
Abstract
Arboviruses, such as yellow fever and dengue viruses, pose a growing public health threat in Sub-Saharan Africa, particularly at human-wildlife interfaces. Mole National Park (MNP), with its rich biodiversity and ecotourism, represents a high-risk area and has been the epicentre of recent outbreaks in Ghana. The objective of this study was to assess community knowledge, attitudes and practices (KAP) regarding arboviral transmission and prevention in this high-risk interface. In December 2023, we conducted a cross-sectional KAP survey among 300 adults in MNP (n = 120) and nearby communities, Murugu (n = 94) and Mognori (n = 86) using structured questionnaires. Data were analysed using descriptive statistics and chi-square tests, and a multivariable logistic regression model (α = .05). Awareness of yellow fever was high (92.0%), but none mentioned dengue or Zika; awareness varied significantly by location (MNP 96.7%, Murugu 96.8%, Mognori 80.2%; P < .001). Only 44.0% correctly associated mosquito bites with yellow fever transmission. Fever was cited as a common symptom by 17.0%, but misconceptions such as “yellow vomit” (5.0%) and “yellow urine” (10.3%) persisted. While nearly all (95.7%) reported using Insecticide-treated nets, adoption of other preventive measures like repellents (5.0%) and environmental management (1.0%) was very low. Perceptions of arbovirus presence also differed significantly across communities (MNP 48.4%, Murugu 38.7%, Mognori 12.9%; P < .001). Despite these knowledge gaps, all respondents indicated they would seek medical care if infected. These findings suggest that, despite high awareness of yellow fever, knowledge gaps persist regarding its symptoms, transmission, and preventive measures. Addressing these requires sustained health education initiatives on arboviral disease transmission, improved access to repellents and water, sanitation, and hygiene tools, and a One Health approach that integrates human, animal, and environmental health.
Keywords
Introduction
Arthropod-borne viruses (arboviruses) are a diverse group of viruses transmitted to humans and other vertebrates through the bites of blood-feeding arthropods such as mosquitoes. These viruses are responsible for diseases such as yellow fever, dengue fever, and Zika, particularly prevalent in tropical regions.1 -3 In recent decades, arboviruses have gained prominence as a global public health concern due to their ability to spread to new geographic areas, driven by factors such as urbanisation and climate variability, 4 as well as the emergence of novel variants, and complications associated with their infections leading to severe disease outcomes.5,6
In recent years, West Africa has experienced a significant rise in arboviral activity, marked by outbreaks of dengue in Burkina Faso,7,8 Côte d’Ivoire,9,10 and Senegal, 11 as well as yellow fever in Côte d’Ivoire 12 and Nigeria. 13 Ghana has not been spared, having reported cases of dengue14 -16 and experiencing localised yellow fever outbreaks, including one from October 2021 to February 2022 that resulted in 35 fatalities. 17 Furthermore, although clinical outbreaks of the Zika virus have been less visible, serological surveillance indicates significant circulation of the virus in Ghana, with seroprevalence rates as high as 20.6% reported in some populations, 18 while serological surveillance provides evidence of past exposure; integrating these findings with behavioural data is critical for understanding the human drivers of transmission. 19 These events highlight an urgent need to understand and address the public health risks posed by arboviruses in the country, particularly in areas where human populations are in close contact with wildlife.
Mole National Park, Ghana’s largest wildlife reserve, is home to diverse non-human primates (NHPs), such as baboons and patas monkeys, which can serve as reservoirs for arboviruses like the yellow fever virus.20,21 Communities living near the park have a heightened risk of arboviral infection due to their proximity to wildlife and their reliance on outdoor activities, such as farming and hunting for sustenance, which increases exposure to mosquito vectors. Compounding this risk are potential gaps in awareness, preventive practices, and access to healthcare resources in these populations.22,23 Ghana has experienced multiple large yellow fever outbreaks in several regions since 1910. 24 However, in recent years, the districts encompassing Mole National Park have emerged as a hotspot, marking the area as a high-risk zone for yellow fever transmission. 25
Assessing the knowledge, attitudes, and practices (KAP) of communities in such high-risk areas as Mole National Park is crucial for understanding how local populations perceive and respond to the threat of arboviral diseases. Such insights will help design effective public health interventions that can reduce the risk of arboviral disease outbreaks in the affected regions. Hence, this study sought to evaluate the KAP of inhabitants of Mole National Park and surrounding communities concerning arbovirus infection awareness and prevention, providing evidence to inform targeted strategies for mitigating arbovirus infection and transmission in this population.
