
Abstract
Keywords
Introduction
Rhinoplasty is one of the most commonly performed facial plastic surgeries, with more than 200,000 operations conducted in 2018 in the United States alone. 1 Esthetic nose irregularities are the main complaints of patients who consider rhinoplasty. 2 A joint structural deformity of the nose is a dorsal hump. 2 Classical approach to a dorsal hump is the structural excision of excess bony and cartilaginous tissues developed by Joseph 3 (Figure 1). Classic structural rhinoplasty (CSR), while being quite effective at reducing dorsal humps, may lead to loss of structural integrity and an esthetically un-pleasing appearance due to small irregularities on the dorsum.3,4
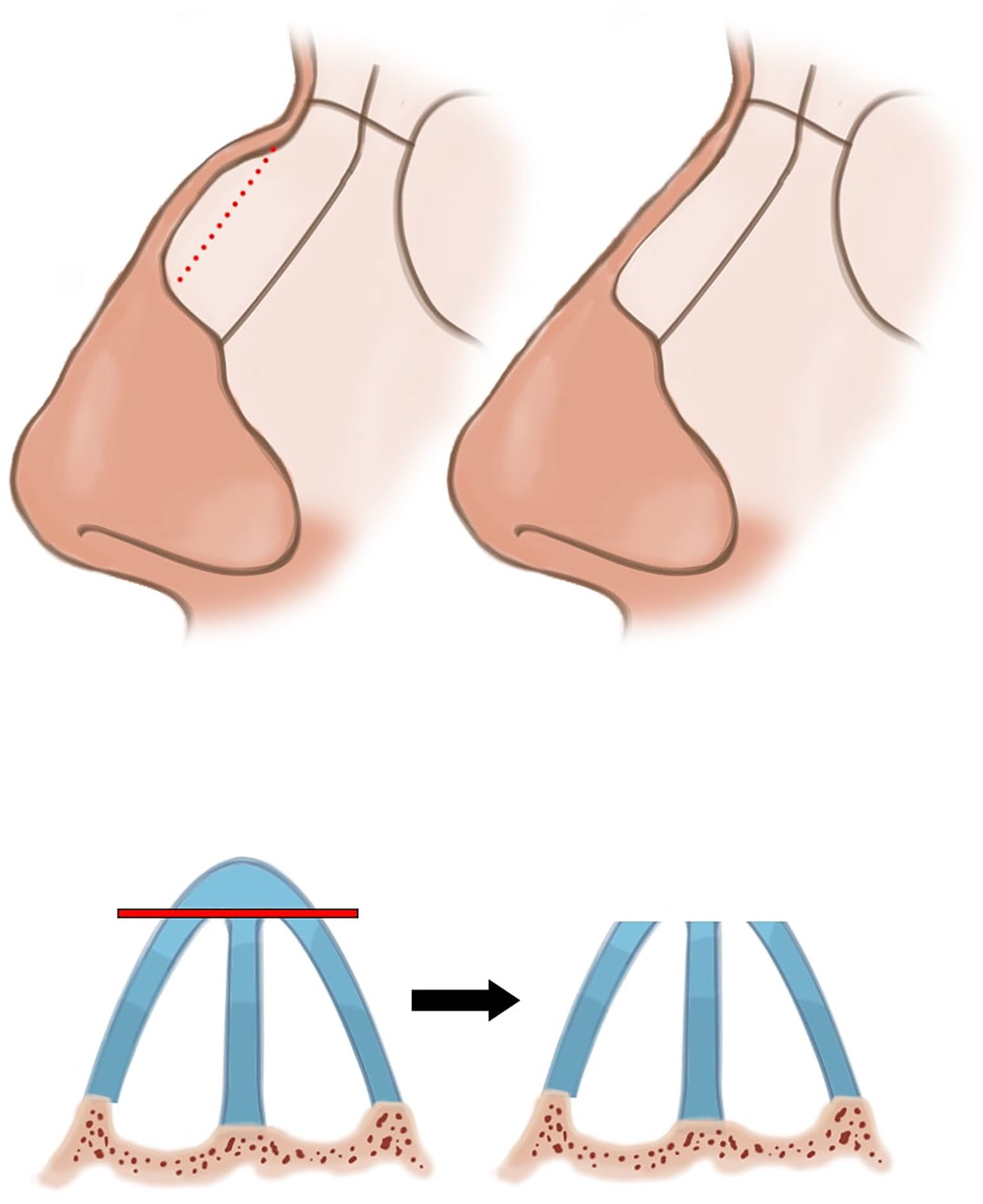
Classical Structural Rhinoplasty.
