
Abstract
Background:
Evidence-based practice in intrapartum care is critical for lowering maternal and neonatal mortality and morbidity. Evidence-based practice, according to the World Health Organization Quality of Care Framework for Maternal and Newborn Health, is an important component of intrapartum care. However, little is understood about evidence-based intrapartum care practice in Ethiopia, particularly in the study setting.
Objective:
To assess evidence-based intrapartum care practice and associated factors among obstetric care professionals in Jimma Zone public hospitals in Southwest Ethiopia.
Methods:
A facility-based cross-sectional study was carried out on 217 obstetric care providers in Jimma Zone public hospitals in southwest Ethiopia. The study used a census approach to include all eligible participants within the specified population. Data were collected from June 1 to 30, 2023, using semistructured self-administered questionnaires. The collected data were entered into EpiData version 4.6 and exported to Statistical Packages for Social Sciences version 25 for analysis. Multivariable logistic regression was run to see the association between evidence-based intrapartum care practice and predictor variables. Statistical significance was set at p-values less than 0.05 in the multivariable logistic regression.
Results:
Overall, 41.2% (95% CI: 40.8–42.3) of obstetric care providers in Jimma Zone public hospitals used evidence-based practices for intrapartum care. Attending in-service training (AOR (95% CI): 3.5 (1.61–9.71)), accessibility of obstetric care guidelines (AOR (95% CI): 2.082 (1.222–3.547)), having regular case presentation (AOR (95% CI): 2.5 (1.234–6.743)), having knowledge (AOR (95% CI): 2.3 (1.222–3.547)), attitude of obstetric care providers (AOR (95% CI): 1.847 (1.065–3.204)), having less than 2 years of work experience (AOR (95% CI): 1.32 (1.012–3.56)), and having 2–5 years of work experience (AOR (95% CI): 3.49 (1.23–6.312)) were among factors significantly associated with evidence-based intra-partum care practice of obstetric care providers in Jimma Zone public hospitals.
Conclusions:
This study indicated that the majority of obstetric care providers did not practice evidence-based intrapartum care, which requires attention from all stakeholders. It is recommended for hospitals in the Jimma Zone to make guidelines available, provide in-service trainings, and identify systematic strategies to improve the knowledge and attitude of obstetric care providers.
Introduction
Each year around 300,000 women die during childbirth around the world. Death during pregnancy, delivery, or even weeks and days after delivery is extremely rare in settings with adequate healthcare facilities, advanced technology, and evidence-based healthcare practice. Maternal death during pregnancy and delivery is a serious public health concern in developing nations. While quality healthcare can prevent most maternal and infant mortality worldwide, hospitals are responsible for the majority of all maternal deaths. 1
Quality of care is a crucial priority to ensure fewer avoidable newborn and maternal morbidity and mortality. Evidence-based practice is an essential component of quality care, according to the World Health Organization’s (WHO) Quality of Care Framework for Newborn and Maternal Health, as well as numerous researches on the subject. 2 This is because healthcare based on the best available evidence can significantly boost the overall quality of care in general and the patient’s health condition in particular. Various studies in many developed and developing countries including in the sub-Saharan African region have also shown that intrapartum care which is based on evidence plays an important role in the improvement of maternal and child health outcomes.1 –3 This entails that evidence-based care (EBC) is the conscientious, explicit, and judicious use of the best available evidence in making decisions about the care of individual patients or populations The practice of EBC is supported by two factors: first, the availability of “‘recommended’ practices” “that are effective and generally facilitate the physiological process of birth. The second is to avoid ‘not recommended’ practices,” which are often invasive medical interventions that have proven ineffective or harmful if provided on a routine basis. 3
Research has confirmed the existence of gaps between established standards and their implementation with labor and monitoring duties often being omitted because of insufficient infrastructure and human resources. Also, abuse and inhumane treatment such as inappropriate interventions, continue to prevail in healthcare service delivery. A cross-sectional study from Sweden indicated that 22.7% proportion of applying evidence in intrapartum care, while 78% of women had received care in accordance with evidence from Iranian social security hospitals.4 –6 All these indicate that there is a major divergence between different settings and conditions in implementing evidence-based practice in healthcare, which signals the need to examine it more and fill the apparent gap. Moreover, another institution-based study in California, United States of America, indicated that women got evidence-based intrapartum care. 7
A multi-institutional Californian study found that age, profession, qualification, present position of care providers, gender, age, and job status were linked with evidence-based practice. 7 Several studies have demonstrated that age, gender, career, qualification, experience, access to the internet, workshops, conferences, and searching for the Cochrane database had significant statistical connections with evidence-based intra-partum practice.7 –10 All these show that evidence-based practice could be linked to numerous elements, and bringing it to the forefront of healthcare and making it the habitual practice of care providers may necessitate examining it from various viewpoints.
