
Abstract
The COVID-19 pandemic has disrupted life and all forms of education. However, the impact on medical education is unique since the need for continuity of training medical students is urgent and traditionally calls for hands-on training and a physical presence. This is further compounded by the unavailability of teachers who are also serving as frontline health-care providers in the pandemic. This article discusses the role and types of information communication technology (ICT) tools in filling the gaps and ensuring educational continuity in medical education, collaboration, and learning, across the world in the current scenario. A variety of online collaboration tools and digital interventions are discussed. A comparison between the various ICT tools being used by medical educators is also presented. The potential and corresponding challenges of revamping the medical education system and incorporating ICT tools in the long run have also been discussed. Our work can serve as the basis of further studies on creating digital educational models in medical education.
Keywords
Impact of COVID-19 on Medical Education
The COVID-19 pandemic has deeply impacted all spheres of education, especially with social distancing norms in place (Dhawan, 2020). Medical education, however, is uniquely affected as the need for training future health-care providers has assumed paramount importance, in the light of the global emergency (Rose, 2020). This impact is compounded by the unavailability of teachers (Marasco et al., 2020) in these unique circumstances. Since medical educators play the dual role of health-care providers, who are being called upon to discharge their duties in the service of the community, leading to a disruption in medical training.
Prepandemic medical education, for the first 12 to 18 months in the preclerkship curriculum, required students to physically convene in small groups for problem-solving collaborations. The final 18 months presented an individualized trajectory in advanced clinical rotations in the clerkship environment. The physical presence of students in inpatient and outpatient environments is a critical component in medical education and the clerkship curriculum, which is greatly impacted by the limitations in in-person gatherings presented by the COVID-19 pandemic.
Social distancing norms, requiring limiting in-person gathering, have led to a cancellation in in-person teaching, conferences, and simulation laboratories. In addition, movement between sites even within the same institution poses the risk to patients, residents, and other health-care providers alike. Patients have been advised to postpone nonessential hospital visits and surgeries. Directives to avoid nonessential personnel at sites and minimization of essential personnel during surgeries have led to a reduced case volume for residents (Chick et al., 2020). The reduced patient volume has reduced the opportunity for postgraduate medical students to perform inpatient medical procedures and gain expertise in a broad spectrum of cases (Edigin et al., 2020). Consequently, clinical rotations for surgical residents have seen a significant decline, deferral, or even cancellation. The impact is also manifested in the form of cancellation of clinical clerkships and collaborative activities of many medical students (Ferrel & Ryan, 2020).
The disruption in medical education is dramatic and without a clear endpoint, in a time where training medical students is of paramount importance in the light of a global emergency. While first-hand training in medical education is essential, information technology tools including prerecorded and live streamed lectures, simulation tools, online collaboration, and discussion platforms are helping fill in numerous other gaps in medical training during the COVID-19 pandemic and ensure educational continuity for the next generation of health-care professionals.
Interventions
Kachra and Brown (2020) aptly remarked that the COVID-19 pandemic has moved medical students out of the clinical environment, redistributed residents across the health-care system and shifted medical education online. In response to COVID-19, medical education faculty have rapidly transitioned the entire preclerkship curriculum online (Chick et al., 2020; Rose, 2020), arranging for smaller groups to convene in virtual team settings.
Medical educators are using a wide range of information and communication technology (ICT) tools to ensure the continuity of medical education amid the pandemic. It may be noted that many of the teachers and students are also involved in patient care. Nevertheless, a quick literature survey reveals that medical educators are using ICT for teaching more effectively than professors of other disciplines (Table 1). Most medical educators are disseminating study materials through university websites and online collaboration tools (Aghakhani & Shalbafan, 2020; Almarzooq et al., 2020; Ashokka et al., 2020; Czepczyński & Kunikowska, 2020; Rasmussen et al., 2020).
ICT Tools and Pedagogical Approach Being Used in Different Medical Schools.
