
Abstract
Objectives:
This study aims to assess health science students’ knowledge and attitude about COVID-19 epidemiology, management, and prevention; and the association of knowledge and attitude with various sociodemographic characteristics.
Methods:
An online survey was done among 524 undergraduate health science students using a pre-tested questionnaire across 19 health science institutions in Nepal from 30 June to 11 August 2021. All subjects were enrolled in the study after informed consent. Outcomes were Knowledge level, attitude level, and predictors of knowledge level and attitude level. Bivariate analysis was done to determine the association between variables.
Results:
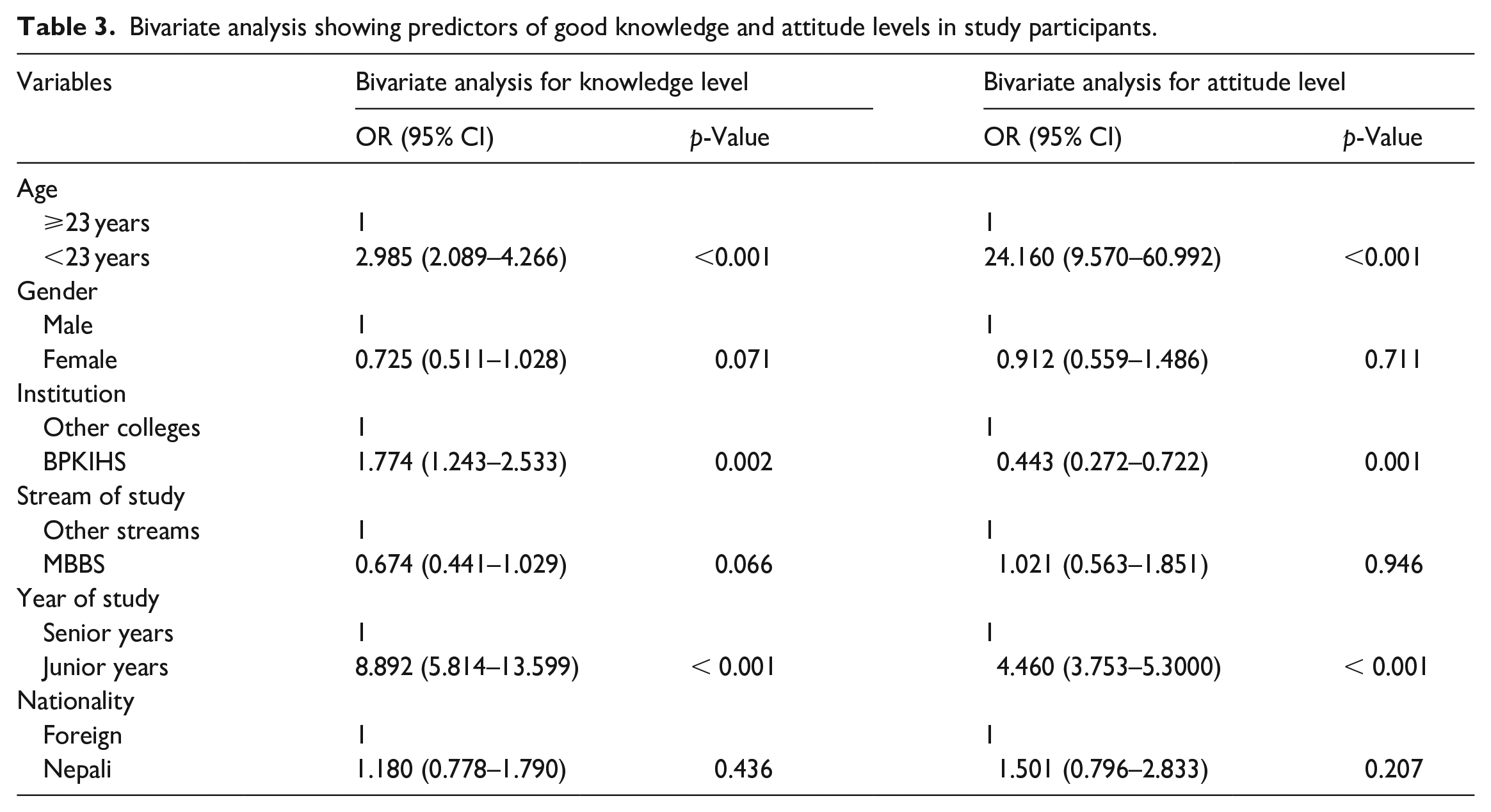
Of 524 students, 42.9% were male, and 57.1% were female. More than half (54.6%) and the majority (85.1%) participants had good knowledge and attitude, respectively. Approximately three-fifths (59.4%) of the participants were from the B. P. Koirala Institute of Health Sciences (BPKIHS). Students in BPKIHS (odds ratio = 1.774; 95% confidence interval = 1.243–2.533), junior years (odds ratio = 8.892; 95% confidence interval = 5.814–13.599), age less than 23 years (odds ratio = 2.985; 95% confidence interval = 2.089–4.266) were more likely to have good knowledge. Students under 23 years (odds ratio = 24.160; 95% confidence interval: 9.570–60.992) and those in junior years (odds ratio = 4.460; 95% confidence interval = 3.753–5.300) were likely to have a good attitude level. Students in BPKIHS (odds ratio = 0.443; 95% confidence interval = 0.272–0.722) were less likely to have a good attitude.