Materials and Methods
Study Area and Design
A community-based cross-sectional survey design was adopted for this study. The study design and reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The study was conducted in Mole National Park and two other communities, Murugu and Mognori, situated at the fringe of the park (Figure 1). Mole National Park, the largest park in Ghana, spans approximately 4840 km2 within the Savannah Region. Classified as a Guinea savanna, the park receives 950 to 1100 mm of annual rainfall during a single wet season. It is home to over 400 animal species, including elephants, chimpanzees, monkeys, birds, and other wildlife. 26 The park is rural and isolated from major urban areas, and employees live in quarters inside the park close to wildlife.

Mole National Park, showing the surrounding communities and study sites.
The park shares a border with 33 farming communities spread across 5 districts, all within a 5 km radius of the park. Murugu and Mognori are 2 of the farming communities that existed before the establishment of the Mole National Park. These 2 communities were purposively selected because they are situated at the primary gateways to the park, resulting in the highest frequency of human-wildlife interaction and ecotourism activities compared to other peripheral communities. The residents are mainly peasant farmers, with some engaged in fishing due to proximity to the Mole River. Traditional mud houses with thatched roofs dominate the housing structure in the communities. Both communities rely on a Community-Based Health Planning and Services (CHPS) compound for healthcare. The 2 communities were chosen for their proximity to potential mosquito breeding sites and their interactions with wildlife and park ecosystems, potentially increasing arbovirus transmission risks.
Study Population, Participants, and Inclusion Criteria
The study population consisted of adult residents (aged 18 years and above) of both genders in the selected communities. Participants were included if they provided written consent or thumb-printed consent and demonstrated a sufficient understanding of the study’s objectives and procedures following a verbal explanation in their dialect. The inability to read or write was not an exclusion criterion; interpreters facilitated the consent process for participants with no formal education to ensure their perspectives were accurately captured. Only individuals who had lived in the study communities for more than 6 months were included, ensuring they had had enough exposure to the environmental and health-related factors relevant to the study. Exclusion criteria included temporary visitors and individuals with residency of less than 6 months.
Sample Size and Sampling Technique
The sample size was calculated based on the requirements for the serological component of the larger arbovirus-risk assessment project. Using the formula for estimating prevalence in cross-sectional studies 28 with a 95% confidence level, a 5% margin of error, and a reported Zika virus seroprevalence of 20.6%, 18 a minimum sample size of 252 was calculated. While this calculation was driven by serological parameters, the final sample size of 300 recruited participants provides sufficient statistical power for the descriptive analysis of knowledge, attitude, and practices.
Data Collection Tool and Procedures
From 27th to 31st December 2023, we administered a structured questionnaire face-to-face at all 3 study sites. The survey instrument (Supplemental File 2) was adapted from validated tools used in previous studies on yellow fever and dengue fever.29 -32
The questionnaire consisted of 4 sections. Section A collected socio-demographic data, including age, gender, education, and occupation. Section B assessed general awareness of arboviral diseases; participants who indicated awareness were asked to specify the disease(s) they knew. Given the endemicity of the region, Yellow Fever was the predominant response and the primary focus of subsequent specific knowledge questions (symptoms and transmission). Section C measured attitudes towards disease risk and severity using a 3-point Likert scale (eg, “Not concerned” to “Very concerned”). Section D assessed preventive practices, specifically the use of vector control measures such as bed nets and protective clothing.
To ensure content validity and cultural relevance, the questionnaire was reviewed by public health experts and pre-tested on 10 individuals in a different community not included in the final study. Feedback from this pre-test was used to refine the phrasing of the questions. Interviews were conducted in English or the local dialect (Twi). To ensure linguistic accuracy without formal written translation, the research assistants underwent a consensus-based training session to agree upon uniform local terminologies for key concepts such as “virus,” “transmission,” and “vector.” Data were collected electronically using the Epicollect5 software 33 on mobile devices.
