
Abstract
Improving medication adherence can reduce the burden of cardiovascular disease (CVD) in Saudi Arabia and its related healthcare expenses. This study aimed to assess physicians’ awareness and knowledge of barriers to medication adherence in cardiovascular patients in Saudi Arabia and to evaluate the strategies they employ in clinical practice to enhance adherence. A sample of Saudi Arabian licensed physicians specializing in CVD participated in an observational cross-sectional investigation. Participants were recruited using convenience sampling method through in-person visits conducted at various healthcare facilities. Using a standardized, peer-reviewed questionnaire spanning areas of knowledge, awareness, and practice, data were gathered. SPSS version 27 was used for statistical analysis; multivariate linear regression was utilized to identify independent factors. A total of 265 physicians participated. Among physicians, 44.9% always asked about medication habits, 26.8% about missed doses, 28.3% discussed illness severity, and 19.2% explained consequences of nonadherence. None consistently addressed side effects, though 46.4% did so frequently. Over half (58.1%) reported that 36% to 65% of patients failed to start therapy after the first prescription. Univariate analysis identified age as associated factors for knowledge, and sex, age, and training for practice. Regression analysis identified age and private work significant independent predictor for knowledge (β = −.05, −.68; P = .01, and .03; respectively), and only training remained a significant independent predictor for practice (β = 8.03, P < .001). Physicians showed modest knowledge with major gaps in practice especially educating patients about side effects and consequences of nonadherence. Knowledge was lower among older physicians and those in private practice, while training was the strongest predictor of better clinical practice, highlighting the need for targeted education and training to improve adherence-related practices.
Keywords
Introduction
Still among the primary causes of death worldwide, cardiovascular diseases (CVD), including ischemic heart disease (IHD), greatly affect the global economic load. Those with IHD run a higher risk of hospitalization, myocardial infarction (MI), and mortality. 1 Programs that encourage behavioral change, such as increasing physical activity, improving eating habits, lowering tobacco and alcohol use, and improving medication adherence, are desperately needed to help lower IHD-related morbidity and death. 2 Intervention programs for behavioral support have great potential to help with IHD management as well as prevention. The World Health Organization claims that changes in these important lifestyle-related risk factors could help to avoid up to 80% of diabetes, stroke, and heart disease early instances. 3
A particularly important and changeable behavioral risk factor, medication adherence, is fundamental in the good control of IHD. Adverse clinical outcomes in patients with IHD have been linked in many studies to inadequate adherence to recommended drugs.4,5 Common to many chronic diseases, obtaining ideal adherence remains a major difficulty despite its relevance. Only over half of patients worldwide follow long-term treatments for chronic conditions. 6 Reported adherence rates in those with a history of MI range greatly from 13% to 61%. 7 These numbers underline the urgent necessity of evidence-based treatments meant especially to improve medication adherence in the IHD population.
Improving medication adherence calls for realizing that adherence is a dynamic and multifarious process comprising 3 separate phases: (1) initiation, when a patient starts a new medication; (2) implementation, taking the medication as prescribed over time; and (3) discontinuation, ceasing the medication, either prematurely or as intended at the conclusion of treatment. 8 Adherence barriers vary across different periods, and patients with IHD and related risk factors often face difficulties all along this continuum. For example, about 1 in 5 Medicare patients fail to complete prescriptions within 7 days following percutaneous coronary intervention with a drug-eluting stent. 9 Though evidence links statins to a 45% reduction in mortality risk, less than half of patients remain consistent with statin treatment 1 year after initiation in the implementation phase. 10
During the discontinuation phase, as many as 50% of patients with diabetes, hypertension, or dyslipidemia stop their medications within the first year of prescription. 11 Across all phases, common barriers to adherence include polypharmacy, limited disease knowledge, low health literacy, difficulties accessing medications, forgetfulness, and financial constraints, among others. 12
The knowledge and awareness of IHD risk factors, along with adherence to both pharmacological and non-pharmacological management strategies, were assessed in Saudi Arabia. A public cross-sectional study involving 5170 individuals from the general Saudi population found that 42.9% of participants demonstrated a good level of awareness about the signs and symptoms of IHD. 13
Another public cross-sectional study reported that nearly half of the respondents demonstrated good knowledge of cardiovascular disease risk factors (46.6%) and a strong awareness of disease prevention (71.2%). However, the majority (67.2%) exhibited limited understanding of the clinical features of CVD. 14