To overcome the risk of complications and obtain an esthetically pleasing dorsum, a “dorsal preservation” rhinoplasty (DPR) technique has been established and improved over the years and gained popularity among rhinoplasty surgeons. Unlike CSR, in which the excess bony and cartilaginous structures are excised, preserving the nasal bones but relocating them to cover the newly formed dorsum is the main concept in DPR. DPR can be further subdivided into 2 approaches, one being “push-down” (PD) and the other “let-down” (LD). A high septal resection in conjunction with lateral osteotomies allows the direct lowering of the bony vault toward the pyriform aperture in PD. In contrast, a high septal resection and an accompanying resection of a wedge of bone at the ascending frontal process of the maxilla allows the bony vault to descend freely in LD.5-11 (Figures 2 and 3). These techniques allow the preservation of dorsal esthetic lines and the structural integrity at the nasal keystone area.10,11
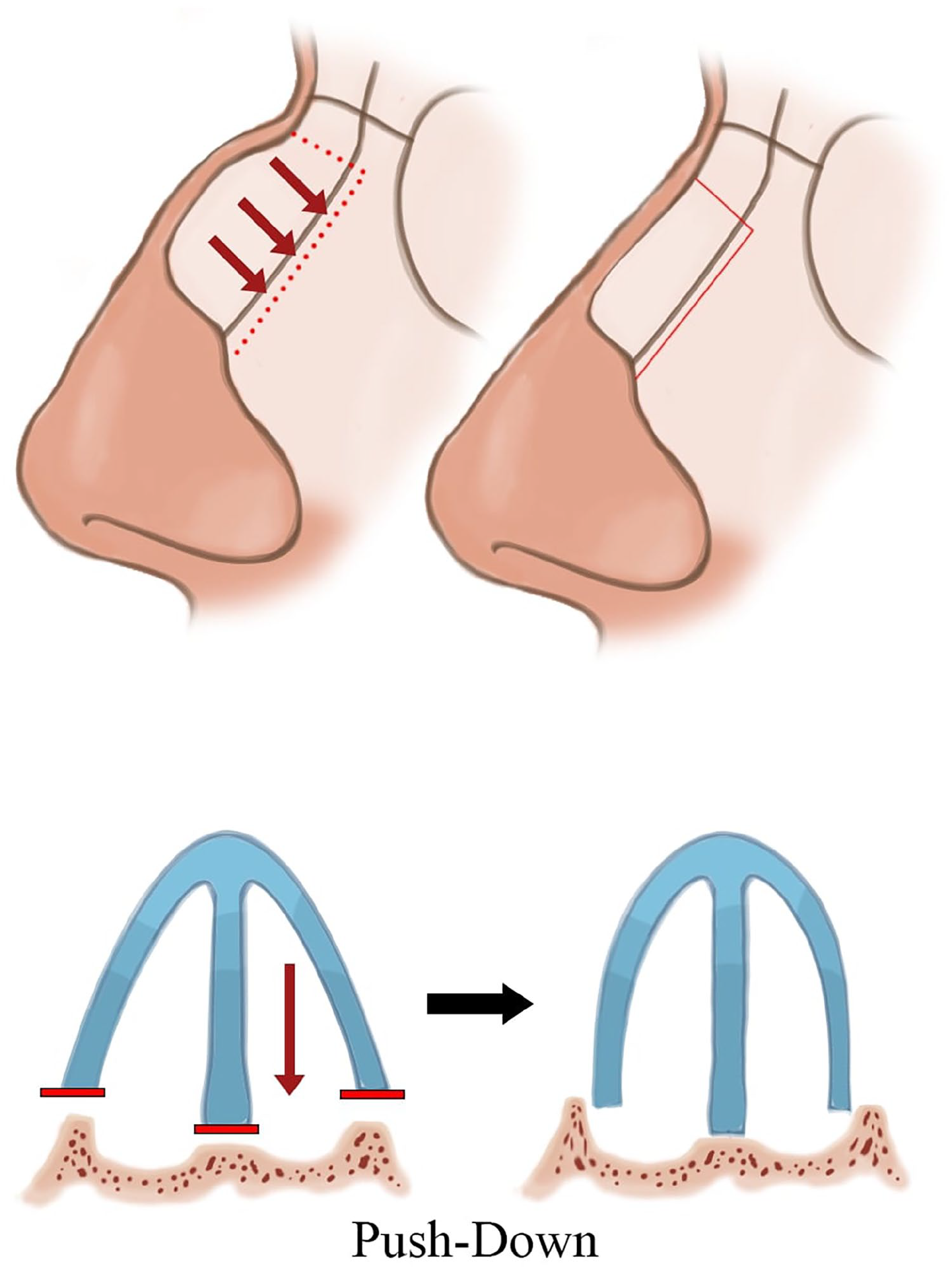
Push-Down Technique.
