
Abstract
Stigma towards People Who Use Drugs (PWUD) is reinforced through social structures and intersectional identities (e.g., gender, race, class). This often manifests as PWUD being The Other in society. This study aimed to explore how stigma manifests within the community environment using Community-Based Participatory Research framework and photovoice. Peer advocates (n = 15) from various Irish community-based organizations were trained in the photovoice technique to capture experiences of stigma. A series of seven focus group interviews were conducted. Photographs were analyzed using visual analysis, and interview data were analyzed using deductive codebook Thematic Analysis informed by Intersectional Stigma frameworks. The findings identified three major themes that demonstrate the multiple pathways through which social structures are used to reinforce stigma across intersectional identities possessed by PWUD
Keywords
Introduction
Globally, the social meaning of drug use is shaped by cultural norms, legal frameworks, and negative public attitudes manifesting as stigma towards People Who Use Drugs (PWUD). Stigma is a critical determinant of health, constraining the implementation of evidence-based interventions, impeding access to care, and reinforcing social and structural inequalities experienced by PWUD (Ahern et al., 2007; Link & Hatzenbuehler, 2016; Livingston, 2020; Van Boekel et al., 2013). Although its specific manifestations vary across sociopolitical contexts, stigma consistently functions to reproduce moral hierarchies, legitimize punitive policy responses, marginalize already vulnerable populations and negative embodiment (Stevens, 2019; Tyler, 2022). Understanding stigma towards PWUD as a phenomenon sustained through public discourse, institutional practice, and interpersonal interaction provides an essential foundation for examining its impact within national and local settings (Hatzenbuehler et al., 2013; Schomerus & Corrigan, 2022). Against this backdrop, this paper aims to contribute to the growing body of literature that interrogates the experiences of stigma experienced by PWUD, providing further insight into how it is produced, sustained, and how it can be potentially challenged in the Republic of Ireland (ROI).
Stigma in the Irish Context
There are various studies within the Irish context showing social stigma, or stigmatized attitudes held by the public, and structural stigma, or stigma enacted at the level of policy and social structures, towards PWUD. A cross-sectional survey by Bryan et al. (2000) identified that a significant portion of the population endorsed fear and social avoidance of PWUD. A more recent opinion poll identified similar (e.g., fear of PWUD) along with the public endorsing PWUD as criminals and favoring tougher sentences for drug misuse (Merchants Quay Ireland, 2025). A cross-sectional survey across the island of Ireland found moderate endorsement of stereotypes and discrimination towards PWUD with a lack of sympathy being a significant predictor for lack of policy support for interventions to reduce drug-related deaths (e.g., naloxone, supervised injection facilities) (Miller et al., 2025). At a structural level, stigma is experienced by PWUD in methadone maintenance treatment (MMT), including poor institutional practices and use of stigmatized language in care (Healy et al., 2022). While another qualitative study using one-to-one interviews of the older Irish population undergoing an MMT program found participants concealed attendance to the program, experienced public shame of being older and engaging in MMT, and social isolation (Mayock & Butler, 2022). Additional qualitative studies identified social and structural stigma as a barrier to the implementation of interventions to reduce drug-related deaths (Atkin-Brenninkmeyer et al., 2017; Miller et al., 2023; O'Shea, 2007).
Other qualitative studies have identified the link between economic status of PWUD, such as being from a lower economic background (i.e., poverty), with being marginalized from local communities, the education system, and social stigma of drug use (Cambridge et al., 2022; O'Connor et al., 2026; O’Gorman, 2005; O’Mahony, 2025). A study using in-depth semi-structured interviews found economic deprivation, loss of community, adverse events in the family, and stigma were contributors to drug-related harm in Cork city (O’Mahony, 2025). Cambridge and colleagues (2022) identified that stigma of poverty was linked with withdrawing from the community and engaging in crime, with substance use stigma was a barrier to recovery. O’Gorman's (2005) work using in-depth interviews and an ethnographic study of deprived areas in Dublin Ireland, identified how the stigma of economic deprivation and being unemployed were connected to heroin use, creating a risk environment for drug-related harm and experiences of social stigma. Similar results were found in a recent report which identified the link between poverty, violence, and drug use in Dublin (O'Connor et al., 2026).The research on stigma in the Irish context is extensive, however, the integration of creative methodologies such as photovoice to explore how stigma manifests and is reinforced within the spatial environment has not been explored.
Photovoice
Photovoice (PV) is a creative methodology that integrates the tradition of critical theory, feminism, and documentary photography by engaging with communities to analyze and showcase local knowledge through a participatory research project (Liebenberg, 2022; Wang & Burris, 1997). This process builds capacity by providing skills in participatory photography. It also incorporates group work where trainees can engage critically with their own living and lived experience through photographs, relate this to wider society, and showcase community strengths to generate social change. In addition, the training group designs a dissemination plan for their project to ensure their collective voices are communicated to key stakeholders. Other qualitative techniques, such as ethnography or in-depth interviews, can explore lived experience, however, does not always aim to generate social change between participants and wider society as the main outcome of the project. In addition, PV can generate more data (e.g., emotions and thoughts) through discussing pictures. This allows for critical reflection on the process and meaning of picture-taking, which enriches exploration of living and lived experience in comparison to other qualitative methods such as one-to-one interviews, focus groups, or ethnographic studies (Liebenberg, 2018).