To counteract maternal and newborn death, evidence-based intrapartum care is the likely method supplied, mostly based on the timely and competent care desired in advance by women. 6 Although competent delivery is the most important factor in minimizing maternal death, new reviews of emergency obstetrics have indicated that obstetric care professionals have limited knowledge and poor abilities in detecting post-partum hemorrhage and birth asphyxia. 11
Evidence-based decision-making has been advocated to improve quality of health services. 3 Even though evidence-based practice has been advocated by healthcare authorities and facilities in Ethiopia, very little is studied about evidence-based intrapartum care and associated factors in Ethiopia and nothing has been discovered in the study area. Thus, the purpose of this study was to contribute to filling this important gap by assessing evidence-based practice intrapartum care practice of obstetric care providers.
Methods and materials
Study area and period
The study was conducted in nine public hospitals in the Jimma Zone, southwest Ethiopia between June 1 and 30, 2023. Jimma Zone is located 352 km southwest of Addis Ababa. In 2022/2023, the zone’s population was projected to be 3,090,112. The nine public hospitals are: two general hospitals, Shenengib and Limmugannet; six primary hospitals, Seka, Dedo, Dimtu, Omo Nada, Agaro, and Satamma; and one referral and specialized teaching hospital, Jimma Medical Center (JUMC). There were a total of 217 obstetric care providers available during the study period. Data were collected from June 1 to 30, 2023.
Study design
A facility-based cross-sectional study was conducted.
Source population
All obstetric care providers who were providing care for laboring mothers in the labor and delivery units of selected Jimma Zone public hospitals.
Study population
All obstetric care providers who provided care for laboring mothers in the labor and delivery units of selected Jimma Zone public hospitals during the study period.
Sample size determination
The study used a census approach to include all eligible intrapartum obstetric care providers in selected Jimma Zone public hospitals within the specified population. Hence, applying a certain specific sample size determination formula was not needed in the case of this study.
Sampling techniques
Every member of the study population was included in the study by using their list from each respective public hospital.
Inclusion and exclusion criteria
The study included obstetric care professionals who volunteered to participate and had at least 6 months of work experience. Obstetric care providers who could be absent or may not volunteer to participate were planned to be excluded, but the investigators encountered no such concerns.
Operational definitions
Recommended evidence-based intrapartum practice: Obstetric care providers who scored greater than or equal to 7 (the median value) on evidence-based practice-related questions. The median value was used as a cut-off value as the data on this variable were not normally distributed.
Nonrecommended evidence-based intrapartum practice: Obstetric care providers who scored less than 7 (the median value) on evidence-based practice-related questions. The median value was used as a cut of value as the data on this variable was not normally distributed.
Obstetric care provider: In this study, an obstetric care provider is one who is a certified health personnel who provides care for the woman during labor and delivery and is currently working in this area.
Good knowledge: Obstetric care providers who scored greater than or equal to 6 (the median value) on knowledge-related questions of intrapartum practice. The median value was used as a cut-off value as the data on this variable was not normally distributed.
Poor knowledge: Obstetric care providers who scored less than 6 (the median value) on knowledge-related questions of intrapartum practice. The median value was used as a cut-off value as the data on this variable was not normally distributed.
Favorable attitude: Obstetric care providers who scored greater than or equal to 5 (the median value) on attitude-related questions on evidence-based intrapartum practice. The median value was used as a cut-off value as the data on this variable was not normally distributed.
Unfavorable attitude: Obstetric care providers who scored less than 5 (the median value) on attitude-related questions on evidence-based intrapartum practice. The median value was used as a cut-off value as the data on this variable was not normally distributed.