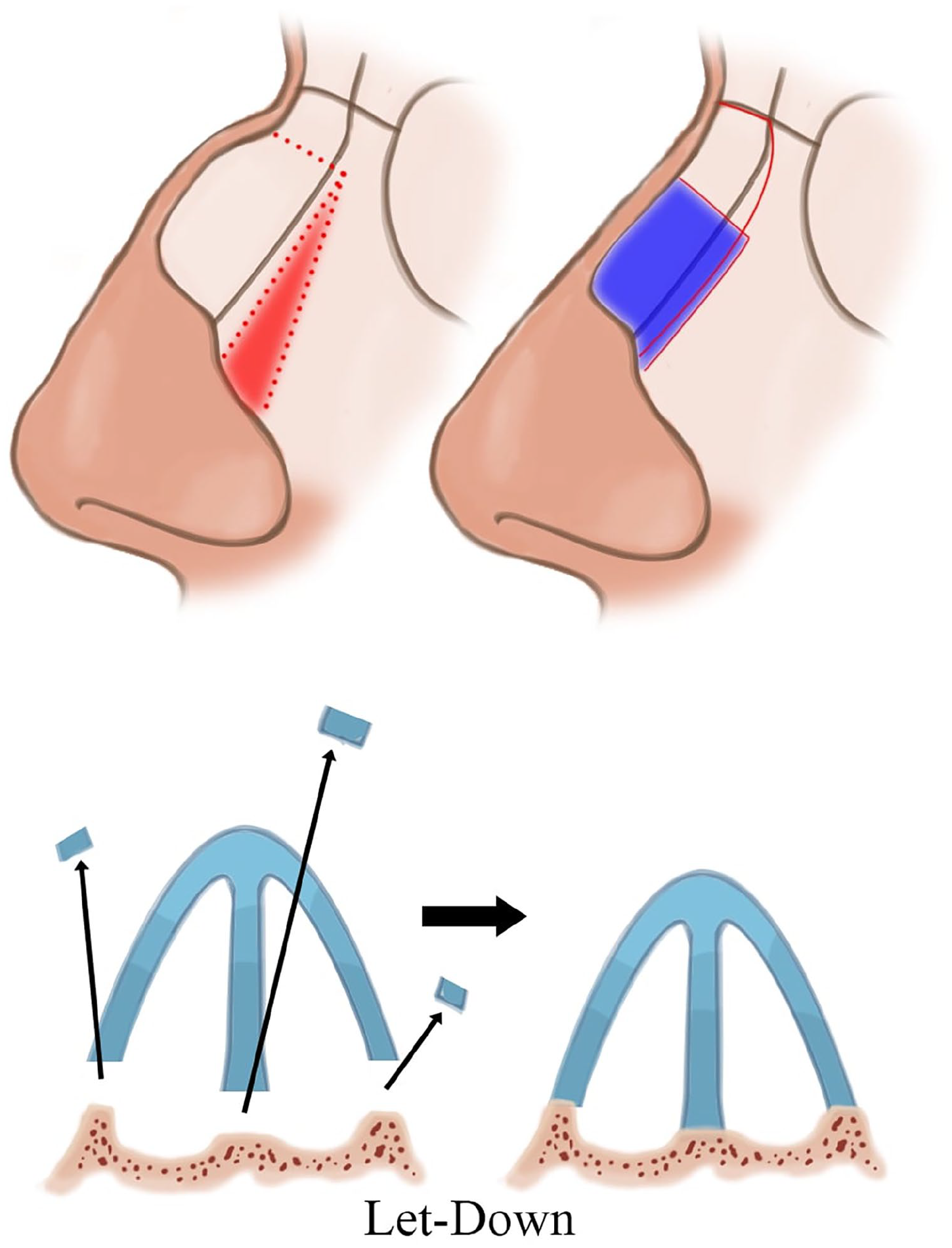
Let-Down tecnique.
Preservation of unobstructed nasal airways is of utmost importance in rhinoplasty surgeries as diminished airflow can cause significant discomfort to the patients and may require further intervention. 12 Objective quantification of nasal airway parameters can be achieved by using acoustic rhinometry (AR), by which minimum cross-sectional areas (MCA) and internal nasal volume (VOL) can be obtained. 13 Patient Reported Outcome Measurements (PROM) are also commonly employed to assess subjective functional outcomes.
This article examines whether classic structural rhinoplasty and dorsal preservation rhinoplasty techniques impacted nasal airway dimensions by comparing preoperative and postoperative measures of MCA and VOL for each technique.
Materials and Methods
Patients
There were 124 patients in this study, of which 80 were female (64.5%) and 44 were male (35.5%). All patients applied to our otolaryngology clinic with complaints regarding the physical appearance of their noses without any problems in nasal breathing and underwent a primary rhinoplasty surgery performed between January 2018 and June 2019 following the authors’ shared surgical regime. Nasal Obstruction Symptom Evaluation (NOSE) scores were obtained before and after the surgery. The inclusion criteria were a NOSE score below 5. Exclusion criteria were septal deviation and concha hypertrophy, as this study aims only to compare the effects of DPR and CSR approaches. None of the patients underwent a complementary or turbinoplasty with their rhinoplasties except for the minimal septal excisions required for DPR and CSR techniques.
Patients were consecutively randomized, and dorsal preservation rhinoplasty was performed on 64 patients (51.6%), while classical structural rhinoplasty was performed on the remaining 60 (48.4%). The mean age of the patients at the time of the operation was 25 ± 7.75 (min: 18, max: 48). The follow-up time was 6 months, at the end of which AR was performed.
Surgical Technique
While both DPR and CSR were employed with an open approach, we abstained from radiofrequency or out-fracture applications as to not influence rhinometry measurements.
A columellar incision was made in DPR operations, and the nasal dorsum was observed after the skin elevation. After septal dissection, required cartilage and ethmoid bone resections were made alongside lateral and transverse osteotomies to allow the descent of the bony vault. There were no septal interventions other than the necessary septal excisions. The repositioned nasal dorsum was then reconnected to the septum with sutures, and the operation was concluded with a tip-plasty.