Conclusions:
Overall, health science students had adequate knowledge and a good attitude regarding COVID-19. However, students lacked knowledge regarding infectiousness, transmission, post-vaccination observation period, remdesivir use, convalescent plasma therapy, and awake-prone positioning. Knowledge and attitude scores were associated with age, stream, and study institution.
Introduction
Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2) is a positive-sense, single-stranded RNA virus with a high transmission rate that causes COVID-19.1–3 It was first reported by the World Health Organization (WHO) as ‘pneumonia of unknown cause’ in the capital of Hubei Province in Wuhan and was declared a pandemic on 11 March 2020. 4 Nepal reported the first case of COVID-19 on 23 January 2020.5–8 As of 14 June 2023, WHO received reports of approximately 767 million COVID-19 cases, with 7 million deaths. 9 Meanwhile, Nepal witnessed approximately 1 million COVID-19 cases, with 12,031 deaths. 10
For effective prevention and control of COVID-19, new guidelines were issued based on developing evidence during the pandemic. Various global and regional apex bodies such as the WHO, Centers for Disease Control and Prevention (CDC), All India Institute of Medical Sciences, and Nepal Medical Council (NMC) recommended COVID-19 infection prevention and control for healthcare workers.11–14 During the second pandemic wave of COVID-19, Alpha, Kappa, and Delta variants were identified in Nepal, with the latter two having higher transmissibility.15–18 Meanwhile, CDC established the airborne transmission of SARS-CoV-2. 19 Among people infected with COVID-19, approximately 40% of the cases were asymptomatic and were less infectious.14,20–22 Furthermore, the NMC guidelines stressed upon the significant risk of aerosol transmission associated with computed tomography (CT) chest scans in poorly ventilated rooms. 14 All these revealed the need for a case detection strategy in Nepal. Hence, various testing strategies were employed, and real-time polymerase chain reaction (RT-PCR) was the recommended strategy to detect COVID-19 cases in Nepal.11,14,23–25 Newer guidelines stated the role of a radiological diagnosis in COVID-19 cases.11,13,14 Also, hospitalization criteria were developed based on Spo2 and respiratory rate to optimize the use of limited resources during the COVID-19 pandemic.12,14 Efficient strategies were required to manage COVID-19 cases during the pandemic, particularly those with severe disease. Hence, prophylactic dose anticoagulation was recommended in severe COVID-19 patients.12,14 Though WHO suggested against convalescent plasma therapy in COVID-19 patients, early use of remdesivir was advocated.11,14,26 Also, initial trials supported the use of inhaled Budesonide in patients at risk for severe disease.27,28 On the contrary, WHO suggested not to use systemic corticosteroids for non-severe COVID-19 patients and advocated against remdesivir use. 26 Despite this, NMC suggested using remdesivir and budesonide for high-risk cases. 29 In severe COVID-19 patients, the emphasis was on awake self-proning for 12–16 h daily. 14 The Nepal government focused on vaccination as a preventive measure, and vaccines were imported from different countries. In Nepal, approximately 62 million doses of vaccines were administered as of 12 June 2023. 10 For the vaccination programs, COVISHIELD/AstraZeneca, Sinopharm COVID-19 vaccine (Vero Cell), Pfizer-BioNTech, Moderna, and Johnson & Johnson/Janssen COVID-19 vaccine were used. The possibility of side effects following vaccination was a significant concern among the population. However, various studies worldwide showed that the side effects after vaccination were primarily self-limiting.30–32 Despite this, the post-vaccination observation period is critical for identifying and managing acute adverse effects.