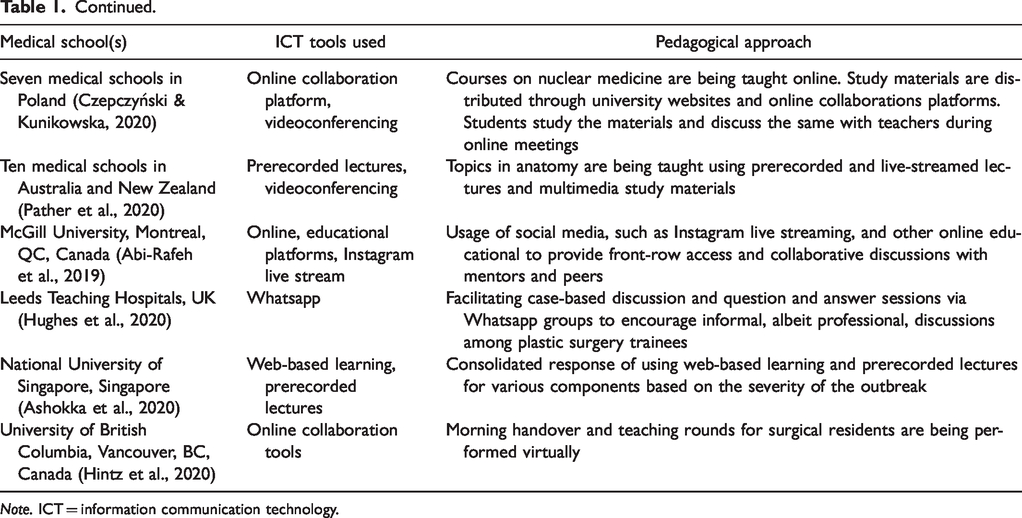
Note. ICT = information communication technology.
Online collaboration tools and social media are the popular choice among teachers and students over university websites, being convenient and more interactive than university websites and allowing for collaborative discussions on topics in medicine and surgery. Facebook groups are being used for hosting such discussions (Chick et al., 2020). Whatsapp is also a popular medium of facilitation of case-based discussion (Hughes et al., 2020). Social media-based live streaming services such as Instagram live (Abi-Rafeh et al., 2019) are also providing avenues for live training for surgery trainees and discussion with mentors and peers. The usage of teleconferencing and audience response methods is being encouraged to promote student participation during the lesson (Alvin et al., 2020). Video conferencing and collaboration tools are allowing surgical handover rounds and educational sessions to be accessible to the general surgeon community at large, providing a collaborative space for reviewing pandemic-related literature and updates (Hintz et al., 2020). Social media platforms such as LinkedIn and Twitter are enabling physicians to continue professional advancement on a personal level as well as continuing to engage with and educate peers, patients, and the community at large (Ricciardi et al., 2020).
Attending lectures delivered by professors is an important part of education in any discipline. Some medical educators are now sharing their prerecorded lectures with students, while most others prefer live streaming their lectures. Students can ask questions during live-streamed lectures via a chat response or through the video conferencing setup and the sessions may be recorded. It requires substantial time and effort to develop multimedia resources and simulation tools appropriate for teaching a course (Jain et al., 2018), and not many such tools are in use currently.
Garcia et al. (2020) recommend that medical students be encouraged to attend online conferences both within and outside their university and provided with online mentorship on a one-on-one or small group basis. Porpiglia et al. (2020) suggested that online symposiums can be conducted to foster medical education and research. Such symposiums may include talks, posters, discussions, and even industry interactions.
Clinical skill lessons are also being delivered online in some cases, although it has been observed that clinical courses typically require more time to be moved to an online platform (Aghakhani & Shalbafan, 2020). Some online resources are available for teaching surgery as well (Abi-Rafeh & Azzi, 2020). Viewing high-quality surgical videos and self and peer review of videos is being encouraged to compensate for the lack of time in the operating room (Chick et al., 2020).
Examinations are also transitioning into a virtual format. Preparations for the future academic sessions, including the selection of potential candidates, are also being made safely and virtually via video conferencing solutions (Cleland, Chu et al., 2020; Cleland, McKimm, et al., 2020).