CSR operations followed a similar start with a columellar incision, skin elevation, and the visualization of the nasal dorsum. Excess bony and cartilaginous tissues of the dorsal hump were excised, and any irregularities were filed. There were no further septal interventions. The medial and lateral osteotomies were followed by spreader grafts. Operations were concluded with a tip-plasty.
Acoustic Rhinometry
Rhinomanometry is a physiologic outcome measure that measures nasal airway resistance and is the gold standard for objective functional assessments of the nasal airway. 14 Unlike rhinomanometry, AR is an anatomic outcome measure of the nasal airway that uses acoustic reflections to calculate the minimum cross-sectional area and volume of the nasal airway. 15 While it is true that breathing is a dynamic process and AR assumes the nasal tissues to be static, we have used rhinometry data in this study to examine structural changes in the nasal airways after 2 different rhinoplasty techniques.
Nasal Airway Parameters
There are 4 parameters relating to nasal airway dimensions in this study, which Clement et al previously established, and the specifications Türk et al had used in their research has also been used in this study (Figure 4).16,17
MCA1: MCA from the nostril to 2.20 cm into the nasal cavity
MCA2: MCA from 2.20 cm to 5.40 cm into the nasal cavity
VOL1: Internal nasal volume from the nostril to 2.20 cm into the nasal cavity
VOL2: Internal nasal volume from 2.20 cm to 5.40 cm into the nasal cavity
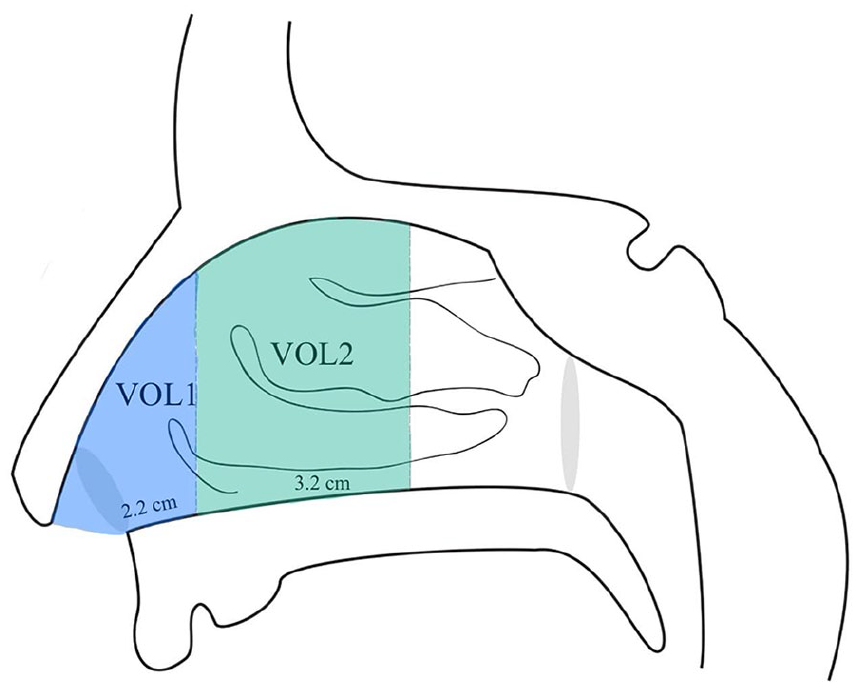
VOL1: Internal nasal volume from the nostril to 2.20 cm into the nasal cavity , VOL2: Internal nasal volume from 2.20 cm to 5.40 cm into the nasal cavity.
All measurements were taken with an AR device (Rhinoscan SRE2000, RhinoMetrics A/S, Lynge, Denmark, with Rhin98 2.0 software for evaluation) by the same author, NS, before and 6 months after the surgery.
Statistical Analysis
All statistical analyses were conducted on SPSS (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0; IBM Corp., Armonk, NY, USA). The Kolmogorov–Smirnov test was performed. According to this test, when variables did not meet the normal distribution, the Wilcoxon test was used to compare dependent groups. When the variables were normally distributed, a paired t-test was used to compare means. When variables were not normally distributed, the Mann–Whitney U test was used. Bonferroni corrections were made to account for multiple analyses.
Ethics Committee Approval
This research was approved by SBU Sisli Hamidiye Etfal EAH Ethics Committee with approval number 2468. Written consent was obtained from all patients presented in this article with an enlightened consent form.