Many studies were done to assess the knowledge and attitude of health science students regarding COVID-19. A study done in the United Arab Emirates revealed a significant (p-value = 0.001) difference in the total knowledge score of medical students (17.5) and allied health science students (16.5). 33 The study also found that 76% of individuals were unaware of the SARS-CoV-2 transmission routes, and participants believed in the effective control measure taken by the government. 33 A study in Pakistan showed that 71.7% of medical students had adequate knowledge, and 92.5% of them had a positive attitude. 34 In addition, female students were more likely to have good knowledge (AOR = 1.367, 95% confidence interval (CI) = 1.081–1.728) and attitude (AOR = 2.545, 95% CI = 1.708–3.794) than male students. 34 Furthermore, studies done in China and Pakistan revealed that health science students were likely to have good knowledge in their senior years.34,35 A local study from Nepal showed that most medical students had good knowledge and attitude. 36 The data collection tool of these studies had limited questions about managing COVID-19 cases in the context of rapidly evolving guidelines. Hence, they could not assess the knowledge aspect regarding management modalities of COVID-19. Also, these studies could not explore the attitude gaps in context to developing evidence during the second wave of the COVID-19 pandemic. The assessment of knowledge and attitude in health science students regarding COVID-19 is crucial as they are the healthcare workers for the future, and being updated with recent guidelines will foster a culture of evidence-based practice. Hence, we aimed to focus more on the evolving epidemiological and management modalities of COVID-19.
This study was conducted among health science students across 19 health science institutions in Nepal. It aimed to determine the knowledge and attitude, identify gaps, and determine their relationship to various predictor variables.
Methods
Design
This cross-sectional survey involved undergraduate health science students from 19 Nepalese health science institutes.
Setting
Nepal has various universities offering various career opportunities for higher education. Institutions affiliated with Kathmandu University (KU) and Tribhuvan University offer various health science courses. Similarly, autonomous institutions such as the B. P. Koirala Institute of Health Sciences (BPKIHS) and the National Academy of Medical Sciences also offer health science courses. Under the Ministry of Health & Population, Nepal’s Department of Health Services (DoHS) provides therapeutic and preventive services. This study was carried out in 19 health science institutions based on the list of health science institutions by the DoHS. 37
Study population
The study population includes all undergraduate health science students across 19 health science institutions pursuing Bachelor of Medicine and Bachelor of Surgery (MBBS), Bachelor of Dental Surgery (BDS), Bachelor of Science in Nursing (B.Sc. Nursing), and Bachelor of Science in Medical Imaging Technology (B.Sc. MIT) courses.
Inclusion and exclusion criteria
All undergraduate health science students aged 18 years or more across 19 health science institutions pursuing MBBS, BDS, B.Sc. Nursing, and B.Sc. MIT courses who gave consent were included in this study. Students during their internship years were excluded from the study population, as they may possess more information due to direct patient interactions. Also, those who did not give consent were excluded from the study population.
Sample size and sampling technique
Data from the Medical Education Commission showed 8203 seats across all 19 institutions (Supplementary File 1). 38 An expected frequency of 50%, 5% accepted margin of error, and 95% CI was considered for sample size calculation using Epi Info version 7 developed by Centers for Disease Control and Prevention. The total sample size calculated was 367. Non-probability sampling was used for data collection. However, we selected 524 students for the final analysis as the number of respondents was higher than the required sample size (Figure 1).

Selection of study participants.
Questionnaire designs
We developed the questionnaire using various online sources12,14,19,39 under the supervision of experts in epidemiology, infectious disease, and public health. We pretested the questionnaire among 30 undergraduate students of BPKIHS across different streams. Following pretesting, questions were revised and reconstructed. The knowledge and attitude scales were then subjected to reliability analysis. For the knowledge scale, the Cronbach’s alpha and standardized item alpha were 0.707 and 0.716, respectively. The Cronbach’s alpha and standardized item alpha for the attitude scale were 0.652 and 0.710, respectively. The final questionnaire had three sections with a total of 29 questions. The knowledge and attitude section had 18 and 5 questions, respectively (Supplementary File 2).