Teachers are typically trying to keep their pedagogical approach simple, while also innovating and transitioning their teaching techniques from those suited for face-to-face instruction to those in virtual formats (Seymour-Walsh et al., 2020). The focus of medical educators remains on innovating in a new environment with novel technologies and adapting to flexible learning plans and outcomes (Hall et al., 2020). There is considerable emphasis on cultivating resilience in the learning environment (Wald, 2020). Most teachers and students are finding online education acceptable under the current circumstances (Chick et al., 2020; Czepczyński & Kunikowska, 2020).
An Analysis of ICT Tools
A wide variety of ICT tools are available currently, many of which are playing a pivotal role in ensuring the educational continuity for medical students during the COVID-19 pandemic. The major categories of tools include videoconferencing (Hintz et al., 2020) and teleconferencing solutions (Alvin et al., 2020), prerecorded videos (Chick et al., 2020), social media (Chick et al., 2020; Hughes et al., 2020; Ricciardi et al., 2020), live streaming applications (Abi-Rafeh et al., 2019), and web-based learning tools (Table 2).
A Comparison of ICT Tools Used for Medical Education.
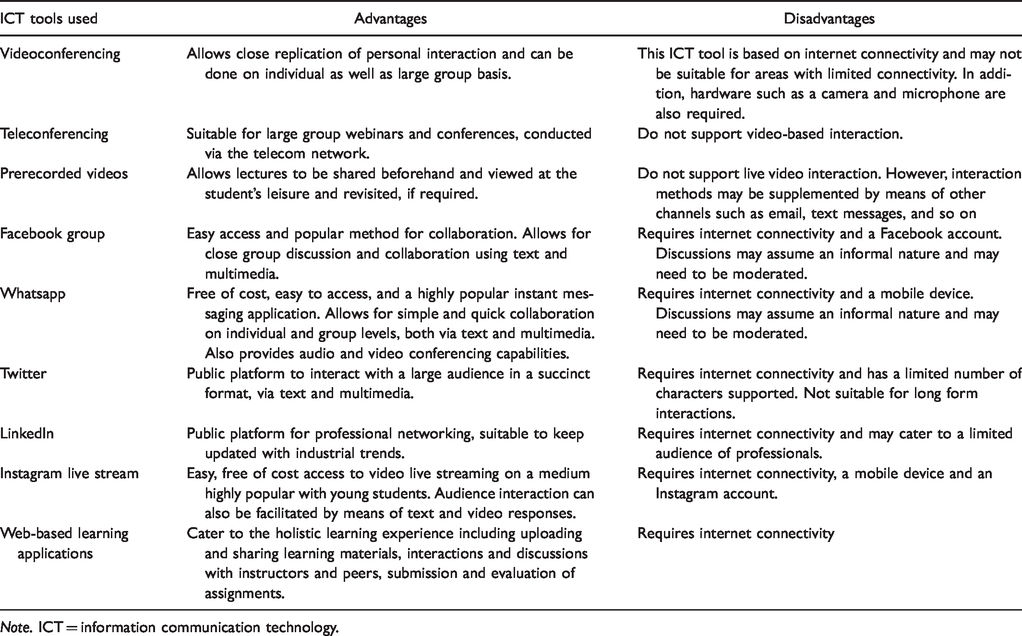
Note. ICT = information communication technology.
Videoconferencing tools allow for a high degree of real-time collaboration between the educators, students, and peers. These tools have assumed immense popularity in the light of the pandemic, given their ability to replicate in-person interaction in close proximity. A variety of internet-based videoconferencing tools are available currently, supporting handheld devices such as mobile phones, tablets, and also laptops and desktops. These solutions are also rapidly scaling up to support the needs of large groups in video calls as well as to facilitate virtual classroom lectures, conferences, and so on. Teleconferencing tools also provide similar solutions via the telecom network and are useful in regions where internet connectivity may be erratic or scarce.
Prerecorded videos and video sharing platforms are also proving to be useful for sharing and disseminating lectures. This format requires multimedia tools to record and edit video content and most commonly, a web-based sharing platform, where the videos can be uploaded, shared, and accessed at the students’ convenience. Prerecorded videos have their appeal in allowing the educational materials to be accessed at leisure and even repeatedly, if required. Such videos also form the basis of publicly accessible lectures to promote equitable access to high-quality learning materials.