Results
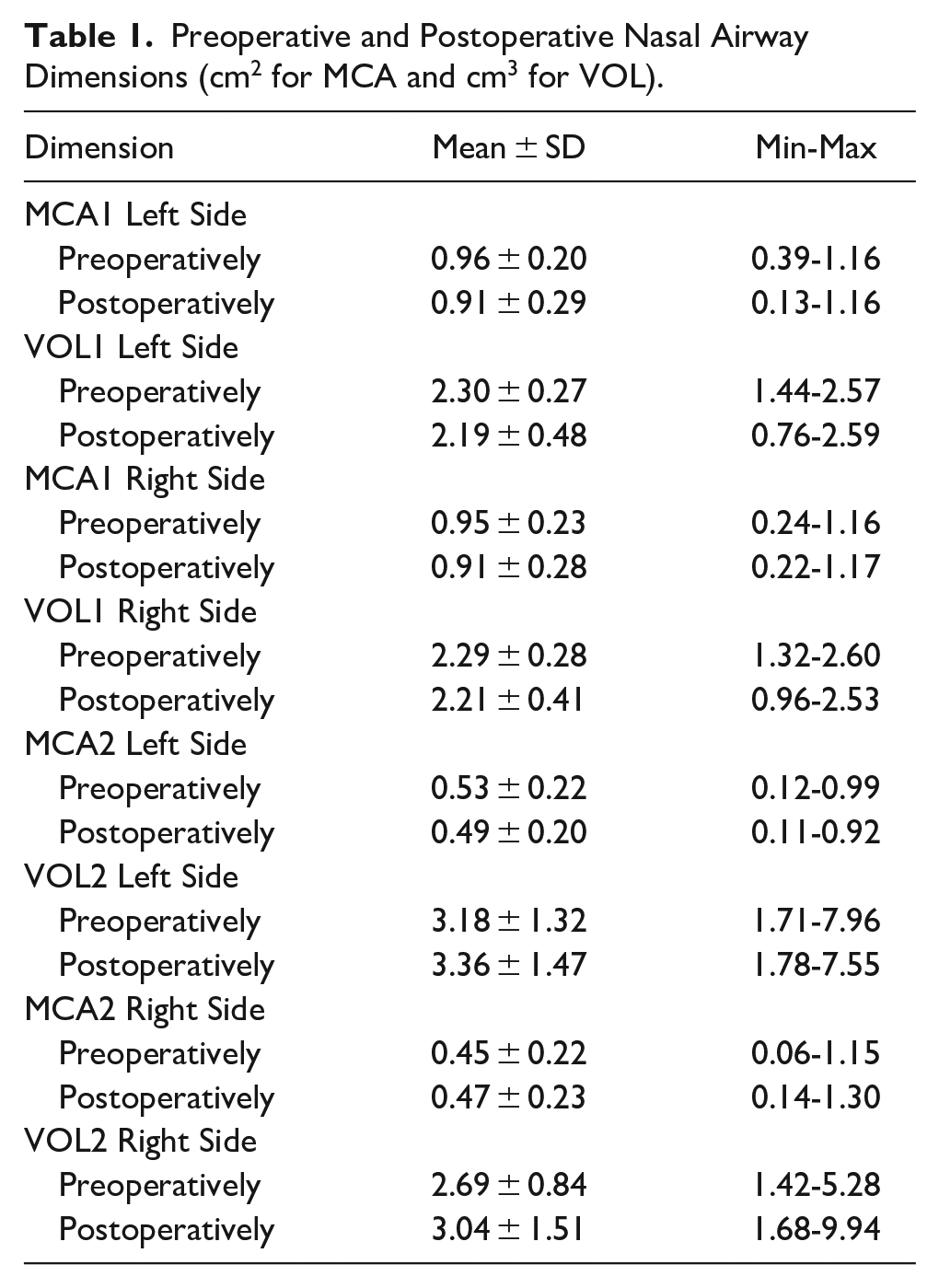
Preoperative and postoperative mean values of MCA1, VOL1, MCA2, and VOL2 for both sides of nasal cavities independent of the technique employed are presented in Table 1.
Preoperative and Postoperative Nasal Airway Dimensions (cm2 for MCA and cm3 for VOL).
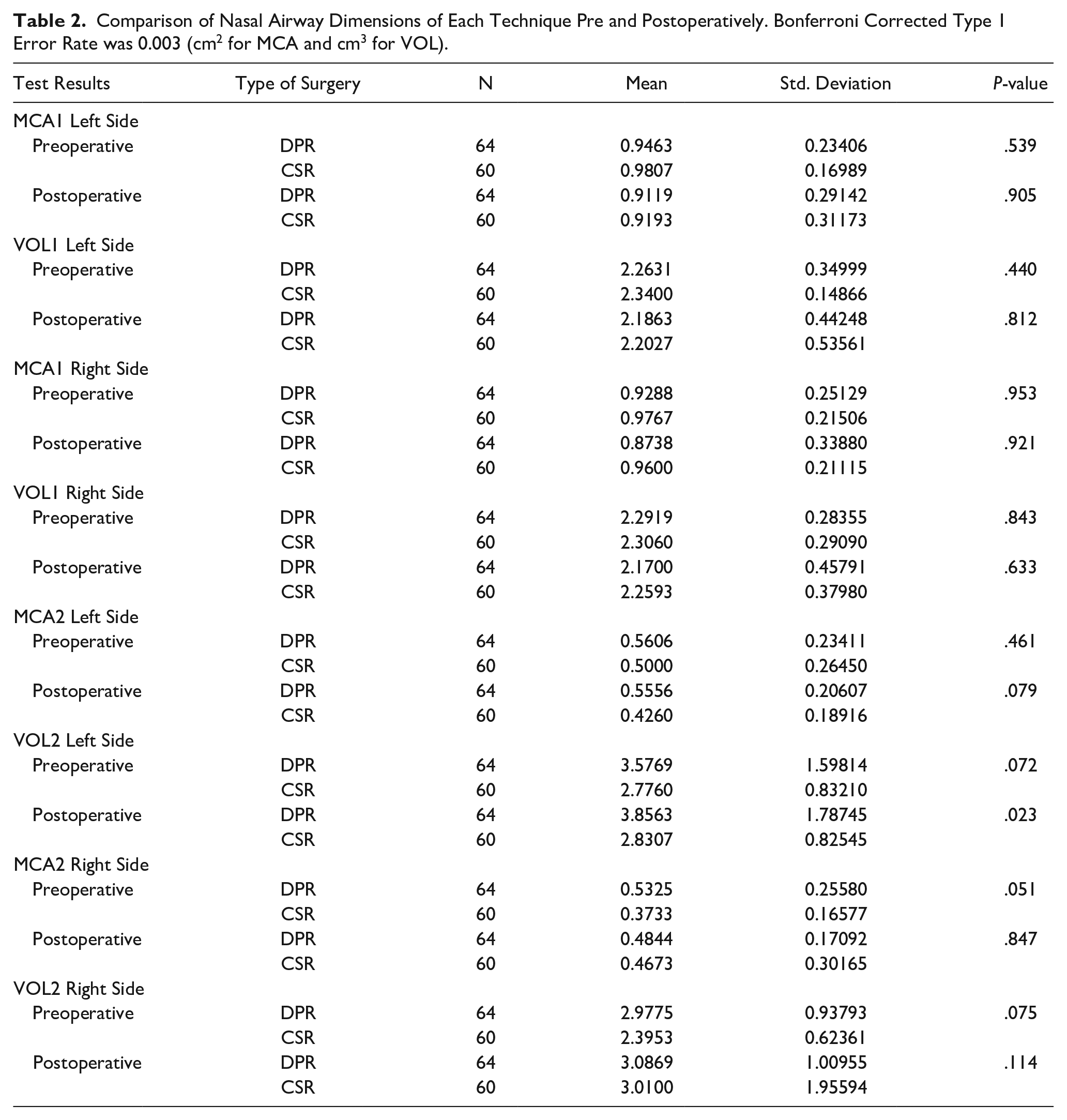