Ethical Consideration
This work was part of a larger arbovirus-risk assessment in and around Mole National Park. For the KAP survey component, we obtained ethical approval (CHRPE/AP/429/23) from the Committee on Human Research, Publication, and Ethics (CHRPE) at Kwame Nkrumah University of Science and Technology. We also received official permission from the Regional Health Directorate of the Savannah Region to conduct community interviews. At the community level, permission was sought and received from the management of Mole National Park, as well as the chiefs and elders in Murugu and Mognori. Following this, the study’s objectives were explained to potential participants. Each individual provided written informed consent before a questionnaire was administered.
For the broader project components, specifically the entomological survey and serological screening, additional permits were obtained from the Wildlife Division of the Forestry Commission and other relevant stakeholders.
Statistical Analysis
The study used the Statistical Package for Social Sciences (SPSS version 25) for all analyses. Descriptive statistics such as percentages and frequencies were used to explore the demographic characteristics and KAP of the respondents. Percentages reported are column percentages to allow for comparison between the 3 study sites. The chi-square test was further used to assess associations across the communities.
Further analysis was conducted using multivariable binary logistic regression to determine the predictors (age, gender, education, occupation, and community) of correct transmission knowledge. The results are presented as Adjusted Odds Ratios (AOR) with 95% Confidence Intervals (CI). A P-value of .05 was considered statistically significant. Data was presented in tables for easy interpretation and understanding.
Results
Socio-Demographic Characteristics of Respondents
A total of 300 respondents participated in the study, comprising 190 males (63.3%) and 110 females (36.7%). The largest age demographic was the 21 to 30 years group (32.7%), while the elderly (>60 years) represented the smallest proportion (3.6%). Educational attainment varied significantly by community; respondents in Murugu had the highest proportion of individuals with no formal education (41.5%), whereas Mole had the highest concentration of tertiary-level education (25.0%; Table 1).
Socio-Demographic Characteristics of Respondents From Study Communities.
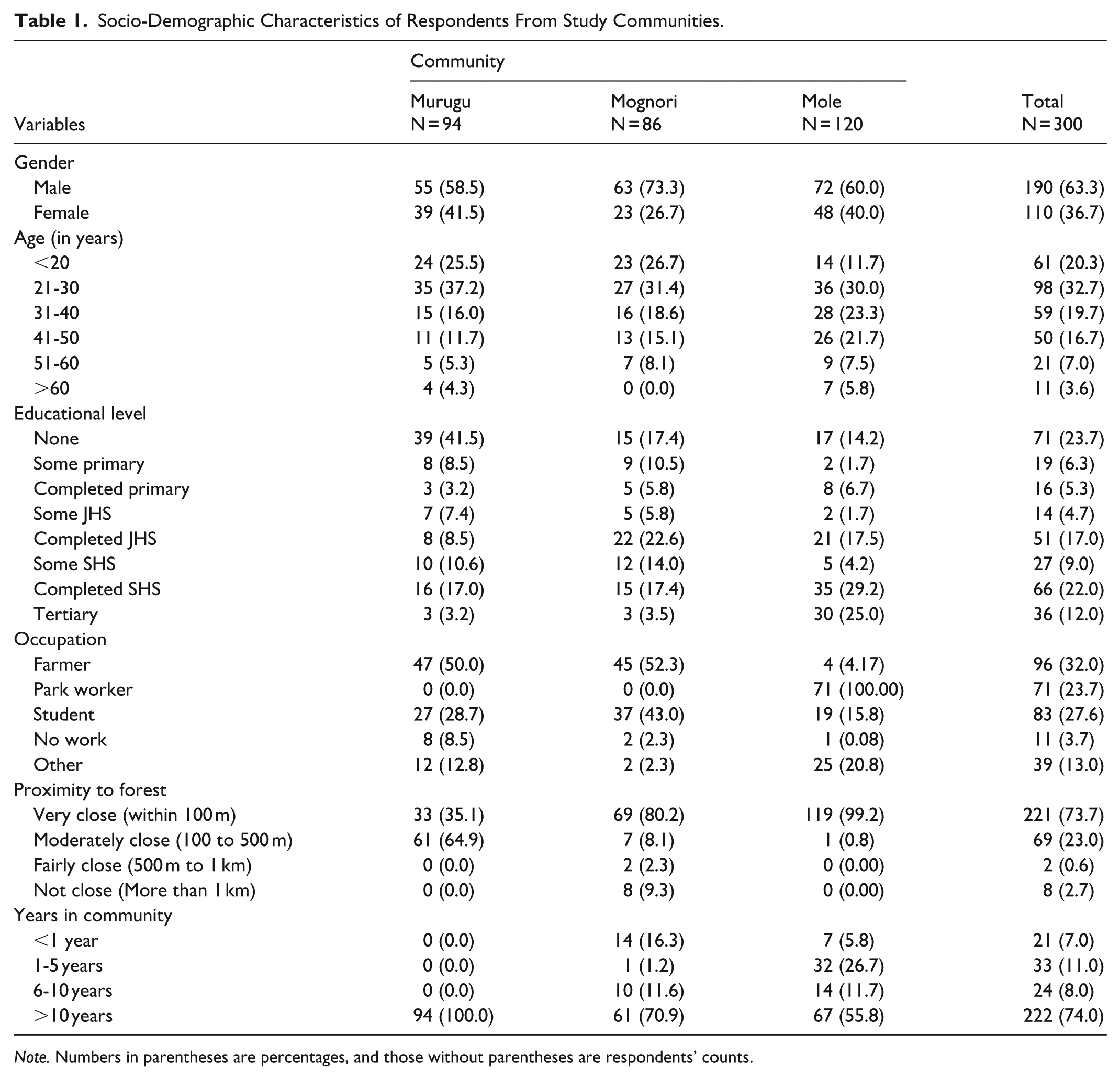
Note. Numbers in parentheses are percentages, and those without parentheses are respondents’ counts.
Occupations reflected local livelihoods and community functions. Farming was the most common occupation overall (32.0%), predominantly in Murugu and Mognori, while all respondents identified as park workers resided in Mole (100.0%). The majority of participants (73.7%) lived within 100 m of the park boundary, and 74.0% had resided in their respective communities for over 10 years, indicating a stable population with long-term exposure to the local environment.