Data collection instrument and procedure
Data were collected using a semistructured self-administered questionnaire adapted from a previously published article. 12 The questionnaire consists of 5 sections and 41 items. The first part of the tool is a sociodemographic section with seven items, the second part is factors/perceived barriers related to evidence-based intrapartum practice with five items, and the third and fourth parts of the questionnaire are sections used to assess the participants’ knowledge and attitude with eleven and eight questions, respectively. The attitude of the care providers was assessed using items developed on a scale, which were found valid and reliable with Cronbach alpha values of 0.84 and 0.87 in the previous and the present studies, respectively. The tool’s last section consisted of 12 items categorized as “recommended” and “not recommended” practices on selected areas of practice to measure the level of evidence-based intrapartum practice. The reliability and validity of the items used to assess the knowledge of participants and recommended and nonrecommended evidence-based intrapartum care practice were also taken to be good as they were used in studies conducted with similar settings in Ethiopia. Moreover, a pretest was conducted in a setting other than the study areas, and the items of the tool used were found to be both valid and reliable.
The questionnaire was originally developed in English and then translated into Amharic and Afan Oromo (the local languages spoken by the study participants) by language experts in all three languages. Back translation was used to ensure uniformity. Five trained data collectors with bachelor’s degrees in health-related professions collected the data by handing out questionnaires to each study participant while they were in the workplace. Data collectors introduced themselves to each study participant and clarified all pertinent information regarding the study and the instrument to ensure clarity. Verbal informed consent which was in full compliance with the institutional review board research ethics guideline was taken from each participant prior to data collection. Two trained master of science supervisors oversaw the data collection process and reviewed the completeness and quality of each tool every day.
Data processing and analysis
The collected data were entered into epi data version 4.2 (a data entry with customizable forms used for data entry, validation checks and for exporting in to softwares like SPSS which was developed by Epi Data association based in Denmark in collaboration with Jens Lauritsen and Michael Bruus which currently is integrated in to Epi Info by the CDC) and then exported to Statistical Package for the Social Sciences (SPSS) version 25 (a statistical software package developed by IBM for data analysis, data mining, and predictive analytics and is part of the IBM SPSS Statistics suite and was released in 2017) for cleaning and analysis. Binary and multivariable logistic regressions were used to determine the relationship between evidence-based intrapartum care and independent variables. Variables with p-values less than 0.25 in binary logistic regression of one independent variable with the dependent variable were included in the final multivariable logistic regression model and those variables whose p-values were less than 0.05 in the final model were taken to be statistically significant at 95% confidence level. The findings are presented using tables, percentages, figures, measurements of central tendency, and texts.
Data quality assurance
To ensure data quality, a pretest was conducted on 22 (10%) of obstetric care providers who were not currently working in the intrapartum care wards at JUMC in Jimma Town, South West Ethiopia. The questionnaire was modified based on the pretest results, including language and grammatical changes, as well as on the tool’s coherence and logical order, before being administered to the real study population. Before data entry, the questionnaires were checked for completeness. Data were entered into EpiData version 4.2 software which can automatically discover errors occurring during data entry. Furthermore, data collectors and supervisors received training on the purpose and procedure of data collection, and the supervisors watched the entire data collection process.
Results
Sociodemographic characteristics of obstetric care providers in Jimma Zone public hospitals
This study had a 100% response rate. The study included 217 obstetric care professionals from public hospitals in Jimma Zone. Out of the 217 study participants, 137 (63.13%) were females. The majority, 190 (87.56%) of participants were midwives. Among the midwives, 161 (84.74%) had a bachelor’s degree (BSc), with the remaining 29 (15.26%) having completed TVET level IV. Table 1 provides a comprehensive list of sociodemographic characteristics of participants.
Sociodemographic characteristic of obstetric healthcare providers in Jimma Zone public hospitals, Southwest Ethiopia, 2023 (n = 217).

Emergency surgeon, general practitioner.
Master’s degree, specialty, accelerated clinician.
Evidence-based intrapartum care practice
The study participants were asked about their utilization of various recommended and nonrecommended practices during intrapartum care. Overall, 89 (41.2%) of obstetric care providers in Jimma Zone public health facilities delivered evidence-based intrapartum care (95% CI: 32.9%–47%). Only 45.3% of obstetric care providers used partographs during the active first stage of labor. Table 2 displays the distribution of participant’s responses on the recommended practices during intrapartum care.
Distribution of recommended practice during intrapartum care among obstetric care providers in Jimma Zone public hospitals, Southwest Ethiopia, 2023 (n = 217).

It is noted in Table 3 that 31 (14.3%) of study participants reported applying fundal pressure on some occasions, whereas 120 (55.2%) reported performing vaginal examinations at intervals of less than 4 h. Participant’s responses on the nonrecommended practices are outlined in Table 3.