Patients in both DPR and CSR groups had similar nasal airway dimensions before and after having surgery. (MCA1 left side DPR vs CSR P = .539, VOL1 right side DPR vs CSR P = .843) (Table 2).
Comparison of Nasal Airway Dimensions of Each Technique Pre and Postoperatively. Bonferroni Corrected Type 1 Error Rate was 0.003 (cm2 for MCA and cm3 for VOL).
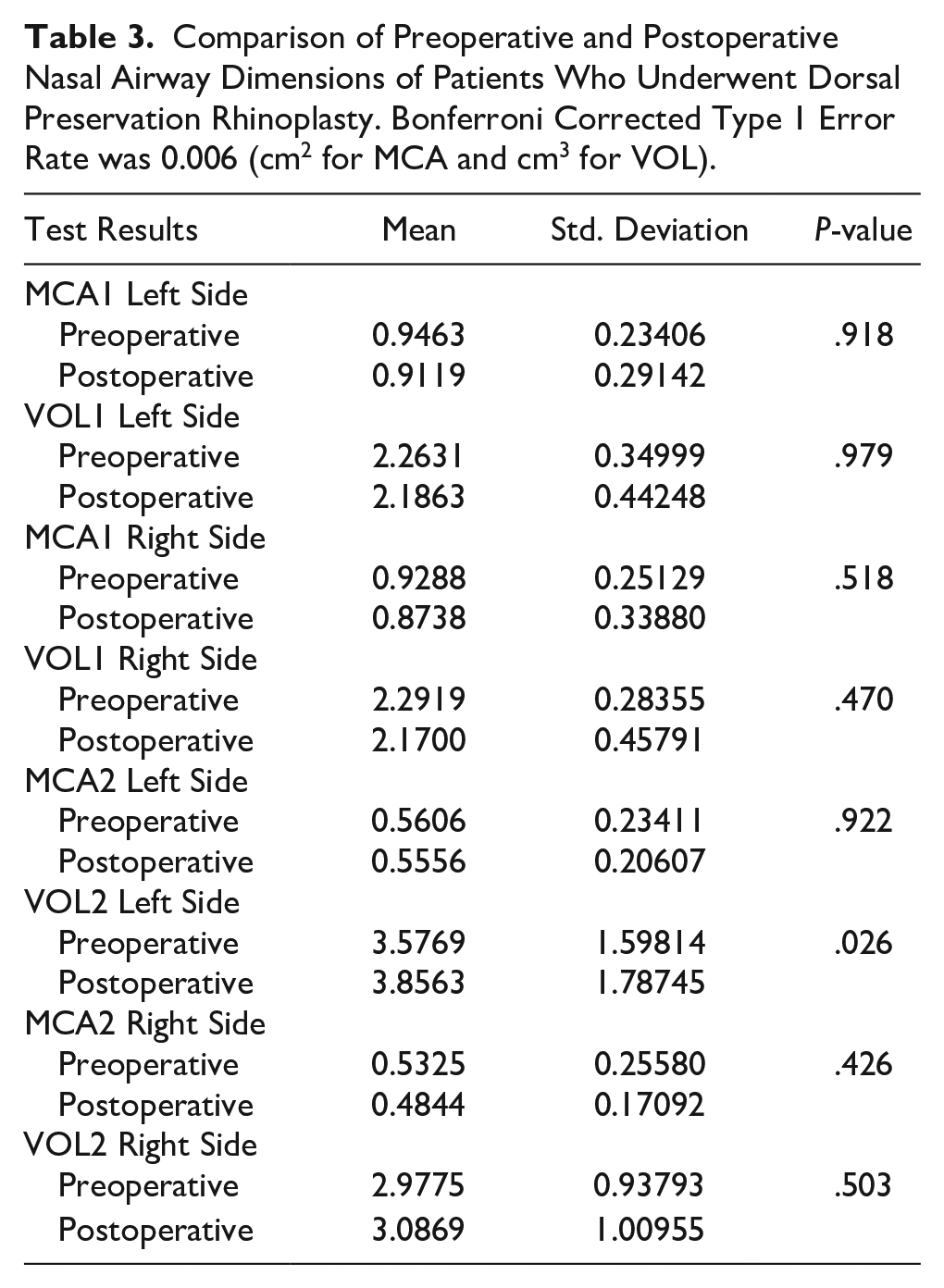