Numerous studies have used PV to explore the lived experience of PWUD where stigma is explored or revealed. Studies range in their aims
This paper reports on the outcomes of a larger study that aimed to co-develop a stigma reduction campaign using multimodal techniques of photovoice and digital storytelling. Although stigma is prevalent in Ireland, a coordinated stigma reduction campaign aimed at exploring ways to reduce stigma is limited in the Irish context (Barron et al., 2019; Citizens Assembly, 2024). This study conceptualizes stigma as an intergroup behavior process using the Stigma of Addiction model (Corrigan et al., 2017) which outlines stigma as being a combination of stereotypes (PWUD are worthless), prejudice (anger, fear), and discrimination (social rejection, reduced opportunities) towards PWUD. This process can be enacted at the public level or as a form of social or community stigma. The term community stigma was incorporated within the research question for ease of understanding for participants. In addition, stigma enacted by social structures was explored by integrating the intersectional stigma framework, (see methods section). In short, this framework outlines where stigma is maintained and reinforced across various structures of society based on social locations or marginalized identities (e.g., class, ability, gender, citizen status and sexuality) possessed by PWUD (Collins et al., 2019; Earnshaw et al., 2022).
As this study produced a rich data set, we present findings from the photovoice study. We plan to publish solutions to reduce stigma (Miller et al., 2026) and the implementation of the digital storytelling campaign in separate journal articles. Building on the literature related to stigma and drug related harm in Ireland, this paper addressed the research question “How does community stigma manifest towards People Who Use Drugs?”.
Methods
Design
This is a qualitative study using the Community-Based Participatory Research (CBPR) framework (Israel et al., 2005; Wallerstein et al., 2017) using the photovoice method (Wang & Burris, 1997). The lead author was the main academic partner for the study (NMM). Values from the Peer Partnership For Change Framework (PPFC) (Kelly et al., 2024; Union for improved Services Communication and Education, 2022)
Epistemology and Positionality Statements
The main academic partner (NMM) ontological and epistemological stance is based on the Transformative Paradigm, which assumes reality is socially constructed with an emphasis on acknowledging social positions associated with power and privilege (Mertens, 2009; Mertens, 2017). In terms of epistemology, Transformative Paradigm assumes knowledge is produced between the researcher and participants; this knowledge is socially and historically situated and can be used for social justice and transformative change. The process of research then becomes “knowledge for change” (Liebenberg, 2022, p. 269). The researcher in this position aims to be aware of their own biases that can influence relationships with the participants and to recognize the validity of local knowledge. In terms of practicality, the main academic partner kept a research diary for personal reflection during the research process where questions of power, knowledge, social positioning, and social change were explored. Positionality statements from all the authors are listed in online supplement one.
Participants
Fifteen participants were recruited into the study through snowballing techniques (Sadler et al., 2010). The average age of the sample was 52.5 years old. Most of the sample (n = 11) identified as male with the remaining identified as female. Most lived in an urban environment (n = 12). The length of being in a peer advocacy role ranged from three weeks to two years. The inclusion and exclusion criteria of the study were provided to UISCE coordinator (AOH). AOH provided these criteria to the UISCE peer outreach team, who recruited from Merchants Quay Ireland peer team and the National Drug Treatment Centre peer advisory board. The inclusion criteria consisted of peers
Materials
An online Qualtrics survey was created that contained a participant information sheet, consent, and demographic data (sex, age, area of residence, length of participating in advocacy). The interview schedule for each focus group can be found in online supplement two. This includes a list of questions to trigger discussions about photographs and how these relate to experience of and ways to reduce stigma.
Community-Based Participatory Research Procedure
Keeping in alignment with the principles of CBPR, peers were involved with all stages of the research; however, with various levels of engagement. To start, the project was initiated by peers within UISCE. The peers nominated the peer coordinator AOH to speak on their behalf and collaborate with the main academic partner NMM on the research proposal, budgeting, research questions, and ethical processes. This allowed for equitable power sharing between the NMM and the peers in designing of the project. Participants were provided with informed consent, information sheets, and debrief forms via a Qualtrics link before the Photovoice training. The Photovoice training and picture viewing sessions were implemented over two 5-h workshops by NMM. The first workshop training started with a brainstorming session between the main academic partner and the peers about experiences of stigma, locations within the community where these experiences occurred, and ways to change stigma. These sessions were interactive and incorporated PPFC values of equality, respect, honesty, and compassion where peers were given time to input on their experiences. Peers were then trained in (1) photo literacy (2) dialoguing photographs, (3) practicing picture taking (4) how to caption photographs to display meaning and (5) ethics of photography to build capacity to engage in the research project (Catalani & Minkler, 2010; Miller, 2024). To establish equitable involvement in picture taking, peers worked closely with another designated peer if they were not confident in picture-taking or did not have access to a camera. The designated peer would take a picture on their peer's behalf, with the understanding that the picture would remain the peer's property.
Picture-taking was iterative such that peers uploaded pictures over time. This process facilitated the development of critical engagement with their own experience, their photographic ability, and understanding of captioning. For example, peers would work with peer coordinators from UISCE to review their captions, discuss the pictures, and decide whether more pictures should be taken. In addition, the iterative nature allowed peers to develop their understanding which reduced pressure related to the time-consuming nature of the methodology.