Variables studied
We considered age, gender, stream of study, year of study, institution, and nationality as the independent variables and knowledge and attitude level as the dependent variables.
Data collection
We collected data using a pre-tested structured questionnaire via Google form base using various social media platforms, email, or other means. We received 588 responses from 30 June 2021 to 11 August 2021. The informed consent form was available in the Google form, and participants could communicate with the investigators through email or telephone to discuss any queries. To avoid multiple responses from a single participant, the participants had to sign in through email. All the data were anonymized to ensure the confidentiality of the participants. The participants were allowed to withdraw at any study stage to promote autonomy. We circulated forms in each institution to avoid selection bias and ensure accurate representation. However, due to the COVID-19 pandemic, avoiding selection bias was a significant challenge.
Statistical analysis
The data from the Google form was extracted into an Excel spreadsheet, followed by data cleaning. Inadequate responses and participants not per the study criteria were removed. Initially, 588 responses were collected. After the data cleaning, 524 responses were included for final data analysis. Entered data were then exported into SPSS version 17 developed by IBM. In the sociodemographic section, categorical data were presented as frequencies and percentages. The continuous variable was expressed in terms of mean and standard deviation. Each question in the knowledge and attitude section was assigned a binary score. Based on the study by Zhang et al., those with less than the median score had poor knowledge/attitude, and those with equal to or more than the median score had good knowledge/attitude. 35 The median score was 10 and 4 for the knowledge and attitude sections, respectively. Responses in the knowledge and attitude section were expressed as frequencies and percentages. Knowledge and attitude score was demonstrated as mean and standard deviation. The bivariate analysis assessed the association between the independent variables and dependent variables. The chi-square test evaluated the association between knowledge and attitude level. All the data were presented as odds ratio (OR) at a 95% CI.
Ethical clearance
The ethical approval (Code No. 01/2021) was taken from the Departmental Research Unit of the School of Public Health and Community Medicine under the Institutional Review Committee, B. P. Koirala Institute of Health Sciences, Dharan, Nepal, which is an extension of the apex body (Nepal Health Research Council) for providing ethical approval in health research. The study subjects were enrolled only after obtaining written informed consent via Google form base.
Operational definitions
Knowledge is defined as the awareness of health science students about COVID-19.
Attitude is defined as the way a health science student thinks and behaves toward COVID-19.
Junior years refer to students in the first and second years.
Senior years refer to third-, fourth-, and fifth-year students.
Results
Sociodemographic information
A total of 524 health science students were included in the study. Table 1 shows the sociodemographic characteristics of the participants. In our study, 57.1% of the participants were female, and 42.9% of the participants were male. Approximately three-fifths (59.4%) of the participants were from BPKIHS, and about four-fifths (79.2%) of them were from the MBBS stream. Also, about two-thirds (66.0%) of the participants were from senior years. More than three-fourths (77.9%) of students were of Nepali origin.
Sociodemographic characteristics of the participants (n = 524).

Knowledge regarding COVID-19
A total of 524 students in the study filled out the knowledge section (Table 2). About 84.2% of students were aware of the structure and the airborne transmission of SARS-CoV-2. Only 15.3% of students knew that SARS-CoV-2 transmission from contaminated surfaces does not contribute significantly to new infections. Less than half (44.8%) of respondents knew that the infectiousness of asymptomatic patients is lower than symptomatic patients. Only about one-third (32.3%) of respondents knew about the risk of aerosol transmission associated with CT chest scans. Nearly two-thirds (64.1%) of the participants knew about prophylactic dose anticoagulation in severe COVID-19 patients. Only 37.0% of the participants knew that convalescent plasma therapy should not be used in hospitalized patients. About 70.4% of respondents knew that empirical antibiotics should be avoided in COVID-19 patients with no clear evidence of COVID-19 infection. Less than half (49.2%) of students knew that remdesivir should be used within 10 days of symptom onset. Also, only about one-third (32.1%) of students knew that remdesivir does not improve patient outcomes on ventilators. About 43.1% of students knew about the early use of inhaled steroids in mild-to-moderate disease patients. Only about one-third (37.0%) of them knew that convalescent plasma therapy should be avoided in hospitalized patients. Also, 88.9% of the participants did not know the recommended duration of awake-prone positioning. More than three-fourths (76.3%) and 70.8% of them knew about the administration site and dosage of the Sinopharm COVID-19 vaccine, respectively. In addition, about four-fifths (77.9%) of them knew about the post-vaccination observation period of the Sinopharm COVID-19 vaccine. The highest mean knowledge score (12.67) was of Manipal College of Medical Sciences (Figure 2). Third- and fourth-year students had higher median knowledge scores (Figure 3). The median knowledge score of students in MBBS (10.00) was more than other streams (Figure 4). Students in BPKIHS (OR = 1.774; 95% CI = 1.243–2.533), junior years (OR = 8.892; 95% CI = 5.814–13.599), and age less than 23 years (OR = 2.985; 95% CI = 2.089–4.266) were more likely to have good knowledge (Table 3).