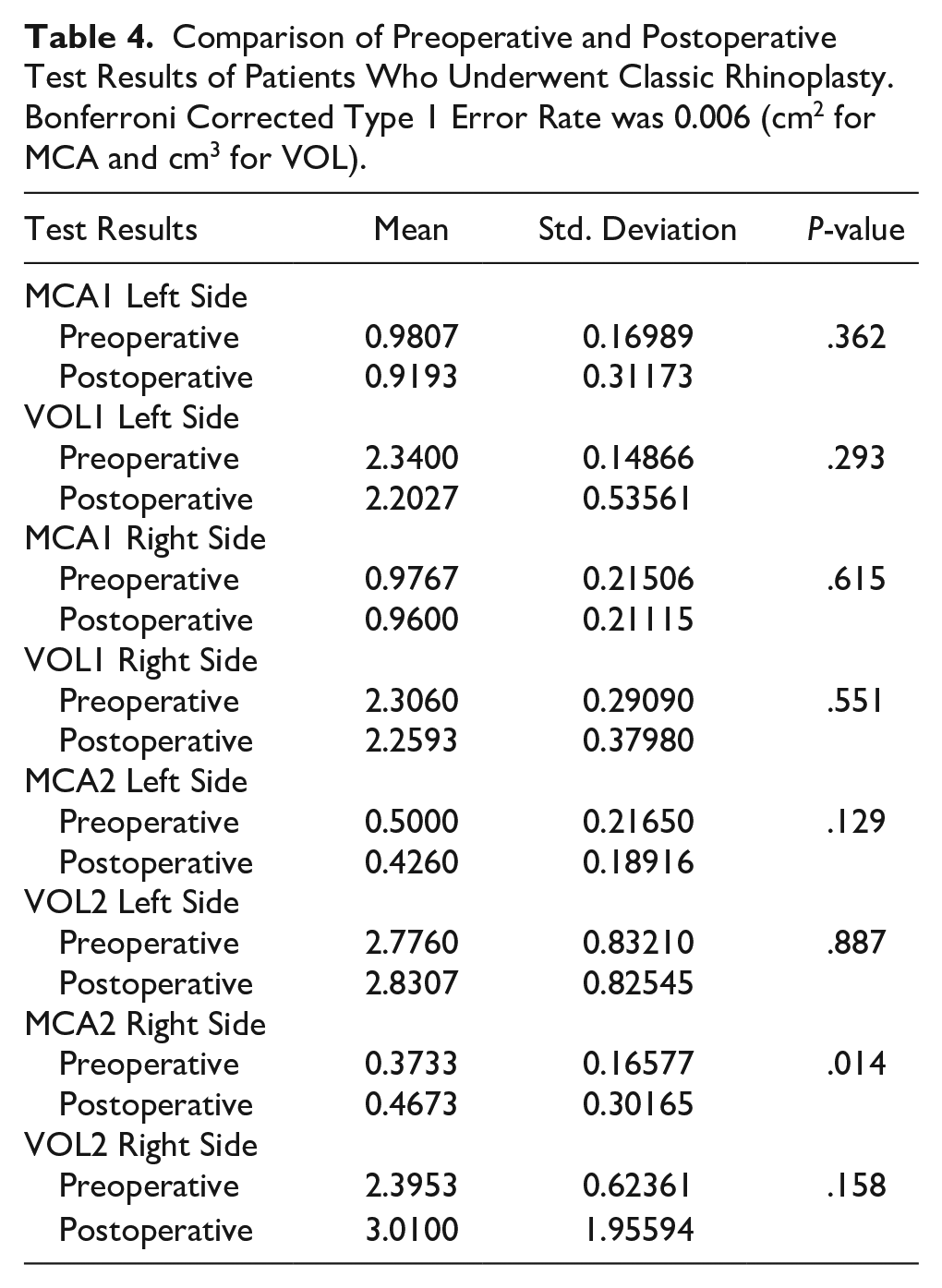
There was no statistically significant difference between preoperative and postoperative MCA and VOL levels in either DPR or CSR technique (MCA1 preoperative measurement compared to postoperative measurement with DPR technique P = .918, MCA1 preoperative measurement compared to postoperative measurement with CSR technique P = .362) (Tables 3 and 4).