Distribution of nonrecommended practice during intrapartum care among obstetric care providers in Jimma Zone public hospitals, Southwest Ethiopia, 2023 (n = 217).

Perceived barriers to evidence-based practice during intrapartum care among obstetric care providers
As illustrated in Figure 1, 75.2% of the participants did not practice evidence-based practice as they believed that it would not bring any change to the patient. More than half, 113 (52.07%) of the respondents also reported that there is no appropriate consultancy among the different obstetric care providers and the remaining 104 (47.93%) of them said that there is appropriate consultancy.

Perceived barriers to evidence-based practice during intrapartum care among obstetric care providers in Jimma Zone public hospitals, Southwest Ethiopia, 2023.
Knowledge of participants on evidence-based intrapartum care
As indicated in Table 4, 160 (73.73%) of participants reported that they knew dilatation of the cervix in the first stage is assessed every 4 h and 30 (13.82%) of the respondents did exactly know that the end of the third stage is considered at the delivery of the placenta. The responses of participants on the knowledge items are indicated in Table 4.
Knowledge of participants on intrapartum care in Jimma Zone public hospitals, Southwest Ethiopia, 2023 (n = 217).

Attitude of participants on evidence-based intrapartum care
It is shown in Table 5 that 101 (46.54%) of participants strongly disagree that the adoption of EBP places too many demands on their workload. Moreover, only 42 (19.82%) of the participants reported that they strongly agree that the application of EBP improves patient’s healthcare outcome. Table 5 displays the remaining responses of participants on the attitude measuring items.
Attitude of participants toward evidence-based intrapartum care in Jimma Zone public hospitals, Southwest Ethiopia, 2023 (n = 217).

Factors associated with intrapartum evidence-based practice among obstetric care providers in Jimma Zone public hospitals
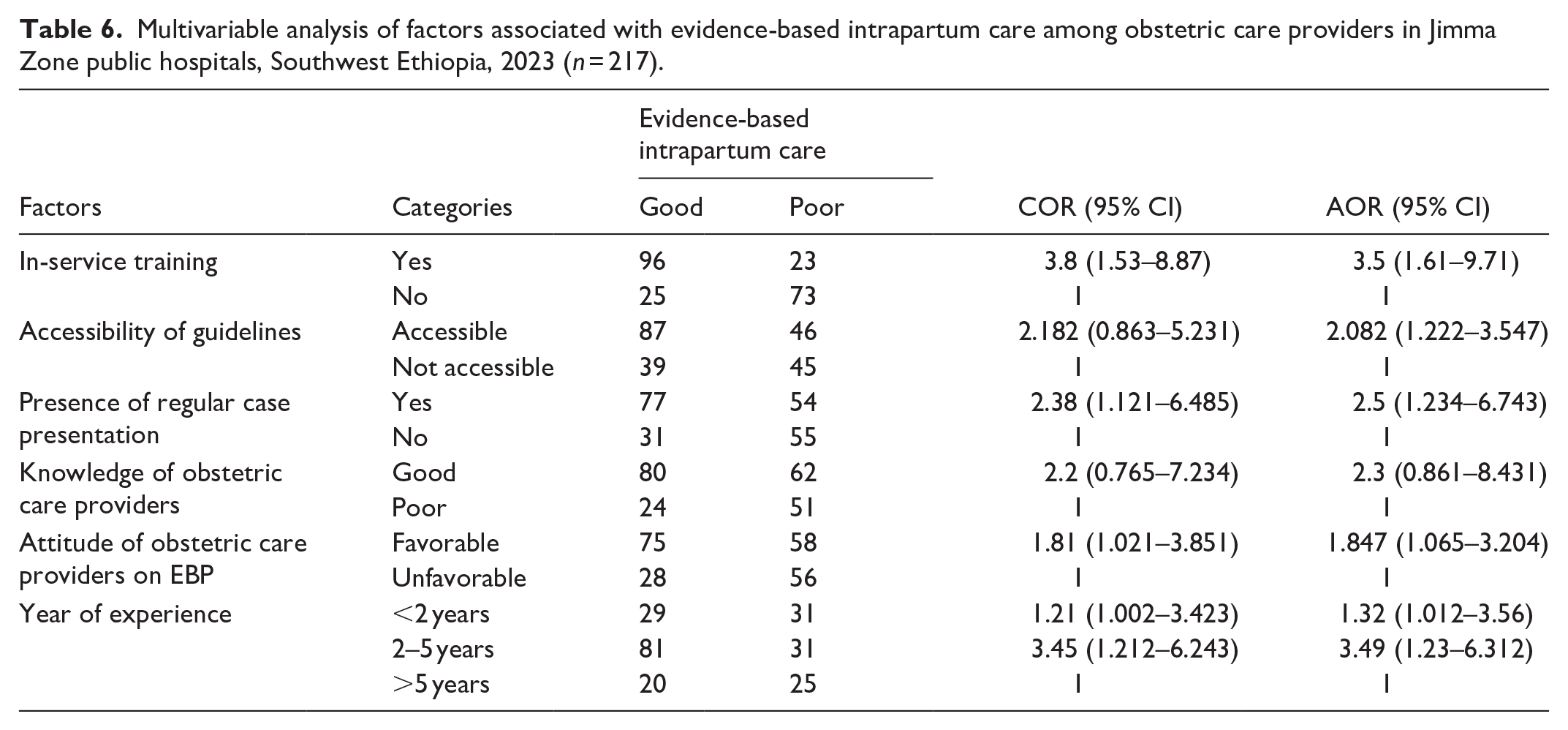
The final multivariable logistic regression involved predictors with bivariate p-values below 0.25. Stepwise backward likelihood ratio selection was used in selecting predictors. Intrapartum EBC is strongly associated with in-service education, the presence of national/international guidelines, frequent workshop/case presentations, and obstetric care providers’ knowledge and attitudes (p-value < 0.05). As a result, this study found that obstetric care providers who received in-service evidence-based practice training were nearly 3.5 times more likely to offer intrapartum care in accordance with the best national or worldwide protocol (AOR = 3.5; 95% CI: 1.61–9.71) than those who did not receive in-service training. Likewise, obstetric care providers who were given access to national/international guidelines were almost two times more likely (AOR = 2.082; 95% CI: 1.222–3.547) to provide intrapartum care according to national/international guidelines. Obstetric care providers who attended routine case presentation/morning sessions were 2.5 times more likely than others to utilize evidence-based intrapartum care (AOR: 2.5; 95% CI: 1.234–6.743).
The study also revealed that obstetric care providers who had good knowledge of evidence-based intrapartum care had 2.3 times (AOR = 2.3; 95% CI: 1.222–3.547) likelihood to practice evidence-based intrapartum care than those who had poor knowledge of evidence-based intrapartum care. Similarly, obstetric providers who had a favorable attitude toward evidence-based intra-partum practice were 1.85 times (AOR = 1.847; 95% CI: 1.065–3.204) more likely to practice evidence-based intrapartum care. Table 6 presents a multivariable analysis indicating the association between independent variables and evidence-based intrapartum care.