Knowledge of study participants about COVID-19 (n = 524).

correct responses.

Mean knowledge score of study participants in different institutions of study (n = 524).

Knowledge score of study participants in different years of study (n = 524).

Knowledge score of study participants in different streams (n = 524).
Bivariate analysis showing predictors of good knowledge and attitude levels in study participants.
Attitude toward COVID-19
A total of 524 respondents filled out the attitude section (Table 4). More than four-fifths (85.1%) of the participants had a good attitude. Nearly three-fifths (57.1%) of the participants strongly agree, and around one-third (30.1%) of them agree to volunteer during COVID-19. More than two-fifths (42.2%) of the participants strongly agree, and more than one-fourth (28.1%) of them agree that Nepal will win the fight against COVID-19. About 43.9% of the participants strongly agree, and 36.8% of them agree that another wave of COVID-19 is possible shortly. Also, 86.1% of the participants strongly agree about prioritizing healthcare workers’ resources during the COVID-19 pandemic. Nearly two-thirds (65.3%) of the participants strongly agree, and about one-fourth (24.8%) of them agree with COVID-19 vaccination despite some side effects.
Attitude of study participants about COVID-19 (n = 524).

correct responses.
Figure 5 shows the mean attitude score of the participants across different institutions. The highest mean attitude score was of Manipal College of Medical Sciences (4.67). The third-year and fifth-year students had higher median attitude scores than other years, but it is not statistically significant (Figure 6). BDS students had a higher median attitude score (5.00) than other streams (Figure 7). Students with ages less than 23 years (OR = 24.160; 95% CI: 9.570–60.992) and those in junior years (OR = 4.460; 95% CI = 3.753–5.300) were more likely to have a good attitude level (Table 3). Students in BPKIHS (OR = 0.443; 95% CI = 0.272–0.722) were less likely to have a good attitude. The association between knowledge and attitude level was not statistically significant.

Mean attitude score of study participants across different institutions (n = 524).

Attitude score of study participants across different years of study (n = 524).

Attitude score of study participants across different streams (n = 524).
Discussion
Overall knowledge and attitude
Our study assessed the knowledge and attitude gaps in the context of the developing evidence during the COVID-19 pandemic. In our study, more than half and more than four-fifths of the participants had good knowledge and attitude, respectively, consistent with other studies conducted among health science students in Nepal and abroad.35,36,40–54
Need to bridge the gap in knowledge regarding COVID-19
In our study, more than four-fifths of health science students were aware of the SARS-CoV-2 structure, consistent with the study conducted in Ecuador and Afghanistan.41,50 Breaking the chain of transmission is a primary preventive strategy for COVID-19. Hence, knowledge regarding SARS-CoV-2 transmission is paramount to preventing and controlling COVID-19 infection in hospital and community settings.3,55 In contrast to results in studies done in the universities of Pakistan and Georgia, only about one-sixth of the students knew that transmission from contaminated surfaces did not contribute significantly to new COVID-19 infections.47,56,57 In our study, roughly two-thirds of the participants were unaware of the risk of aerosol transmission in poorly ventilated CT-scan rooms. Adequate knowledge regarding the transmission of COVID-19 is vital to develop better practices to mitigate the spread of the disease. The deficiency in knowledge regarding modes of transmission reflects the need to educate health science students regarding COVID-19 transmission. In addition to mitigating the spread by breaking the chain of transmission, vaccination was a major modality for added protection against COVID-19. In addition to awareness of vaccines, the knowledge of the post-vaccination period is essential to identify and manage immediate complications. Although the Sinopharm vaccine was commonly used in Nepal, only about one-fifth of the participants were aware of the post-vaccine observation period in our study. Hence, the students need to be educated regarding the post-vaccine observation period.