Knowledge of Respondents About Arboviral Diseases
The study assessed respondents’ knowledge of arboviral diseases. Approximately 92.0% of respondents indicated awareness of some arboviral diseases, with awareness largely limited to yellow fever (276, 92.0%), and no report of awareness of other arboviral diseases such as Dengue and Zika.
Among the respondents who knew about yellow fever, the majority reported health clinics (79.3%; χ2 = 11.957, P = .002) as their source of information, followed by the Media (58.7%; χ2 = 5.16, P = .076), and community leaders (9.4%; χ2 4.67, P = .097) were reported as the least common source they acquired information about arboviral diseases.
The majority of the respondents (45.3%) knew mosquito bites as the mode of transmission, whilst slightly less than half (43.1%) were not sure how arboviral diseases were transmitted. However, other routes of arboviral transmission mentioned were direct contact with an infected person (8.7%), and a few (2.9%) mentioned both mosquito bites and direct contact with an infected person. These responses varied significantly across the communities (χ2 = 17.02, P = .009).
The most common symptoms the respondents associated with yellow fever were yellow eye (jaundice, 23.6%), fever (18.5%), and headache (14.1%); the least mentioned symptoms were body weakness/ fatigue (6.2%) and body pains and dizziness, accounting for 1.4% each, respectively. The respondents also mentioned symptoms that are not often used as clinical signs of yellow fever, such as yellow urine (11.2%), yellow vomit (5.4%), and cold (4.0%).
The availability of the yellow fever vaccine was well known to the respondents (83.3%); however, the majority of the respondents (67.8%) also claimed that arboviral diseases can be treated (Table 2).
Respondents’ Knowledge of Arboviral Disease.

Note. Italicised numbers are percentages; χ2 is the Chi-square coefficient.
Indicates a significant difference at P < .05.
The Attitude of Respondents Towards Arboviral Diseases
The data reveal varying attitudes towards the presence of arboviral diseases across the 3 communities. A greater number of respondents (94.0%) perceived arboviral diseases as very serious, and this perception varied significantly across the communities (χ2 = 15.88, P = .003). About 20.7% believed arboviral diseases were present in their communities. Across the communities, 90.7% of respondents were very concerned about the risk of arboviral diseases. Moreover, all the respondents (100.0%) expressed a willingness to seek medical treatment if they suspected they had contracted an arboviral disease, reflecting a common proactive attitude towards healthcare (Table 3).
Respondents’ Attitude Towards Arboviral Diseases.

Note. Italicised numbers are percentages; χ2 is the Chi-square coefficient.
Indicates a significant difference at P < .05.