A study investigating medication adherence among cardiac patients at King Fahad Medical City Cardiology Clinics revealed that 24.5% of participants had high adherence, 41.7% showed medium adherence, and 33.7% exhibited low adherence to their prescribed treatments. 15
Reducing the disease load in the community and lowering the related healthcare expenditures depend on preventing and controlling IHD. Effective plans call for lifestyle changes like cutting alcohol intake, stopping smoking, supporting good diets, and consistent exercise. 16 Optimizing medication management is also crucial and calls for early identification, quick start of therapy, and guaranteed adherence to prescribed medications. Healthcare professionals, including nurses, pharmacists, and physicians, usually carry out effective interventions for medication adherence. 17 However, nonadherence is a major issue in Saudi Arabia; over half of the patients fail to follow recommended treatments, 18 and about half of the patients neglect to follow recommended therapies.19,20 In addition, a recent study by Almoghairi et al reported low adherence to secondary prevention measures among patients with coronary heart disease following percutaneous coronary intervention (PCI) in Saudi Arabia. 21 Despite this high non-adherence burden, there is limited information regarding physicians’ understanding of the reasons for medication nonadherence and the strategies they apply in routine cardiovascular practice within the Saudi healthcare system. Specifically, cardiac rehabilitation (CR) is strongly recommended by international guidelines because it helps patients follow their medications, lowers the risk of repeat heart problems, and improves overall health. However, CR programs are not widely used in Saudi Arabia due to limited availability and referral challenges, so many patients do not get structured support to take their medications correctly. These gaps show the need to understand how physicians are aware of, knowledgeable about, and actively support medication adherence in their daily practice. 21 Therefore, this study aimed to assess physicians’ awareness and knowledge of barriers to medication adherence in cardiovascular patients in Saudi Arabia and to evaluate the strategies they employ in clinical practice to enhance adherence.
Methods
Study Design and Ethical Considerations
The study was an observational cross-sectional study involving physicians specializing in CVD. Data collection started in November 2024 and was finished in February 2025, when the required sample size was recruited. Ethical approval was obtained from the Institutional Review Board of the Faculty of Pharmacy, Jadara University with IRB number (PHARM-JA-8/2024) and the ethical approval was exempted by the department of training, institutional development, and academic affairs in AL-Jouf region, Ministry of Health, Kingdom of Saudi Arabia. Written informed consent was obtained from all participants prior to recruitment. All data were anonymized to ensure confidentiality.
Inclusion and Exclusion Criteria
The study included licensed physicians specializing in CVD. Eligible participants must hold a cardiology specialist license. Participants were excluded if they were not cardiology specialists, were still in training and not fully licensed, lacked a valid cardiology license from the Saudi Ministry of Health, were retired or non-practicing, were not involved in patient care, or did not provide consent or complete the questionnaire.
Sample Size Calculation
To identify physicians who do support their patients’ medication adherence, reported to be 45.6% in a previous study, 22 a sample size of 265 individuals was estimated assuming a 95% confidence level and a 6% margin of error according to the following equation, 23 where n represents the sample size, z is the z-statistic corresponding to the desired confidence level, P is the expected prevalence, and d is the allowable margin of error.

Data Collection Tool and Outcome Measure
Data was collected using a validated, peer-reviewed questionnaire developed by Aguiar et al., and published by Springer Nature, administered with permission (License No. 6216570753921, and 6217380212044 CC BY-NC). 24 Face validity and content validity were assessed and established through expert panel review. To assess physician knowledge, perceptions, and practices regarding patient medication adherence, a structured questionnaire was developed and administered. The instrument consisted of 5 main sections: General Awareness, Knowledge, Patient Awareness, Practice, and Respondent Characterization.
In the General Awareness section, physicians were asked whether they had received any formal education or training on improving medication adherence, such as postgraduate courses, conference participation, or involvement in related studies. They were also queried on how frequently they inquire whether patients take their prescribed medications and whether they miss any doses. Physicians were further asked whether they reinforce adherence during consultations. If so, they were prompted to indicate the frequency with which they employed specific adherence-promoting strategies, including explaining disease severity, discussing the consequences of nonadherence, detailing the purpose of each medication, clarifying side effects, and demystifying common misconceptions. Additionally, physicians could report any other adherence-related actions they regularly undertake. Respondents also estimated the proportion of consultation time dedicated to discussing these matters.