The second workshop consisted of reviewing how to capture solutions to reduce stigma (results reported in a separate article Miller et al., 2026). Peers uploaded their pictures and captions to the online Padlet system and attended a focus group four weeks after their training to discuss their pictures. Last, peers and the main academic partner viewed pictures together in a small photography exhibit where they analyzed the pictures together as a group and shared decision making over what pictures were shortlisted for the final campaign. There were 198 pictures taken in total across 15 participants. Participants shortlisted 70 pictures for the final digital storytelling campaign. Peers were compensated for their time with both cash and vouchers worth €10 for each PV workshop and focus group session.
The nominated peer coordinator AOH provided feedback on the analysis of the results and on the development of the manuscript. The results of the project were presented in series of large and small targeted community events to generate social change. Each event involved a collaborative presentation between a nominated peer and the main academic partner NMM.
Data Analysis
All focus groups were audio recorded and transcribed. Photographic data were analyzed using visual analysis as outlined by Collier (2001). The visual analysis was conducted in three stages. The first stage was open viewing where the team reviewed the pictures without captions. Careful notation of impressions, questions, and other observations were written during this stage. The second stage was an inventory where photographs were inventoried based on content, for example, whether the picture had objects, places, locations (named locations) and specific aesthetics. The third stage included a structured analysis of notations of the picture into a visual matrix adapted from Russinova et al. (2018). This included notation of a) picture caption b) concrete meaning such as a description of what was in the picture c) symbolic meaning or any metaphorical meaning in the concrete image and d) abstract meaning of the picture and caption with a focus on how stereotypes, prejudice, and discrimination were demonstrated in the photograph (Corrigan et al., 2017).
The focus group interviews were coded using deductive codebook Thematic Analysis (Braun & Clarke, 2019). In alignment with the Transformative Paradigm, the use of intersectionality frameworks allowed the researcher to explore how social structures and systems of power operated to sustain and ways to reduce stigma. Intersectional stigma is a useful model to identify how multiple social structures use power to oppress marginalized identities across multiple levels of society. For example, social structures can reinforce stigma associated with social location related to class, ability, gender, citizen status, and sexuality (Collins et al., 2019; Earnshaw et al., 2022). Thus, intersectional models can help deconstruct this relationship to reduce stigma (Collins et al., 2019; Crenshaw, 1991; Earnshaw et al., 2022). Intersectional Stigma (Earnshaw et al., 2022) and Intersectional Risk Environment Framework (IREF) (Collins et al., 2019) were used as the primary theoretical frameworks as opposed to intersectional theory for ease of coding. The IREF was used to help generate codes for social locations of participants (e.g., class, ability, gender, and sexuality). For the purposes of this analysis, social locations were defined as follows 1) class related to housing status and employment and 2) ability was associated with mental health, and 3) gender referred to peers connecting their experience as an identified woman or man. When codes did not apply to the framework, they were inductively coded based on the semantic and latent meaning aligned with hybrid coding approaches (Fereday & Muir-Cochrane, 2006). After the initial codebook was established, the data was mapped according to Earnshaw et al. (2022) Intersectional stigma framework to outline how social structures can perpetuate stigma. This framework outlines how stigma manifests as 1) Multidimensional-describing the various social locations of the participants 2) Multilevel- or notation of social structures where stigma manifests. This may include structures such as health care systems, criminal justice or the police, and urban architecture and 3) Multidirectional- meaning where one social structure reinforced stigma in another structure. Those experiences that did not fit within the Intersectional framework were kept as negative cases to ensure that peers’ experiences were still acknowledged. The last stage involved synthesizing both the visual and focus group data by blending the meta-inferences (Schoonenboom, 2022) or the claims being made by both data sets to provide a comprehensive narrative.
Ethics
This study aimed to address common ethical concerns in photovoice (Ng et al., 2024). As experiences of stigma can carry some risks, this was mitigated in several ways. The academic partner engaged in debriefing sessions with the coordinator and academic team members to discuss experiences of interviews and PV training. Ethical guidelines included informed written consent, the ability to withdraw or to not discuss sensitive content. If a participant was distressed during an interview, they were given the opportunity to pause or stop the interview entirely, while given the space to discuss the distress with the coordinator AOH. The project was approved by the University of West London Ethics Committee (UWLRECPSW-01589).
Quality
Trustworthiness was established through team coding. The main academic partner, (NMM) acted as the lead analyst. The academic partner along with a research assistant RB implemented all visual analysis and the analysis of focus group interviews. Coauthor LLC conducted a visual analysis of 50% of the photographs and coauthor GL coded all focus group interviews. The analysis of the pictures and focus group interviews involved debriefing sessions to review consistency and completeness of coding. This included reviewing where codes were similar and diverged, discussing discrepancies, synthesizing codes that had similar content, and agreeing on a codebook.
The Community Engagement in Research Index (CERI) instrument was used to identify levels of participatory engagement with the main academic partner and the participants (Khodyakov et al., 2013). Engagement rated on a Likert scale of 1–3 (1 = community partners were not involved to 3 = community partners were engaged in the activity) across 12 items. The total score is divided by three
Findings
The analysis identified three major themes that described how various social systems (e.g., the local community, housing sector, mental health and social care sector) reinforced and sustained stigma through various social locations possessed by the participants, common stereotypes towards PWUD, and discrimination. These experiences were often multidirectional, meaning one social structure or level reinforced stigma in another structure.