There are very few medications available to treat COVID-19 patients. Injudicious use of antibiotics may lead to an increment in antimicrobial resistance cases and prove detrimental to public health.58–60 Hence, antibiotics should be indicated only in cases with clear evidence of infection. 11 In our study, more than two-thirds of students were aware of the appropriate use of antibiotics in COVID-19, which is consistent with findings in studies in Italy and Pakistan.47,52,61 In addition to antibiotics, antivirals and corticosteroids were used during the COVID-19 pandemic. NMC recommended early use of remdesivir and inhaled Budesonide to manage COVID-19 patients. 14 We found that more than half of the participants were not updated regarding using remdesivir within the first 10 days of symptom onset, and about two-thirds of the students were unaware that remdesivir does not improve outcomes in patients on ventilators. Also, nearly two-fifths of the participants were unaware of the early use of inhaled steroids. Recent evidence-based guidelines advocated against convalescent plasma therapy in COVID-19 patients.11,14 However, two-thirds of the participants were unaware of current recommendations regarding convalescent plasma therapy. In countries with limited availability of medical oxygen, awake-prone positioning was a cost-efficient supportive management strategy for severe COVID-19 patients. 11 However, only about one-tenth of the participants in our study knew the recommended duration for awake-prone positioning. One possible explanation for the knowledge gap regarding treatment strategies might be the lack of exposure to the management of patients. Also, the data regarding COVID-19 were underdevelopment, and preliminary studies could not be used as a reference for educational purposes.
Predictors of knowledge level
Like studies in Saudi Arabia and Indonesia, age and stream were significantly associated with knowledge level.53,54 We found that the knowledge score of MBBS students was more than other streams, consistent with findings from studies done in Jordan, United Arab Emirates, and Vietnam.33,40,52 Usually, we expect senior-year students to have better knowledge. Our study reported that students in their senior years were less likely to have good knowledge, contrasting the studies done in Pakistan, China, Vietnam, and Indonesia.34,35,52,53 Good knowledge regarding COVID-19 among junior-year students may be because of their better attitude toward COVID-19 in our study. Other studies have also reported a positive association between knowledge and attitude.62–64 Despite the evidence, there is a need for further research to identify the factors leading to this observation. We observed that participants from BPKIHS and those under 23 years were more likely to have good knowledge than other colleges in Nepal combined. Students in junior years are younger, which justifies the better attitude of younger students reported in our study.
Good attitude is essential for providing high-quality healthcare service in future
Many countries experienced a scarcity of healthcare personnel to manage COVID-19 cases effectively. Battlefield promotions of health science students were required. Hence, measuring students’ eagerness to volunteer during COVID-19 was critical. In a study done among university students in Ecuador, only 42.1% of the participants were willing to volunteer during the pandemic. 50 However, in our study, most participants were willing to volunteer during COVID-19, consistent with other studies done in Pakistan, Vietnam, and Turkey.47–49,52 Optimism regarding infection control is a complex trait to assess. Optimism may lead to increased drive and motivation to follow protocols. However, too much optimism can be detrimental as the person may perceive the risk as lower. A study from Ecuador observed that only 23.1% of the participants believed COVID-19 would be controlled. 50 However, our study showed that more than two-thirds of the participants were optimistic that Nepal would win the fight against COVID-19, consistent with findings in other studies done in Ecuador, Pakistan, Vietnam, and Turkey33,34,48,52,65 Cautious optimism may be seen as being optimistic and at the same time, being prepared for adverse situations. More than three-fourths of the participants in our study believed in the possibility of another wave soon. This shows that though the students were optimistic regarding the government’s preventive measures, they were also aware of the deficiencies that may lead to another pandemic wave. Most participants were affirmative about prioritizing resources for health workers and the use of vaccines as a preventive strategy, which shows that most students understand the importance of prioritizing resources for the effective management of COVID-19.