The Knowledge section aimed to assess physicians’ perceptions of the utility of various information sources in evaluating patient adherence. These included patient interviews, standardized questionnaires (targeted at patients or caregivers), clinical observations in the medical record, pharmacy claims data, prescribing records, patient diaries or mobile applications, appointment-keeping records, hospital admissions, laboratory results indicating drug levels, and pill counts. Respondents rated each source using a five-point Likert scale from “Very useful” to “Totally useless.”
In the Patient Awareness section, physicians were asked to estimate the proportion of cardiovascular patients in Saudi Arabia who (1) fail to initiate treatment upon first prescription, (2) take their medications differently than prescribed (eg, skipping doses or incorrect timing), and (3) discontinue treatment prematurely. Subsequently, physicians were instructed to reflect on the last 10 patients with cardiovascular disease they had seen who exhibited poor disease control. For these patients, physicians indicated how many cases they attributed to lack of medication efficacy, poor adherence to lifestyle recommendations, or poor medication adherence. Additionally, under a hypothetical scenario in which all 10 patients admitted nonadherence, physicians identified perceived causes, such as forgetfulness, side effects, financial barriers, communication issues, disease misperception, lack of understanding, treatment complexity, lifestyle interference, or confusion arising from medication packaging or instructions.
The Practice section examined the frequency with which physicians employed various methods to assess adherence in their last ten patients with cardiovascular disease. Methods included standardized questionnaires, pill counts, prescription record review, clinical judgment, laboratory drug monitoring, and attendance records. Physicians were also asked to evaluate the perceived usefulness of multiple adherence-improving strategies, including pillboxes, fixed-dose combinations, cost-reducing measures, simplified dosing regimens, therapy adjustment, mobile reminders, enhanced communication, personalized care plans, shared decision-making, educational interventions, and motivational techniques.
Finally, the respondent characterization section collected demographic and professional information. This included specialty areas, primary workplace settings (eg, public hospital, private practice), age, and sex.
Recruitment
Physicians were recruited using convenience sampling method through in-person visits conducted at various healthcare facilities in Saudi Arabia (Northern Saudi Arabia, Riyadh, and Madina). This region includes diverse network of hospitals and primary healthcare centers. Eligible physicians who were available and willing to participate at the time of data collection were invited to complete the questionnaire. These visits were aimed at raising awareness about the study and encouraging voluntary participation among eligible physicians.
Statistical Analysis
Data was analyzed using descriptive and inferential statistical methods. Descriptive statistics, including frequencies, percentages, means, standard deviations (SD), median, and interquartile range (IQR) were used to summarize the characteristics of the physicians and their responses across the 4 domains: education, awareness, practice patterns, and communication strategies. Normality of practice score was checked using the Kolmogorov–Smirnov test, although our sample size aligns with the sample size required for the central limit theorem. 25 To examine the relationship between continuous variables, such as practice score, and sociodemographic factors, t-tests were applied, as appropriate. Correlation test using the Pearson correlation coefficient was utilized for testing the relationship with age. Linear regression analysis was performed to identify predictors of high knowledge and practice scores, controlling for potential confounding variables. A p-value of <.05 was considered statistically significant. All analyses were conducted using SPSS (version 27). The results of the analysis were presented in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 26
Results
Characteristics of the Studied Subjects
As shown in Table 1, the study included 265 practitioners, with males representing the majority at 64.15% (n = 170). The mean age of the participants was 45.2 years, with a SD of 9.1 years. Other characteristics are presented in the Table 1.
Characteristics of the Studied Practitioners.
Note. SD = standard deviation.
General Assessments
When asking patients about medication-taking habits (Q2), 44.9% always inquired, while 25.3% did so frequently, and 23.0% sometimes. Similarly, 47.5% frequently and 26.8% always asked patients about missed doses (Q3). Regarding providing information about the severity of illness (Q5.1), 52.5% frequently addressed this, with 28.3% always doing so. Informing patients about the consequences of nonadherence (Q5.2) was less consistent, as only 19.2% always and 43.4% frequently shared this information. While 43.0% frequently explained the purpose of each medication (Q5.3), only 18.9% always did. Notably, none of the practitioners always informed patients about the most frequent side effects (Q5.4), with 46.4% doing so frequently and 37.4% sometimes. Most practitioners (67.9%) reported having education or training on medication adherence (Q1), and all practitioners (100%) indicated they reinforced medication adherence (Q4). The median proportion of time spent discussing with patients was 35%, with an interquartile range of 20% to 50% (Table 2).