Practices of Respondents Related to Arbovirus Prevention
A total of 99.3% of respondents across the 3 communities demonstrated a strong willingness to engage in arbovirus prevention. Specifically, 98.9% of respondents from Murugu, 100.0% of respondents from Mognori, and 99.2% from Mole indicated their willingness to participate in preventive measures (Table 4). There was no significant difference in willingness across the communities (χ2 = 0.85, P = .653), suggesting a uniform attitude towards prevention (Table 4).
Practices Related to Arbovirus Prevention.

Note. Italicised numbers are percentages; χ2 is the Chi-square coefficient.
Indicates a significant difference at P < .05.
All respondents (100.0%) reported using some form of protection. Insecticide-treated bed net was the most frequently reported, followed by wearing long trousers and long-sleeved clothing (33.7%), and insecticide spray use (31.7%). The least reported practices were smoke from firewood (0.3%), environmental management (1.0%), mosquito repellent (5.0%), and the use of mosquito coil (7.0%; Table 4).
Predictors of Correct Transmission Knowledge
A multivariable binary logistic regression was performed to ascertain the effects of community, age, gender, education, and occupation on the likelihood of participants correctly identifying mosquito bites as the transmission route (Table 5). The model explained significant variance in knowledge. Residence was a significant predictor; residents of Mognori had significantly lower odds of correct knowledge compared to residents of Mole (AOR = 0.21; 95% CI: 0.07-0.60; P = .004). Age was also a strong predictor, with older age groups consistently demonstrating lower odds of correct knowledge compared to the youngest cohort (<20 years) (P < .05 for all groups). Interestingly, after adjusting for other factors, neither educational level (P > .05), gender (P = .832), nor occupation (P > .05) were statistically significant predictors of transmission knowledge.
Multivariable Logistic Regression Analysis of Factors Associated With Correct Knowledge of Arbovirus Transmission.

Note. AOR = adjusted odds ratio; CI = confidence interval; Ref = reference category.
Significant at P < .05.
Discussion
This study examined community awareness, knowledge, attitudes, and prevention practices related to arboviral diseases among communities in and around Mole National Park. The findings reveal notable strengths and gaps in community knowledge and behaviour, offering insights for improving public health interventions and reducing the risk of arboviral transmission in Ghana.
Awareness of yellow fever as an arboviral disease was generally high across the 3 communities. Health clinics and media outlets served as primary sources of information for raising awareness about yellow fever. However, their influence differed across the communities, with residents of Mole citing the media more frequently, whereas respondents from Murugu relied heavily on health workers for information. In line with our findings, previous research has also reported widespread knowledge about yellow fever in Ghana, largely attributed to targeted vaccination campaigns. 34 These campaigns are often accompanied by extensive education and sensitisation efforts led by health workers. While clinics remain an important source of information, other studies have shown that some populations also receive health information through mass media, such as television. 30 This reinforces the role of both interpersonal and digital communication in shaping public awareness of arboviral diseases in some parts of Ghana. In addition to health workers and media sources, the involvement of community leaders was mentioned as a channel for disseminating health information. Strengthening the engagement of these trusted local figures may improve public receptivity and participation in health interventions. Similar strategies have proven effective in other African contexts, including Kenya and Burkina Faso, where partnerships with religious and traditional leaders significantly enhanced community adherence to prevention measures. 7
While general awareness of the disease name was high, specific knowledge regarding transmission dynamics and clinical presentation was less comprehensive. About 45.3% of the respondents stated that mosquito bites are capable of transmitting arboviruses, while 43.1% had no idea how they are transmitted. This observation contradicts other studies, where very few participants knew that the mosquito is the transmission vector for yellow fever.35,36 Fever and yellow eyes, often associated with jaundice, emerged as the most frequently identified symptom, a finding consistent with prior studies conducted in rural settings, where feverish illnesses are commonly linked to mosquito-borne infections.31,32 However, misconceptions such as associating yellow vomit and yellow urine with yellow fever were frequently reported. These inaccuracies align with findings from Côte d’Ivoire and Senegal, where similar confusion around symptoms has been documented.37,38 This suggests that while general awareness may be present, depth of understanding remains shallow, requiring targeted health education that addresses not only the disease name but also its clinical presentation and transmission dynamics. Most respondents reported vaccine availability and reported that treatments exist for yellow fever. This pattern suggests confusion between vaccination and treatment, a common finding in KAP studies in the region. 30
Only 20.7% of respondents believed yellow fever was present in their communities, while 59.3% were unsure. This high level of uncertainty implies low perceived local risk and reflects likely uneven exposure to recent outbreaks and uneven access to information. Studies from Ghana show awareness rises after outbreak response campaigns, while communities not reached by those campaigns remain less certain. 30 Despite the differences in perceived disease presence, the majority of respondents across all 3 communities viewed yellow fever as a serious illness, with significant proportions from Mognori, Murugu, and Mole rating it as very serious. However, concerns about contracting the disease did not significantly vary between communities, suggesting a shared sense of vulnerability. Notably, all respondents reported they would seek medical care if infected, reflecting a strong health-conscious attitude consistent with the positive health-seeking behaviours observed in previous studies.30,39 This willingness to seek care may be leveraged to enhance arboviral educational activities and surveillance campaigns, particularly in communities with lower perceived risk or knowledge gaps. In contrast to our findings, studies in other parts of West Africa have reported lower willingness to seek care or limited understanding of yellow fever severity, often due to poor access to health services or low health literacy.38,40 This suggests that while attitudes in the current study were encouraging, such outcomes cannot be assumed across all rural populations.