Predictors of attitude level
Age, academic level, and institution can significantly affect attitude level. 53 A study in Saudi Arabia reported that younger students had poorer attitudes. 54 In contrast, our study reported that students under 23 years and those in junior years were likely to have a good attitude. This may be because of a positive association between knowledge and attitude.53,62,63 Since younger students had better knowledge, they had better attitudes too. BDS students had a higher median attitude score than other streams. Also, students in BPKIHS were less likely to have a good attitude. Though there are discrepancies in studies regarding good or poor attitudes toward COVID-19 among dental students, only a few studies have been conducted so far comparing various streams.6,66 Further studies are warranted to delineate the possible multifactorial interactions leading to higher scores among BDS students and poor attitudes among BPKIHS students.
Importance of this study
Nepal is a developing nation with limited resources to combat the pandemic. The focus should be on developing healthcare workers with good knowledge and attitude. This study has identified the knowledge regarding various epidemiological and management aspects of COVID-19. Also, attitudes about volunteering, resource prioritization, COVID-19 vaccination, and confidence in government measures have been assessed. Our study has revealed knowledge deficiencies among health science students related to COVID-19. Overall, the students lack a clear understanding of the various treatment and preventive modalities used for COVID-19 patients. Hence, we need to train health science students to improve prevention and management practices related to COVID-19. 66 Our study’s findings suggest establishing a national curriculum and developing intervention programs for health science students. The efforts at the institutional level should be focused on motivating and engaging students regarding evidence-based medicine and its significance in public health. Particular importance should be given to training the students in their senior years.
Strength and limitations
To the best of our knowledge, this study is the first multi-institution study conducted among health science students of Nepal. The results of this study provide baseline data about the knowledge and attitude of health science students toward the COVID-19 pandemic, which might help devise effective strategies and training programs in the future. However, this study is not without limitations. We used a non-probability sampling technique, so the results may not be generalized to the whole population. There is a possibility of self-reporting bias. Also, we might not have approached the students with internet connectivity issues which might have led to bias.
Conclusion
From our study, we can conclude that MBBS students, especially those in their junior years, had adequate knowledge regarding COVID-19. However, students lacked knowledge regarding transmission risk associated with CT scans and the post-vaccination observation period for the Sinopharm vaccine. Also, participants had inadequate knowledge regarding using remdesivir, convalescent plasma therapy, and inhaled steroids in COVID-19. Most participants, especially BDS students, had a good attitude regarding COVID-19. Overall, health science students had adequate knowledge and a good attitude regarding COVID-19.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121231196703 – Supplemental material for Knowledge and attitude regarding the COVID-19 pandemic among undergraduate health science students of Nepal: An online survey
Supplemental material, sj-pdf-1-smo-10.1177_20503121231196703 for Knowledge and attitude regarding the COVID-19 pandemic among undergraduate health science students of Nepal: An online survey by Ayush Anand, Ashwini Gupta, Sweta Singh, Sulav Pyakurel, Rajendra Karkee and Prajjwal Pyakurel in SAGE Open Medicine
Supplemental Material
sj-pdf-2-smo-10.1177_20503121231196703 – Supplemental material for Knowledge and attitude regarding the COVID-19 pandemic among undergraduate health science students of Nepal: An online survey
Supplemental material, sj-pdf-2-smo-10.1177_20503121231196703 for Knowledge and attitude regarding the COVID-19 pandemic among undergraduate health science students of Nepal: An online survey by Ayush Anand, Ashwini Gupta, Sweta Singh, Sulav Pyakurel, Rajendra Karkee and Prajjwal Pyakurel in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank all the participants of the study, and our special thanks to Prof Dr. Paras Pokharel and the School of Public Health and Community Medicine, B. P. Koirala Institute of Health Sciences, Dharan, Nepal, for their constant support and guidance.
Author contributions
A.A. contributed to the conceptualization, design, data acquisition, data analysis, data interpretation, drafting the work, and critical revision of the work. A.S. and S.S. contributed to the design, data acquisition, drafting, and critical revision of the work. S.P. contributed to data acquisition, drafting the work, and critical revision. R.K. and P.P. contributed to the conceptualization, design, data acquisition, data analysis, data interpretation, and critical revision of the work. All authors are accountable for all aspects of the work.
Data availability statement
Anonymized data will be made available on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Departmental Research Unit of the School of Public Health and Community Medicine under the Institutional Review Committee, B. P. Koirala Institute of Health Sciences, Dharan, Nepal (Code No. 01/2021).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.