General Assessment of the Studied Practitioners.

IQR = interquartile range.
Knowledge and Practice Assessment
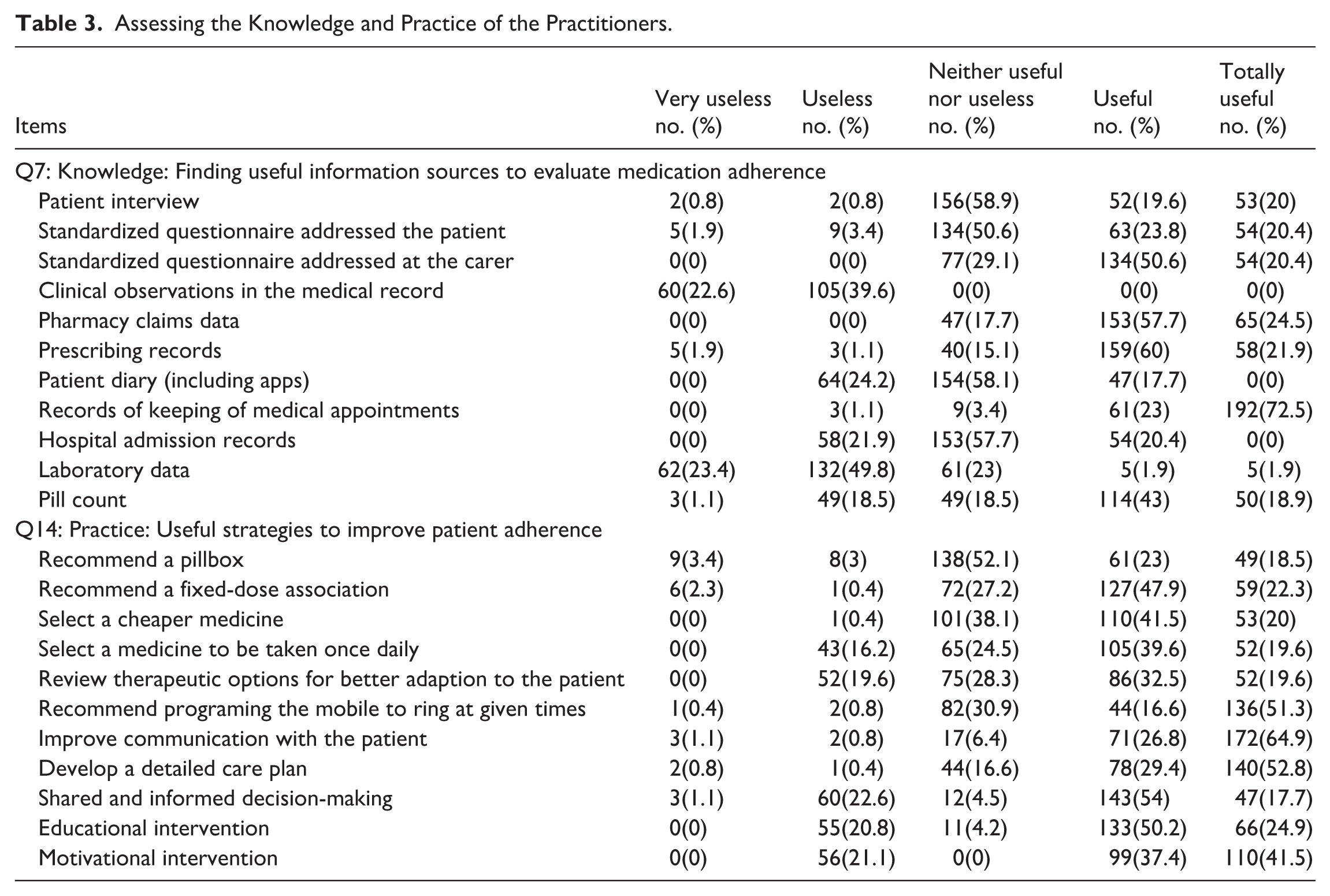
For identifying useful information sources (Q7), patient interviews were rated as “totally useful” by 20.0% and “useful” by 19.6%, while standardized questionnaires addressed to patients and carers were perceived as “totally useful” by 20.4% each. Clinical observations in medical records were deemed “useless” or “very useless” by 62.2% collectively, reflecting limited perceived value. Conversely, pharmacy claims data (57.7% useful, 24.5% totally useful) and prescribing records (60.0% useful, 21.9% totally useful) were highly regarded. Records of medical appointments stood out, with 72.5% rating them as “totally useful,” the highest among all methods. However, tools like hospital admission records, laboratory data, and patient diaries were less favorably assessed, with “neither useful nor useless” being the predominant response.