Social media is a ubiquitous and popular choice of ICT tool for collaboration and learning, especially due to its appeal with the students, ease of access, and wide utilities. Facebook groups allow easy, closed group collaboration on lecture materials. Such groups provide an effective medium of conducting case-based discussions for a limited group of individuals who can participate in the discussion via the web or mobile-based platforms. Whatsapp, the popular instant messaging application, is facilitating sharing of instant messages and multimedia to individual users and large groups, free of charge via the internet. Such messaging applications tap into the convenience, ease of use for the students and educators, and allow for both formal and informal discussions.
Twitter is a public platform which is being used to connect with a larger audience of medical industry leaders, peers, patients, and educating the community at large. The microblogging nature of the platform allows medical professionals to use the short text and multimedia aid format to communicate succinctly and reach a wide audience. LinkedIn, a similar public platform, provides the tools for professional networking and continuing professional advancement through the web and mobile-based platforms. Instagram, another popular mobile-based social media application which relies greatly on sharing photographs and videos, is also a popular choice among students and lecturers.
Social media applications such as Instagram and Facebook also have video live streaming capabilities allowing ready and safe access to live demonstrations in the clinical environment. Such live stream sessions also allow for real-time interaction with the students, by means of text-based or verbal responses. These can be easily accessed via mobile and web-based platforms.
Web-based learning applications have been in use for the past several years and have contributed immensely in providing equitable and ready access to high-quality materials, earlier only available to a select group worldwide. Such platforms support a holistic learning experience, including uploading and interaction with text and multimedia content, interaction and discussion with instructors and peers, and submission and evaluation of assignments. All of these facilities are made available through websites, and in many cases, through mobile applications as well.
Discussion
Medical schools are trying to adapt to the pandemic (Cleland, Chu et al., 2020; Cleland, McKimm, et al., 2020) and using ICT for teaching, assessing, and managing students (Jervis & Brown, 2020; Watson et al., 2020). While preclinical courses may be taught through videoconferencing, clinical courses may benefit from simulation tools and problem-based learning tutorials (Sahi et al., 2020).
Flipped classroom methods are a well-studied teaching pedagogy, providing learners with prerecorded didactic video lectures to be watched at the learner’s leisure before an in-person conference. The purpose of the in-person congregation shifts to application and case-based discussion on the basis of the lecture. These methods are found to be more effective than traditional teaching methods to improve student learning performance (Hew & Lo, 2018). Given the prior experimentation and experience of medical educators, flipped classroom methods and technologies provided a rapid transition in the light of the prevailing restrictions due to COVID-19. Although some medical schools had been experimenting with flipped classrooms to provide individualized and blended learning models in recent years, face-to-face interaction for peer group discussions, laboratory and technology sessions, continues to play a crucial role in medical education (Michels et al., 2020). Medical educators agree that there can be no substitute for hands-on learning through dissections, equipment training, direct patient care, and operative experience (Chick et al., 2020; Evans et al., 2020). However, the introduction of flipped classrooms during the COVID-19 pandemic will provide the platform for incorporation of flipped classrooms and their numerous benefits in the medical education system of the future.
Video-based coaching for surgical education, in an era of competency-based surgical education, was already being evaluated for its efficacy before the COVID-19 pandemic and has been observed to increase the technical performance of surgical residents (Augestad et al., 2020), including in suturing tasks (Alameddine et al., 2018). Residents have also favorably viewed video-based surgical instruction and preferred intraoperative recordings (McKinley et al., 2019). E-learning has also been found to be effective in teaching cases through virtual patients (Jayakumar et al., 2015). Furthermore, surgical simulations, preferably using virtual reality, can be used as viable educational tools (Kogan et al., 2020). Future studies must be undertaken in order to regularize the delivery of lessons through electronic mediums.