Theme 1: Class and the Accommodation Sector
Peers’ experiences demonstrate how the accommodation sector, class, such as being unhoused and having no income, and negative attitudes towards PWUD work together to perpetuate stigma. To start, one peer perceived that people who are unhoused become “institutionalized” (Figure 1 caption) by the state. Continuing they discussed the connection between being unhoused and being a person who used drugs and stigma. This stigma manifested as a form of social rejection and desensitized attitude towards people living on the streets. This stigma was reinforced by making it socially acceptable to perpetuate homelessness as expressed as “bodies all over the city” in the next quote: “I think it says something about the sort of national attitude to drugs and homelessness. It's not just the fact that the authorities have an attitude to it. It's like we have actually come to accept and it's perfectly alright to throw bodies all over the city.” (Focus Group 6, Peer 1)

These sleeping bags are all over the city and are a sign of institutionalized homeless people. The people who use them are usually drug users and from that stigma lives.
The peers were also aware of how possessing multiple marginalized identities based on class, such as being unhoused and in poverty, a criminal record, and drug use stigma legitimized discrimination in the form of social rejection. This social rejection was perceived by the peers to sustain homelessness. A few peers shared: Right. Nine times out of ten, people that were experiencing homelessness have either got a criminal record, or are in addiction, or ill, and poverty stricken. Um, those things go hand in hand…so it's easier to ostracize them (Focus Group 6, Peer 1). The most stigmatized people are IV drug users, people with, um, the, some of the diseases that result, long term homeless, especially street dwellers and, uh, working girls. We're a completely ignored group… (Focus Group 7, Peer 1). Caption: You can’t stay here, even in public spaces like library's n parks no one wants us and we get harassed just for existing… dis is the first sight confronts me every morn. Reminding me it don’t matter how crappy I feel, takin a breath n a rest ain’t for the likes of me. It makes me sad every time. With shops because you're sitting outside like business and that. They come out and they throw water and dirt. Oh, you can't sit there, or they'll go to ring the guards and get you moved on… And if it's not the businesses, its people walking past, like there could be a gang of a youths gone past and they’d start with the girl, and they kick her and throw stuff (Focus Group 3, Peer 2). The violence is horrific and bullying and drug use, like you're forced into it a lot of the time because people want your money… As soon as you go into a hostel, they know you want disability or job seeker, what day you get paid, you literally get followed to the f** ATM. You know, you can't stay clean in those places (Focus group 7, Peer 1). You're coming from homelessness, you're coming from drug addiction, you're not rocking up with loads of money in your bank account. You're going to be looking rough, and they already have their opinion, their mind made up, that you're not going to get anywhere…and they prejudge you and you just get nowhere and you're back into the cycle of homelessness and drug use (Focus Group 7, Peer 2).

Tho, it supposed to be our fault n everyone judges us, we ain’t allowed to follow or even try to better ourselves…these spikes is the window opposite my methadone clinic. I’m always exhausted n still feeling sick leaving, so I try find somewhere to sit n roll a smoke, n dis is the first sight confronts me every morn.reminding me it don’t matter how crappy I feel, takin a breath n a rest ain’t for the likes of me. it makes me sad every time.

This girl was stigmatized for being homeless.
Theme 2: Class-based criminalization — “It's almost like racial profiling”
The second theme demonstrates experiences of discrimination by police. Some of these stigmatizing experiences were based on class, and two social structures, such as the criminal justice system and social assistance to acquire accommodation, working together to reinforce stigma. This manifested in Class-based criminalization
Peers shared experiences of being targeted by police. Police behavior was “like racial profiling” (Focus Group 6, Peer 2) based on living in a specific estate (class) or an area known for high economic deprivation. One peer described being publicly humiliated where they were stopped, searched for drugs, and assaulted by a police officer in front of their mother. This experience suggests that being from a lower class enables discrimination in the form of illegitimate use of force by police. The peer stated: And they always justify it by your background…from living in, uh, living in XX Me and my little brother and one of my best mates from the flats …And that, any time we were seen, we were stopped and searched even in front of our mother, and that used to be shame for the kids, yeah, getting searched in front of your mother. Then you'd be getting battered… (Focus Group 6, Peer 2). Because got stuck with the guards…To see if he got drugs, and he had to drop, take off all his clothes and made him squat and all that. You know what I mean? And the stigma of that and he came back up, and he actually broke down in front of me and started crying. (Focus Group 1, Peer 3)
Looked down at for being on drugs and homeless and no support because he is just looked down on and judged instead of been supported.
Upon release from prison, peers were misled to believe they would get social assistance to find housing. For example, peers were referred to the “free phone” (Focus Group 4, Peer 1) a government support service, when released. This type of referral was a dead end, taking away hope, fueling disappointment, reinforcing a cycle of class (homelessness) and sleeping rough in the streets. In addition, a prior criminal history also reduced opportunities to access proper employment “You can't get a job” (Focus Group 2, Peer 1) continuing the cycle of economic deprivation and inability to acquire housing after leaving prison. Two peers share their experiences: I got eleven and a half years, with a year and a half-suspended sentence so I've done seven out of that. When I got out the first thing that's supposed to get you to these places when you're in prison, but they don't. They just throw you out, and you have to ring the free phone (Focus Group 4, Peer 1). I'd ring the free phone, and if the free phone hadn't got a bed for you, they say go to such and such and get a sleeping bag (Focus Group 4, Peer 2).