Multivariable analysis of factors associated with evidence-based intrapartum care among obstetric care providers in Jimma Zone public hospitals, Southwest Ethiopia, 2023 (n = 217).
Discussion
Evidence-based intrapartum care is an essential health concern championed in nearly all health facilities. This study aimed to assess the evidence-based practice of intrapartum obstetric care providers and its determinants. In-service education, availability of evidence-based guidelines of obstetric care, availability of case presentation at the work site, knowledge of care providers, attitude of care providers toward EBC, and the number of years participants have worked were strongly associated with the practice of evidence-based obstetric care by professionals.
According to this study’s results, 89 (41.2%) of obstetric care providers provided evidence-based intrapartum care. This was lower compared to a Benin study (70.1%) and a Rwanda study (65%). The difference may have been contributed by socioeconomic and sociocultural variations among study participants, experiences with various workshops and education on evidence-based intrapartum care, the three countries’ healthcare system, and a variation of study environment. Furthermore, the Benin and Rwanda studies were conducted in urban hospitals, while our study was conducted in both rural and urban hospitals.13,14
Furthermore, the study discovered that in-service training on evidence-based intrapartum care was substantially related to the participants’ evidence-based intrapartum care practice. This was demonstrated by the fact that obstetric care providers who received in-service training were 3.5 times more likely to deliver evidence-based intrapartum care than those who did not (AOR = 3.5; 95% CI: 1.61–9.71). This finding contradicts earlier findings in Sweden, Italy, and Cameroon. This inconsistency might be because there are variations in study populations, study sites, study designs, and sample sizes. The time of study duration variation might also account for this inconsistency since the current healthcare workers are more likely to receive and be exposed to routine and sophisticated in-service training than in the past.15,16
This study also illustrated that access to national/international protocols for obstetric care providers was strongly linked with evidence-based intrapartum care (AOR = 2.082; 95% CI: 1.222–3.547). This was consistent with earlier studies in Sweden, Cameroon, and the Amhara region in Northern Ethiopia. This may be so because compliance with national/international guidelines mainly contributed to evidence-based intrapartum care in the world.17,18
This study also discovered that having a favorable attitude toward evidence-based intrapartum practice was substantially related to evidence-based intrapartum care (AOR = 1.847; 95% CI: 1.065–3.204). Two studies conducted in Spain and the United States of America indicated a strong relationship between favorable views of healthcare providers and evidence-based intrapartum care.8,9,19 This significant link could be related to the fact that if a healthcare professional has a favorable attitude toward EBC, he or she is more likely to practice care provision based on existing evidence.