Regarding strategies to improve adherence (Q14), improving communication with patients was highly valued, with 64.9% rating it “totally useful” and 26.8% “useful.” Developing detailed care plans (52.8% totally useful) and programing mobile reminders (51.3% totally useful) were also popular. Fixed-dose associations (47.9% useful) and selecting cheaper medications (41.5% useful, 20.0% totally useful) were practical strategies. Educational (50.2% useful) and motivational interventions (41.5% totally useful) were also favored. However, strategies like recommending pillboxes or reviewing therapeutic options received more moderate ratings, highlighting variability in perceived effectiveness (Table 3).
Assessing the Knowledge and Practice of the Practitioners.
Patient Awareness and Practitioner Practices Assessments
For patient awareness, a significant proportion (58.1%) reported that 36% to 65% of patients failed to initiate their medication upon the first prescription (Q8), with only 1.9% indicating an 86% to 100% rate of such behavior. Regarding patients taking medications different from those prescribed (Q9), the majority (56.2%) estimated this occurred in 16% to 35% of cases, while 25.3% reported a rate of 0% to 15%. Early discontinuation of prescribed medications (Q10) was predominantly noted in 16% to 35% of patients (62.3%).
For the last 10 patients with poor disease control (Q11), poor adherence to lifestyle recommendations was cited most frequently (median 8, IQR 5-9), followed by poor medication adherence (median 7, IQR 7-8) and lack of medication efficacy (median 3, IQR 2-4). Among patients with poor disease control due to nonadherence (Q12), therapy complexity was the most cited cause (median 7, IQR 6-8), along with communication failures (median 5, IQR 3-5) and medication packaging issues (median 5, IQR 3-8). Other factors included forgetfulness, adverse drug effects, economic constraints, disease perception, and lack of understanding of therapeutic regimens, with medians ranging from 2 to 3.
Practitioners’ practices (Q13) showed that among the last 10 patients, prescription records (median 7, IQR 6-8) and records of keeping medical appointments (median 7, IQR 6-9) were most commonly used to assess adherence. Pill counts were moderately utilized (median 5, IQR 5-8), while standardized questionnaires and clinical judgment were less frequently employed (both median 2, IQR 2-2). Monitoring drug levels in blood or urine was rare (median 1, IQR 0-1). These findings highlight critical gaps in patient adherence and the need for more consistent and effective assessment strategies by practitioners (Table 4).
Assessing Patient Awareness and the Practitioner’s Practice.

IQR = interquartile range.
Determinants of the Practitioners' Knowledge and Practices Using Univariate Analysis
As shown in Table 5, private practice affiliation did not significantly impact the knowledge score (P = .07), with mean scores of 37.55 (SD = 2.37) for non-private practitioners and 36.98 (SD = 2.44) for private practitioners. Moreover, training did not significantly affect the knowledge score (P = .728), as practitioners who received training scored higher (mean = 37.21, SD = 2.2) compared to those without training (mean = 37.09, SD = 2.9). Gender also showed a nonsignificant association (P = .271), with females achieving numerically higher knowledge scores (mean = 37.39, SD = 2.62) than males (mean = 37.05, SD = 2.3). However, age was negatively correlated with knowledge scores (r = −.15, P = .015), indicating that younger practitioners tended to have better knowledge scores.
Univariate Analysis for Factors Affecting Knowledge Score (Q7).

Note. Independent t-test was used with a significant level of 0.05 indicating by (*) symbol.