Theme 3: Inadequate Mental Health and Family Social Care Systems
The last theme demonstrates how ability, such as having previous mental health issues, class, and structural stigma in mental health clinics and the family social care system, worked to reinforce and maintain stigma. The first subtheme Structural stigma, lack of access, and class demonstrates how current mental health issues, strict rules associated with access to mental health treatment, and low-income reinforces structural stigma towards PWUD. The second subtheme “Constant fear of losing our children” gender-based stigma within the family and social care system outlines how gender, and class, reinforce discrimination within the family and social care system.
Structural Stigma, Lack of Access, and Class
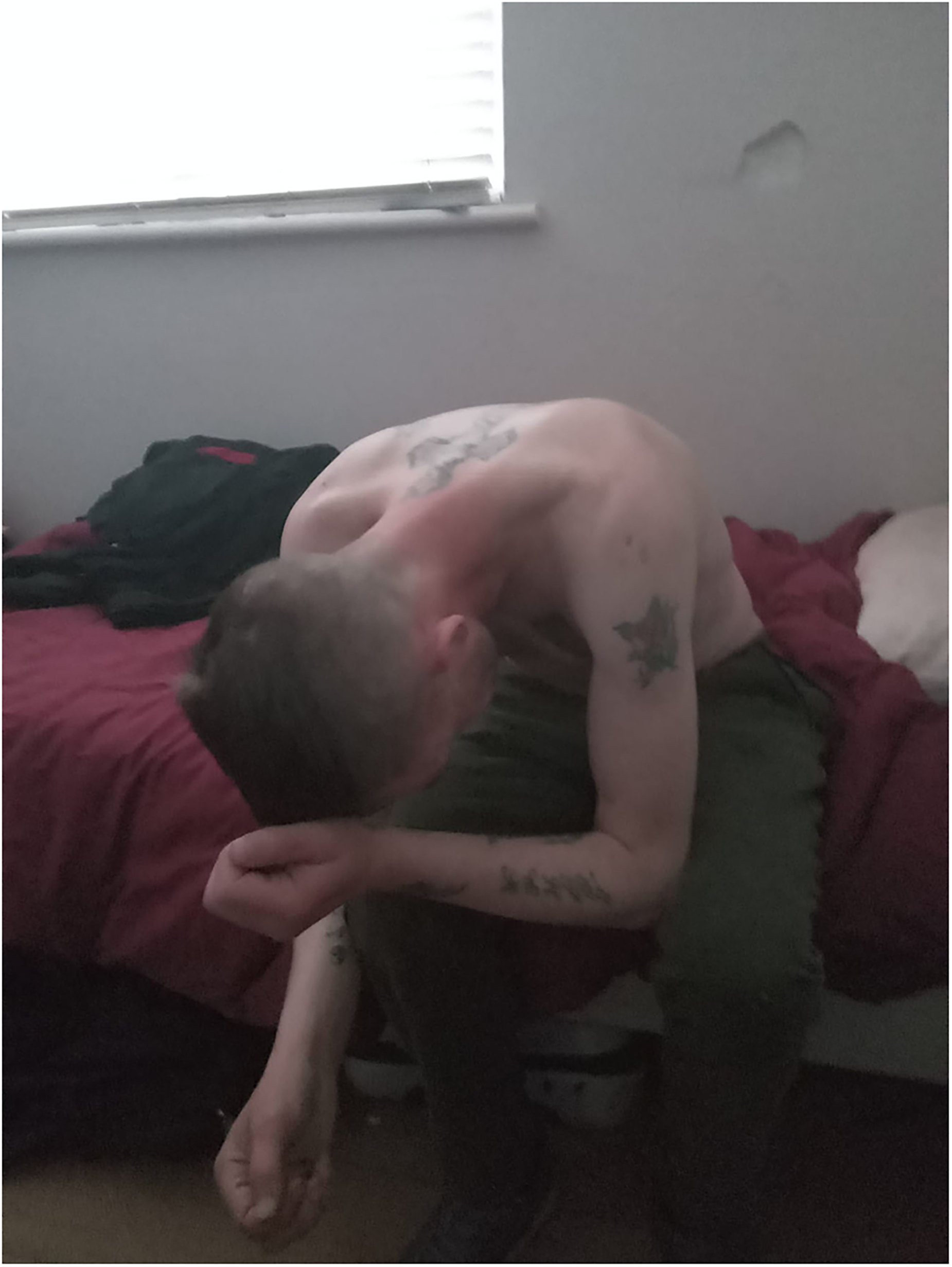
Peers who had both mental health (ability) and who attempted to stop using drugs had negative experiences within mental health clinics. Stigma in this context was detrimental as peers would anticipate being stigmatized and then actively avoid seeking care in mental health settings. One peer described taking several overdoses because of poor mental health and always having to call an ambulance. The ambulance was the only safe space where they never felt stigmatized because “I have been stigmatized when it comes to the hospital” (Focus group 1, Peer 2).
