical force during daily life, and not due to severe iatrogenic mechanical force. According to a previous study, calcifications were observed with the naked eye at 5 years and 8 months after insertion, and the number and size of calcifications observed on gross examination increased with time. 6 In our case, gross examination revealed calcifications on the removed silicone implant (Figure 2B); however, no signs of gross infection or inflammation of the surrounding capsular tissues were observed. Therefore, we suspect that progressive calcification over the implantation period might have decreased the original softness of the silicone and hardened the implant, inducing spontaneous implant fracture during daily life.
Silicone implants are effective and relatively safe for augmentation rhinoplasty. Although complication rates are reported to be low, most reported complications are relatively early-onset complications that occur several years after surgery. The findings in our case showed that long-term complications such as spontaneous implant fracture can occur, suggesting that attention should be paid to delayed complications after silicone implant rhinoplasty.
Footnotes
Acknowledgements
None.
Data Availability Statements
The datasets generated during and/or analyzed during the current study are not publicly available owing to the patient’s privacy, but are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean Government (MSIT) (2022R1F1A1063720).
Ethical/Consent Statement
Written informed consent was obtained from the patient.