In contrast, a positive attitude toward evidence-based practice was not found to be a significant factor in determining healthcare providers’ evidence-based intrapartum care practice in an Italian study. This discrepancy might be due to the disparities in the healthcare system, variations in how obstetric care providers’ attitudes toward evidence-based treatment were formed by training and education, variation in the study period, and the items used in the tools to assess participants’ attitudes.4,20,21
This study also showed that there is a significant association between a higher knowledge of evidence-based practice and evidence-based intrapartum care (AOR = 2.082; 95% CI: 1.222–3.547). The findings of this study are consistent with those of previous studies conducted in Cameroon, the United States of America, and Italy. Knowing the value of evidence-based intrapartum care and how to practice it may lead to professionals providing evidence-based intrapartum care.1,9,19 Finally, this study has demonstrated that evidence-based intrapartum care practice is not at the ideal level, and there are extremely crucial factors associated with evidence-based intrapartum care practice which are in most cases compatible with what is shown in the prior studies.
Strengths and limitations
The study’s strengths include the utilization of primary data, a census to include all participants and a 100% response rate. The limitations of this study could include a lack of sample size computation and potential biases from respondents as a result of responding to a self-administered instrument.
Conclusion and recommendation
The current level of evidence-based intrapartum practice among obstetric care experts in Jimma Zone public hospitals is taken to be inadequate. In-service training, accessibility to guidelines, knowledge, attitude, regular case presentation, and experience were all significantly associated with evidence-based intrapartum practice. It is recommended that Jimma Zone health office collaborate with different stakeholders to improve evidence-based practice through providing various training. Moreover, hospitals in Jimma Zone should make guidelines accessible and find systematic ways to improve the knowledge and attitude of obstetric care providers. We recommend future researchers investigate further barriers to the application of evidence-based intrapartum treatment using observation checklists and possibly through other designs including qualitative methods.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251358969 – Supplemental material for Evidence-based intrapartum care practice and associated factors among obstetric care providers in Jimma Zone public hospitals, southwest Ethiopia: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121251358969 for Evidence-based intrapartum care practice and associated factors among obstetric care providers in Jimma Zone public hospitals, southwest Ethiopia: A cross-sectional study by Diriba Wakjira, Eneyew Melkamu Andualem, Azmeraw Bekele and Desalew Tilahun Beyene in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank all the study participants who voluntarily participated in this study and provided their valuable responses. We also thank the data collectors and supervisors for their patience and effort throughout the data collection process.
Ethical considerations
Ethical approval for this study was obtained from Jimma University Institute of health ethical review board (IRB) with Ref. No: IHRPG/201/2023 Additional permission to collect data was secured from each facility. Moreover, participants were informed about the objectives of the study and possible associated risks and benefits of participating in this study prior to data collection. Participation was entirely voluntary and the right to withdraw at any time from the study was assured. Participant’s identifiers like their name were not included in the data collection tool and all their responses were kept confidential.
Consent to participate
Verbal informed consent was taken from all subjects before the study. This was in full compliance with the Institutional Review Board’s research ethics guideline, as it was sufficient for studies of this nature and method.
Consent for publication
Not applicable.
Author contributions
DW: conceived the study, authored the original write-up, entered data, analyzed data, wrote the results, explained the study’s findings, and prepared the paper. EMA, AB, and DTB contributed to data analysis, results writing, study findings discussion, and manuscript preparation. The final manuscript has been approved by all authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated by this research and/or analyzed during the current study are available from the corresponding author through email upon reasonable request and at the appropriate time: enemelkamu@gmail.com
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.