A strong willingness among all 3 communities to prevent yellow fever was observed, with over 90.0% of participants reporting protective behaviours. The consistent attitude suggests a common concern about mosquito-borne infections, which reflects previously reported findings that showed similar engagement during yellow fever interventions in northern Ghana. 30 While the overall reported uptake of preventive measures was high, the specific methods adopted varied in efficacy against day-biting vectors. The majority of the participants across the communities mentioned that they used insecticide-treated nets (ITNs) as a preventive measure, followed by wearing trousers and long-sleeved shirts. This reliance on ITNs aligns with previous regional studies 30 and likely reflects successful nationwide distribution campaigns. 41 However, since ITNs primarily protect against night-biting mosquitoes, relying on them alone leaves a critical gap in protection against day-active Aedes vectors, 42 as their specific biting patterns and lifecycle limit the efficacy of nocturnal barriers. In contrast, the use of environmental management, repellents, and mosquito coils was minimal, contradicting studies elsewhere that observed higher usage of these tools.30,43 These disparities likely stem from limited access to resources or inadequate knowledge about the specific vector in the study areas.
Multivariable analysis identified age and residence as the primary drivers of correct transmission knowledge. Older respondents were consistently less likely to identify mosquito bites as the transmission route compared to the youngest cohort (<20 years), suggesting that recent educational initiatives may be reaching youth more effectively than the elderly. Additionally, residents of Mognori had significantly lower odds of correct knowledge compared to Mole, highlighting a need for geographically targeted health education. Interestingly, occupation was not a significant predictor in the adjusted model, likely due to the strong collinearity with residence, as the high-knowledge park worker population resides exclusively in Mole.
Given the proximity of these communities to the wildlife interface of Mole National Park, these behavioural findings highlight the human component of transmission risk. Integrating these insights with entomological and wildlife surveillance, a One Health approach, will be essential for developing comprehensive control strategies.44,45
This study has several limitations inherent to its design. First, the cross-sectional nature of the data prevents the establishment of causal relationships between sociodemographic factors and KAP variables. Second, the reliance on self-reported data subjects the findings to information bias, specifically recall bias regarding past sources of information. Third, social desirability bias is a common challenge in KAP surveys, where participants may over-report positive preventive practices to appear compliant with public health expectations. Additionally, while we assessed preventive measures related to vector control, we did not verify yellow fever vaccination status (eg, via vaccination cards), limiting our scope regarding biomedical prevention practices. Finally, selection bias may have occurred if residents available for interviews during the day differed systematically from those absent due to farming activities. Despite these limitations, the inclusion of 3 distinct communities and the high response rate strengthens the validity of the findings.
Conclusion
This study demonstrates that while general awareness of yellow fever is high among communities surrounding Mole National Park, specific knowledge regarding transmission vectors and symptoms remains suboptimal, particularly among older populations and residents of Mognori. Although attitudes towards seeking medical care are positive, the reliance on bed nets alone leaves a gap in protection against day-biting vectors. Educational interventions should be revitalised, with a specific focus on bridging the knowledge gap between the youth and the elderly, and targeted outreach for communities with lower awareness. Finally, because these communities exist at the human-wildlife interface, future control efforts should move beyond isolated human health interventions and adopt a One Health framework, coordinating community engagement with vector control and wildlife surveillance to effectively mitigate arboviral risks.