The univariate analysis presented in Table 6 revealed several factors influencing the practice scores of practitioners (Q13,14). Private practice affiliation did not significantly impact the practice score (P = .75), with mean scores of 68.41 (SD = 4.395) for non-private practitioners and 68.21 (SD = 5.281) for private practitioners. However, training demonstrated a highly significant effect (P < .001), as practitioners who received training scored higher (mean = 70.91, SD = 3.335) compared to those without training (mean = 62.72, SD = 2.963). Gender also showed a significant association (P = .02), with females achieving higher practice scores (mean = 69.24, SD = 4.307) than males (mean = 67.74, SD = 5.284). Additionally, age was positively correlated with practice scores (r = .23, P < .001), indicating that older practitioners tended to have better practice scores. These findings highlight the importance of training, gender differences, and age as significant contributors to the quality of practice among practitioners.
Univariate Analysis for Factors Affecting Practice Score (Q13, Q14).

Note. Independent t-test was used with a significant level of 0.05 indicating by (*) symbol.
Determinants of the Practitioners' Knowledge and Practices Using Multivariate Analysis
The linear regression analysis aimed to identify predictors of the knowledge score revealed that among the variables, age and private were the only significant predictors, with a little negative effect for age (Beta = −.05, SE = 0.02, t = −2.7, P = .01), suggesting that practitioners scored approximately 0.05 points lower on the knowledge scale for every year increased in the age.
Similarly, being affiliated with private practice (Beta = −.68, SE = 0.32, t = −2.14, P = .03) reduced the knowledge score by 0.68 compared to the public sector.
On the other hand, training and being female did not significantly influence the knowledge score. These results emphasize that younger practitioners and being affiliated with public practice were associated with better knowledge score, while factors such as training and gender did not significantly contribute to the predictive model (Table 7).
Linear Regression for Predicting Knowledge Score (Q7).

Beta = regression coefficient; SE = standard error.
Significant p-value at .05 level of significance.
The linear regression analysis aimed to identify predictors of the practice score revealed that among the variables, training was the only significant predictor, with a positive effect (Beta = 8.03, SE = 0.44, t = 18.18, P < .001), suggesting that practitioners who received training scored approximately 8 points higher on the practice scale.
Age showed a non-significant positive association with practice scores (Beta = .03, SE = 0.02, t = 1.33, P = .19), indicating that age was not a strong predictor in this model. Similarly, being affiliated with private practice (Beta = .47, SE = 0.43, t = 1.10, P = .27) and being female (Beta = .48, SE = 0.42, t = 1.15, P = .25) did not significantly influence the practice score (Table 8).
Linear Regression for Predicting Practice Score (Q13, Q14).

Beta = regression coefficient; SE = standard error.
Significant p-value at .05 level of significance.
Discussion
This study examines all of the physicians’ awareness, knowledge, and practice regarding how to maintain patients on their drugs throughout a broad spectrum of medical environments. By considering both behavioral and systemic elements influencing adherence, our findings enable us to better grasp present gaps in practice, relevant areas for intervention, and what constitutes high-quality treatment. Doctors are rather crucial in identifying, resolving, and minimizing the issues that make it difficult for patients to take their prescriptions as advised since they are the first persons patients consult during therapy. Their ability to adequately communicate to patients, identify early nonadherence indicators, and apply tried-and-true strategies that have shown success is absolutely vital. 27 However, physician engagement in adherence-related practices remains understudied, especially in real-world clinical contexts across different healthcare settings in Saudi Arabia.
Notably, this study goes beyond patient-level barriers and focuses on the provider perspective, a relatively underexplored domain. It highlights how physician behavior, training, communication, and assessment methods critically influence adherence outcomes. The statistical rigor employed, including both univariate and multivariate analyses, enables a robust understanding of factors that predict better adherence-related practices. Our findings underscore the urgent need for targeted educational interventions and standardized assessment tools to enhance physicians’ capacity to support patient adherence.
The study’s results yield several key insights. First, while most practitioners are engaged in medication adherence support, there remains significant variability in how they assess and intervene in nonadherence. Although 100% reported reinforcing adherence, the depth and consistency of their patient interactions were often limited. Few consistently educated patients on the importance of adherence, potential side effects, or the risks of nonadherence, components shown to significantly influence patient behavior.
Secondly, tools used to assess adherence were predominantly indirect, such as prescription and appointment records, while more patient-centered approaches like interviews and standardized questionnaires were underutilized. This indicates a gap in applying personalized adherence assessments despite their recognized value in literature.