Some peers described strict and unrealistic rules to obtain access to care in mental health clinics suggesting structural stigma (stigma within policies) at work. This included refusing service to people who were still using drugs “The (name removed) department of psychiatry will not help you, mentally, at all, unless you are not using drugs” (Focus Group 7, Peer 3). This stigma was reinforced by their class, where they could not obtain private services due to their low income, and had to use state services involving long waiting times. Delays in accessing treatment were detrimental as it enabled poor mental health and suicidal ideation. A peer states, “So instead of you getting dealt with there that day it could take you 18 months…that makes you want to feel like you want to put a gun up to your head” (Focus Group 7, Peer 3). Figure 5 was taken to showcase their experience.

Have an anxiety condition and told they won't treat me when I am using drugs. But I was self medicating with them. Catch 22 situation. Means you have to lie to psychiatrist about what I am really doing.
“Constant fear of losing our children” gender-based stigma within the family and social care system
There were common experiences that suggested gender-based discrimination, namely being unfairly treated as a Women Who Used Drugs (WWUD), occurred with the family and social care system and with the police. This awareness of the dynamics of being a WWUD came with feelings of “constant fear of losing our children” (Focus Group 5, Peer 1) and limited the ability to ask for support if they wanted to stop using drugs “I feel that women, you know are more fearful and reluctant to reach out for help due to that stigma.” (Focus Group 5, Peer 1). Instead of getting help peers felt they were punished by the family and social care system, which led to further marginalization. A peer described creating a scene or staging a picture to symbolize feelings of stigma experienced by women. This was showcased with several women standing with their backs to the camera to represent feelings of shame (Figure 6). A peer stated: Because women, like, with kids, automatically are terrified your kids are going to be took. That's what happened with me, because I wanted to get into treatment, even though I was still clean. Yeah. It didn't matter. The kids were still taken till I got out of treatment (Focus Group 4, Peer 4). They also went and actually done door-to-door inquiries to all my neighbors. Asked them, was there any change in me, what was I doing, and everything else. So that was another thing. Even though I haven't been in trouble in two and a half years, they still reacted within minutes (Focus group 4, Peer 4).

Women who use drugs can't ask for help they have to hide the fact that there are addicted due to discrimination and stigma. We live in constant fear of losing our children.
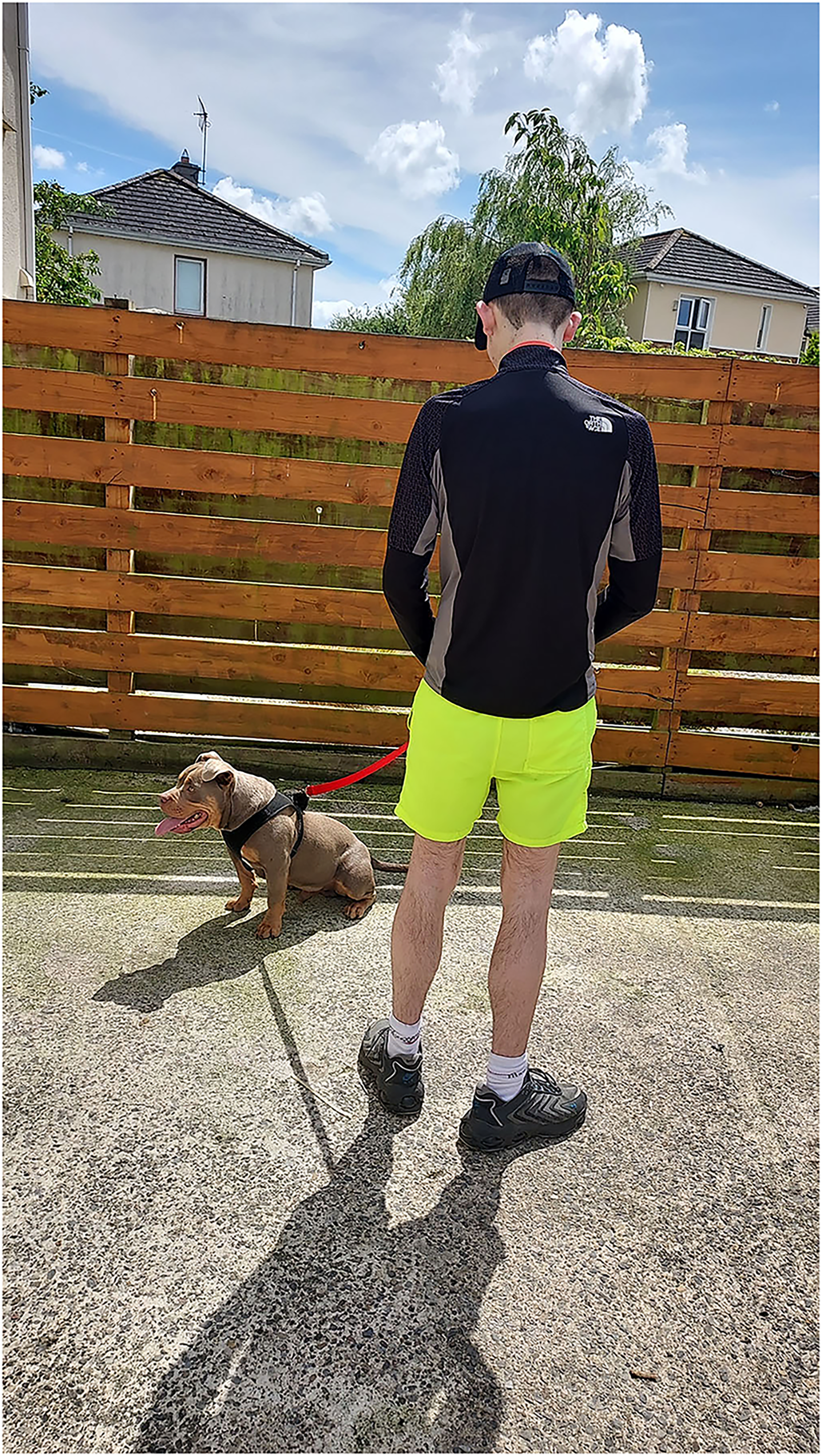
Drug dealer because of a family pet- nowadays people are breeding “bully dogs” but people have this perception that if you have this dog your involved in drugs. In the Guards eyes I went from being a drug user, to being a drug dealer because I had this type of dog.