Supplemental Material
sj-docx-2-inq-10.1177_00469580261436618 – Supplemental material for Knowledge, Attitudes, and Practices Regarding Arboviruses at a Human-Wildlife Interface: A Cross-Sectional Study in and Around Mole National Park, Ghana
Supplemental material, sj-docx-2-inq-10.1177_00469580261436618 for Knowledge, Attitudes, and Practices Regarding Arboviruses at a Human-Wildlife Interface: A Cross-Sectional Study in and Around Mole National Park, Ghana by Patrick Kwasi Obuam, Sandra Abankwa Kwarteng, Anthony Afum-Adjei Awuah, Shirley Cameron Nimo-Paintsil, Seth Offei Addo, Mba Mosore, Ernest Ampon, Sylvester Coleman, Augustina Angelina Sylverken, Meyir Yiryele Ziekah, Thomas Peprah Agyekum, Philip Kweku Baidoo, Robert Clement Abaidoo, Samuel Kweku Dadzie and Ellis Owusu-Dabo in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-1-inq-10.1177_00469580261436618 – Supplemental material for Knowledge, Attitudes, and Practices Regarding Arboviruses at a Human-Wildlife Interface: A Cross-Sectional Study in and Around Mole National Park, Ghana
Supplemental material, sj-pdf-1-inq-10.1177_00469580261436618 for Knowledge, Attitudes, and Practices Regarding Arboviruses at a Human-Wildlife Interface: A Cross-Sectional Study in and Around Mole National Park, Ghana by Patrick Kwasi Obuam, Sandra Abankwa Kwarteng, Anthony Afum-Adjei Awuah, Shirley Cameron Nimo-Paintsil, Seth Offei Addo, Mba Mosore, Ernest Ampon, Sylvester Coleman, Augustina Angelina Sylverken, Meyir Yiryele Ziekah, Thomas Peprah Agyekum, Philip Kweku Baidoo, Robert Clement Abaidoo, Samuel Kweku Dadzie and Ellis Owusu-Dabo in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-3-inq-10.1177_00469580261436618 – Supplemental material for Knowledge, Attitudes, and Practices Regarding Arboviruses at a Human-Wildlife Interface: A Cross-Sectional Study in and Around Mole National Park, Ghana
Supplemental material, sj-pdf-3-inq-10.1177_00469580261436618 for Knowledge, Attitudes, and Practices Regarding Arboviruses at a Human-Wildlife Interface: A Cross-Sectional Study in and Around Mole National Park, Ghana by Patrick Kwasi Obuam, Sandra Abankwa Kwarteng, Anthony Afum-Adjei Awuah, Shirley Cameron Nimo-Paintsil, Seth Offei Addo, Mba Mosore, Ernest Ampon, Sylvester Coleman, Augustina Angelina Sylverken, Meyir Yiryele Ziekah, Thomas Peprah Agyekum, Philip Kweku Baidoo, Robert Clement Abaidoo, Samuel Kweku Dadzie and Ellis Owusu-Dabo in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to acknowledge the management of Mole National Park, public health nurses, and the people of Murugu and Mognori communities for their exceptional support, which made the completion of this work possible.
Ethical Considerations
This study received ethical approval from the Committee on Human Research, Publication, and Ethics (CHRPE) at Kwame Nkrumah University of Science and Technology (CHRPE/AP/429/23) on June 12, 2023. Respondents provided written consent and signed a form before participating in the interviews.
Consent to Participate
Written informed consent was obtained from all participants prior to administering the questionnaires.
Author Contributions
Conceptualisation: S.A.K., M.M.; Data curation: P.K.O., E.A.; Formal Analysis: P.K.O., T.P.A., S.C.; Investigation: P.K.O., E.A., M.Y.Z.; Writing – Original Draft: P.K.O.; Writing – Review & Editing: S.A.K., A.A.A.A., A.A.S., S.C.N.P., S.O.A., T.P.A., S.C., E.A., P.K.B., R.C.A., S.K.D., E.O.D.; Supervision: S.A.K., A.A.A.A., P.K.B., E.O.D.; Funding Acquisition: S.A.K. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the KNUST Research Fund (KReF) [grant number: VC/OGR/15].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data for this study are available upon request from the corresponding author.*
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.