Comparison of Preoperative and Postoperative Nasal Airway Dimensions of Patients Who Underwent Dorsal Preservation Rhinoplasty. Bonferroni Corrected Type 1 Error Rate was 0.006 (cm2 for MCA and cm3 for VOL).
Comparison of Preoperative and Postoperative Test Results of Patients Who Underwent Classic Rhinoplasty. Bonferroni Corrected Type 1 Error Rate was 0.006 (cm2 for MCA and cm3 for VOL).
Discussion
Several methods have been previously employed to assess functional outcomes of nasal airways. 15 Even though both rhinomanometric and rhinometric measures give an idea about nasal airflow, the latter is more critical for the scope of this article as we’re more interested in the structural changes, about which rhinometry provides a better understanding. PROMs, such as the NOSE questionnaire, have been widely used to assess functional outcomes and complications of rhinoplasty patients in conjunction with objective measurements. Reinforcing rhinometric outcomes with PROMs is critical as they provide an idea about the patient’s perceptions of functional outcomes and enable a correlation to be made between objective and subjective measurements. In this study, functional complaints of patients were evaluated with the NOSE questionnaire before and after the surgery at the 6-month follow-up. All patients had a NOSE score of less than 5 on both occasions, indicating no functional negative perceptions. The absence of negative subjective outcomes bolsters rhinometric findings, suggesting the lack of a significant difference in MCA and VOL values, suggesting that dimensions of the nasal airway are neither predictive nor indicative of the technique.
Effects of DPR and CSR on the nasal airway dimensions without septoplasty and turbinate interventions mainly stem from the osteotomies performed. Grymer et al had postulated that in reduction rhinoplasty, there was a 22% to 25% reduction in cross-sectional area at the level of nasal valve and 11% to 13% at the level of pyriform aperture. Since then, the effects of osteotomies on subjective and objective outcomes have been contradictory and are still a matter of debate.18-23
Abdelwahab et al had previously compared radiological outcomes of DPR and CSR techniques in cadavers and found significant changes in cross-sectional areas of internal nasal valves of cadavers that had undergone PD DPR but not on those that underwent LD DPR. 24 This study diverges from the article by Abdelwahab et al in 2 ways: first, our measurements were taken from living people, and second, we used AR instead of computed tomography.
Several reports have measured nasal airway dimensions with AR after rhinoplasty: Paul et al have shown that spreader graft rhinoplasty significantly increased the cross-sectional area of the nose together with a subjective functional improvement. 25 Kahraman et al have used VOL and MCA values for 4 groups of patients: septoplasty, septoplasty with spreader graft, septorhinoplasty, and septorhinoplasty with spreader graft. 26 Deviated side significantly increased MCA values in all groups, while there was no substantial change in VOL values. Nondeviated sides had no significant change in any measures and groups. 26 Erdogan et al also found substantial changes in MCA values on the deviated side but no significant changes in the nondeviated sides in septorhinoplasty cases. 27 Kilic et al compared structural and functional outcomes before and after decongestion in 2 different groups of patients, one of which had undergone inferior turbinate reduction in addition to septorhinoplasty. 28
The literature suggests a change in nasal airway dimensions is rooted in the septal and turbinate interventions in a rhinoplasty setting. This correlates with our findings, as none of our patients underwent septoplasty and we have not found significant differences in nasal airway dimensions apart from the aforementioned exceptions of the left side.25-28 This study is the first to date to assess the effects of DPR and CSR techniques individually and comparatively on nasal airway dimensions in actual patients, building upon the knowledge with cadavers. 24
Overall, our results suggest that the technique employed in a rhinoplasty setting, whether DPR or CSR, is not significantly related to any changes in nasal airway dimensions. As a result, it could be postulated that neither DPR nor CSR significantly affects nasal geometry or ease of breathing. More patients from different ethnicities and surgeons trained in different parts of the world are required to confirm that the nasal airway dimensions are not predictive or indicative of the technique.
Conclusion
In summary, nasal airway dimensions do not predict or indicate whether the DPR or CSR technique will be/has been used in a rhinoplasty surgery, and the employed technique does not significantly alter the nasal geometry or ease of breathing. Surgeons choosing between DPR and CSR in a rhinoplasty setting should remember that changes in nasal airway dimensions are more likely to have occurred due to the intervention to septa or turbinates.
Footnotes
Acknowledgements
The authors have no acknowledgment regarding the contents of this manuscript.
Consent to Participate
Written consent was obtained from all patients presented in this paper with an enlightened consent form.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This research was approved by SBU Sisli Hamidiye Etfal EAH Ethics Committee with approval number 2468.