Negative Cases
Data that did not fit within the intersectional framework and was relevant to the research question was grouped under a series of negative cases. This included evidence of stigma toward PWUD that did not necessarily relate to a social location. This included internalized stigma, experiences of family stigma, and being discriminated against by police. To start, some peers expressed being excluded or “not part of society (Focus Group 7, Peer 1). This sense of exclusion manifested in “hide behind the bushes looking out at what could be” (Focus Group 1, Peer 4) suggesting an awareness of their desire to be both a part of society but also knowing that their identity as a PWUD is socially unacceptable.
The peers provided examples of negative attitudes towards PWUD in the community, more specifically the city center, neighbors, and within their own family. Some were barred from shopping centers by security “They won’t even allow you in” (Focus Group 2, Peer 3) with some incidences of public displays of discrimination “They'd make a show in front of everybody.” (Focus Group 2, Peer 1). Peers described how their family members were stigmatized by the local community. For example, a peer described how their mother encountered negative attitudes from local community members about their behavior while using drugs: …for her whole life, she had to be approached by people saying things about me. And she had to stand up and say, no, that didn't happen and pick up for me. And sometimes it might have happened. And just because I was her son, She took the stigma (Focus group 1, Peer 3)

My mother took allot of stigma in the area over my drug use.
Family members were reported to endorse typical stereotypes of PWUD and enacted stigma on their loved ones “My family stigmatized me because I was addicted to those tablets like I was a junkie. I was a everything…every name you can call under the sun for being on drugs.” (Focus Group 3, Peer 2). This stigma continued after they stopped using drugs “Even when you're doing well. It's still there” (Focus Group 3, Peer 1). Family fears were aired “I think they're afraid that when I do fully, when I do fully finish with the methadone that I'll probably go back to heroin, but I'll never go back to heroin, no.” (Focus Group 3, Peer 1). Family members were suspicious “But when they start saying things to me. Saying like you’re fairly loud you must be on something or you're talking too much you must be on something” (Focus Group 3, Peer 2). This demonstrates how hostile social conditions towards PWUD can erode the family system - a vital resource for belonging.
Peers also encountered ‘acceptable violence’ from the police. The police denied wrongdoing invalidating these experiences and instead blamed PWUD. Two peers describe their experiences: But they battered me that night and I went to court the next day, black and blue. And my solicitor said it to the judge that she seen me at 8 o'clock that night…but the next morning she seen me, I was black and blue. But the guard says that I am, I was banging my own head off the wall and I made all the injuries up myself (Focus Group 5, Peer 3). But yeah, here you are with a woman, a female in handcuffs, and you had to give her such a dig into the side of her ribs. You've broken her ribs…. this guard is trying to say that I've done it to myself, But it wasn't, it's not physically, it wasn't physically possible (Focus Group 5, Peer 1).
Discussion
The experiences of the peer participants demonstrate how stigma was reinforced based on multiple intersectional identities and across various social structures. Stigma involved multiple social locations as 1) class, such as lack of housing and being employed 2) gender, such as being a woman, and 3) ability, peers who had mental health challenges. The social structures involved the accommodation sector, urban city architecture, police, mental health system, and the family and social care system. Some of the experiences of stigma were multidirectional where one level of stigma (e.g., upon release from prison) reinforced stigma in another (e.g., social assistance for housing).
The results support existing research exploring stigma towards PWUD and demonstrate some novel findings. Public and police discrimination in the form of physical and verbal abuse and lack of opportunities to obtain housing, demonstrate how various social structures enact power over the physical body of PWUD and reinforces stigma as a form of embodied shame as discussed in Tyler (2022). Internalized stigma and negative health care interactions were common as in other studies (Austin et al., 2022; Batchelder et al., 2021). As in previous research in the Irish context, class-based poverty related stigma (Cambridge et al., 2022; O’Gorman, 2005; O’Mahony, 2025) was a common experience across the data set mostly relating to being unhoused and living in areas of high economic deprivation. Our research further clarifies the mechanisms in which social structures reinforce and maintain stigma towards PWUD based on class. For example, being unhoused reinforced social rejection of PWUD. The spatial environments within the urban city center contained hostile architecture (Glynn, 2024; Petty, 2016; Preece, 2020) which appeared to reinforce internalized stigma for those peers who were unhoused. Prior homelessness was also a ‘mark’ that enabled discrimination as evident by reduced opportunities to obtain housing in the accommodation sector. The experiences also show how living in areas of economic deprivation legitimized police discrimination in the form of unnecessary violence. Gender-based stigma, although a minority view, were in fact a part of how some participants navigated the family and social care systems as shown in previous work (Lucey, 2025; Meyers et al., 2021; Vu et al., 2019). The current study demonstrates how gender-based stigma is a barrier to seeking help for WWUD. This points to the importance of emphasizing the social location of PWUD into stigma reduction training and future campaigns. Last, the negative cases showed some evidence of novel findings, namely the effects of stigma on the family members of PWUD, as it adds to understanding of how increased familiarity may motivate family members to enact stigma on their loved ones due to the social pressures they face by their community and larger society (Corrigan & Nieweglowski, 2019).