Delivery of case discussions in an informal, albeit professional, manner through the free, encrypted cross platform application Whatsapp (Hughes et al., 2020) and social media-based live streaming services such as Instagram live (Abi-Rafeh et al., 2019) encourage active involvement by students at all levels, while bridging the gap in clinical exposure due to the pandemic and providing opportunities for mentorship and collaboration. The efficacy of Whatsapp as an educational tool has been evaluated (Coleman & O’Connor, 2019) and if used appropriately with the purpose of disseminating medical education and discussion can serve as the basis of an instant messaging application-based learning model for medical education.
Hughes et al. (2020) rightly add caveats to ensure privacy, despite Whatsapp’s end-to-end encryption, and refrain from disclosing patient details and identifiable data. Professional usage of closed social media groups for surgical practice and education calls for informed patient consent, the responsibility of which lies with the physician (Bittner et al., 2019).
Online education is allowing medical students to attend lectures and access study materials from anywhere and at any time using a computer or a smartphone (Chick et al., 2020). This is particularly helpful for international students many of whom have returned to their native countries at the outbreak of the pandemic (Sandhu & de Wolf, 2020). Similar to other educational domains, usage of ICT tools has also brought about a democratization of educational content, giving students access to high-quality didactic tutorials by the pioneers in their field, regardless of geographical and monetary barriers (Abi-Rafeh & Azzi, 2020).
Shaping the Educational Fabric of the Future
The COVID-19 pandemic presents us with both the gaps in the current system and the opportunity to rethink educational paradigms, especially in the context of medical education and the incorporation of ICT tools in the longer run. ICT tools have acceptably provided continuity of education in the ongoing crisis and have even exhibited their benefits in multiple spheres. Some online teaching–learning processes introduced in medical education due to the COVID-19 pandemic have been appreciated by teachers and students, and will perhaps continue to be used in the future (Ahmed et al., 2020).
Medical education systems have largely focused on content delivery over problem-solving and the call for reforms and the introduction of digital infrastructure has long been made, but the changes in the light of the pandemic can catalyze the long pending changes (Chen & Mullen, 2020). Online lecture videos have been identified to be an effective and preferred content delivery route in learning, leaving in person interactions for active learning, problem-solving, and providing feedback.
The current assumption of the availability of a device with the learner exposes equity gaps (Fuller et al., 2020) which must be addressed in order to provide educational access to all. This paradigm shift in the delivery and assessment of medical education also calls for the flexibility and innovation in the policy response for the present and the future (Fuller et al., 2020). The pedagogical approaches must acknowledge the capabilities and limitations of modern online educational systems and create systems which accommodate learners across socioeconomic backgrounds and geographies (Seymour-Walsh et al., 2020).
It is also worth noting that transition from workplaces and medical schools to a home-based learning environment via ICT tools may result in isolation and difficulties in establishing boundaries between home and work environments, affecting medical educators, students, and staff. In reimagining medical education for the future, arrangements must be made to take into account the mental well-being of health-care professionals who are exposed first-hand to the current ongoing crisis.
Conclusion
The COVID-19 pandemic has undoubtedly impacted all aspects of education. However, in case of medical education, the impact is unique since medical educators play dual roles of health-care providers who are engaged in combating the pandemic on the frontlines. Continuity of medical education has gained paramount importance in the light of the global emergency and has been affected by the social distancing norms in place.
ICT tools are proving to be acceptable and even indispensable in filling the gaps in medical education currently. A wide variety of ICT tools such as university websites, online collaboration and video conferencing tools, prerecorded and live-streamed video lectures, social media platforms are proving to be effective means to ensure educational effectiveness and continuity for the training of the future generation of medical students.
The COVID-19 pandemic also presents the opportunity to rethink educational paradigms (Wotto, 2020), especially in the context of medical education and the incorporation of ICT tools in the longer run. While the usage of ICT tools was being experimentally being evaluated by medical schools before the pandemic and was found to be promising, the current circumstances have accelerated their adoption and have provided real-time value and adoption. Medical educators and professionals are reevaluating the usage of technological tools to provide effective and safe ways to deliver instruction during the foreseeable future during the pandemic and beyond. The digital infrastructure put in place for teaching during this time and the learning from this transition can provide the much-needed foundation and impetus of creating a medical education system of the future, powered by ICT tools.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.