Intersectional Informed and Contact-Based Stigma Reduction Training and Campaigns
This research points to the importance of making anti-stigma training a requirement for those who encounter PWUD in mental health (e.g., psychiatric offices) and non-clinical (police, housing) contexts in Ireland and internationally. Taking an intersectional approach, which involves the recognition of how social structures may reinforce marginalized identities based on social locations
Policy Recommendations
Policies involving prisoners upon release currently provide several resources to integrate back into the community (Irish Penal Reform, n.d.), however can improve by providing a service dedicated to housing support. Irish housing policies should reinforce non-discrimination clauses based on low income and prior experiences of being unhoused to support PWUD entry into the housing market. This applies to international contexts where housing and drug use stigma are a public health issue. Criminalization was also described as a reason for the lack of opportunity to improve income, which in turn related to reduced access to housing. Decriminalization is associated with reducing stigma, arrests and over policing, reduced social costs of crime and the potential to reduce poor mental health outcomes (Grucza et al., 2018; Mohebbian et al., 2025; Sigaud et al., 2024; Stevens et al., 2024) suggesting the benefits it can provide to PWUD in the Irish context. Hostile architecture is used to socially exclude marginalized groups in the urban environments across the globe (Annan, 2021; McCreath, 2025). The effects are further compounded in areas of high rate of homelessness such as in Canada (de Fine Licht, 2020; Rosen, 2023) and the United Kingdom (Nielsen, 2025) leading to poor sleep quality for people who are homeless, generating poor health outcomes (Edmed et al., 2025) and continue stigma (as outlined in this study). This type of architecture should be reduced and replaced with community-based initiatives that are inclusive of PWUD. This is in alignment with Lefebrve's right to the city framework where urban space is co-produced with all citizens involved to reduce alienation and generate belonging (Aalbers & Gibb, 2014). In addition, national advocacy groups like UISCE and a social determinants of health approach should inform the National Drug Strategy in Ireland (Conneely, 2026) and internationally to ensure equitable care and reduce stigma towards PWUD who have multiple marginalized identities.
Strengths and Limitations
There are several strengths and limitations to this study. Some strengths include the integration of the CBPR, namely PV, as it provided a critical space for peers to engage in thinking about their experience. The use of CBPR monitoring ensured equitable engagement of the peers in the research process. As mentioned, the intersectional approach allowed for identification of fine details of how stigma operates across the social environment, while helping to outline key stigmatizing processes that are often not captured in other frameworks. Data quality procedures ensured robustness of the analytical process. In terms of limitations, qualitative analysis is context dependent, and the experience cannot be generalized to all PWUD across Ireland. Experiences of intersectional identities based on race, such as in the Irish Traveler community (Haynes et al., 2021), or citizenship status such as people seeking asylum or who are immigrants living in Ireland who also use drugs was not included and could be a focus in future research. The sample consisted of peer advocates who have been involved in advocacy and are aware of the structures that influence their lives and therefore may be more aware of the structural processes at work in their experience as opposed to other members of the community of PWUD. The authors acknowledge that the peers spoke on behalf of their own living and lived experiences as opposed to gathering formal evidence within their peer networks.
Conclusion
People Who Use Drugs may have multiple marginalized intersectional identities making it difficult to remove stigma without exploring how social power is used to maintain it. The lived and living experience of PWUD is paramount to understanding and deconstructing social structures that reinforce stigma so they can take up their rightful place amongst society. Intersectional frameworks are of the utmost importance to inform future trainings and campaigns to reduce stigma towards PWUD.
Supplemental Material
sj-docx-1-cdx-10.1177_00914509261440952 - Supplemental material for The Other Ireland: Visualizing Intersectional Stigma Experiences of People Who Use Drugs Using Photovoice
Supplemental material, sj-docx-1-cdx-10.1177_00914509261440952 for The Other Ireland: Visualizing Intersectional Stigma Experiences of People Who Use Drugs Using Photovoice by Nicole M. Miller, Raychelle Baffo, Lucy Louise Clarke, Greg Los and Andy O’Hara in Contemporary Drug Problems
Footnotes
Acknowledgements
Thank you to the peers who dedicated their time and energy into capturing photographs and discussing them as a community. Without your intense and committed effort this project would not have been possible. Thank you to members of UISCE team, Laoise Darragh and Dr Erin Nugent for providing feedback on the manuscript.
Ethical Approval and Informed Consent Statements
This study was approved by the University of West London Research Ethics Committee (approval no. UWL/REC/PSW-01589) on 16/4/2024.
Consent to Participate
All participants provided written informed consent prior to participating. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Consent for Publication
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Union for Improved Services and Education; Merchants Quay Ireland; and the Health Service Executive National Drug Treatment Centre Ireland.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from Union for Improved Services and Education, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Union for Improved Services and Education.
Supplemental Material
Supplemental material for this article is available online.