Importantly, training emerged as the most powerful predictor of adherence-related practices, emphasizing the necessity of structured educational programs to improve practitioner engagement in this domain. Physicians affiliated with private practice and older age groups showed lower knowledge scores. Age and gender also influenced practices to a lesser extent, though these effects diminished in multivariate analysis.
The results reveal substantial variability in how physicians approach medication adherence. While all practitioners reported reinforcing adherence (100%), proactive inquiry into adherence behaviors was inconsistent. Only 44.9% always asked about medication-taking habits, and even fewer always explained medication purposes (18.9%) or side effects (0%). This inconsistency indicates a gap between awareness and practice, where adherence is emphasized conceptually but not operationalized consistently in consultations.
These findings align with prior studies demonstrating that although providers recognize the importance of adherence, practical constraints such as time limitations, perceived patient receptivity or lack of structured communication tools may hinder consistent implementation.27,28 Enhancing routine, structured discussions about medications, possibly through checklist-driven consultations or integrated electronic prompts, could bridge this gap.
Our study highlights notable variation in the perceived utility of adherence assessment methods among physicians. Traditional sources, such as patient interviews and pharmacy claims, were rated positively, suggesting that physicians rely on direct patient interactions and prescription refill data to gage adherence. However, standardized questionnaires and clinical judgment were underutilized, with median scores of only 2, indicating a lack of integration of formalized tools into routine practice. In contrast, medical appointment records were viewed as the most useful, with 72.5% of physicians rating them as “totally useful,” reinforcing the preference for indirect, behavior-based indicators over structured adherence measurement tools.
Their availability and relevance in therapeutic settings help to explain this predilection for behavior-based indicators. Instead of using validated adherence metrics, physicians often rely on visible markers, such as missing visits or inconsistent drug refills. On the other hand, subjective or insufficient signals could reduce diagnostic accuracy, therefore leading to erroneous impressions of individual adherence. The findings show that proven adherence monitoring methods call for institutional support and training for application in clinical settings. This will facilitate a more consistent and accurate evaluation of patient compliance. 29
Many studies have looked at the effectiveness and frequency of adherence assessment methods, thereby enabling a comparison of our results with theirs. Examining multiple validated self-reported adherence instruments, including the Medication Adherence Questionnaire (MAQ) and the Morisky Medication Adherence Scale (MMAS-4), Nassar et al. 30 showed that these organized adherence strategies are not used often in clinical settings, which is consistent with our observations regarding the low use of consistent physician surveys.
Practitioners’ perceptions of patient behavior revealed that 36% to 65% of patients do not initiate treatment post-prescription, while early discontinuation was similarly common. Poor adherence to lifestyle modifications was the top cause of poor disease control, followed by medication nonadherence.
Importantly, therapy complexity and communication failures were cited as major contributors to nonadherence. This underscores the multifactorial nature of adherence challenges and the need for a multidimensional approach. Simplifying regimens and improving provider-patient communication are well-documented strategies for improving adherence and the data here support their prioritization in local practice improvement efforts. 31
The most significant determinants of knowledge score were age and private workplace, whereas physicians affiliated with private practice and older age groups showed lower knowledge scores in the multivariate analysis. Our results are matched with previous study showed a decline in physicians’ knowledge with age. 32
In addition, our study highlights that training is the most significant determinant of higher practice scores, with physicians who received adherence-related training scoring 8 points higher on average. This reinforces the critical role of continued professional education in shaping clinical behaviors related to adherence. While female physicians and older age groups showed higher practice scores in univariate analysis, these associations were not significant in the multivariate model, suggesting that training has an independent and robust effect, transcending demographic factors.
The emphasis on training is supported by broader literature indicating that educational interventions targeting healthcare professionals can significantly improve adherence-supporting behaviors. 33
The importance of educational interventions in shaping physician practices is well-documented. A scoping review examined interprofessional education in healthcare, finding that structured training programs significantly enhance competency development, communication, and teamwork among healthcare professionals. 34 Furthermore, it was conducted a systematic review on educational interventions in healthcare, finding that structured training programs significantly improve evidence-based practice competencies among physicians. 35 This aligns with our findings that adherence-related training directly improves physician practice scores, emphasizing the need for institutionalized adherence education in medical curricula and continuing medical education (CME) activities.
Our study found that female physicians had higher practice scores in univariate analysis, but this association was not significant in the multivariate model. This is consistent with previous findings, which explored gender-based differences in physicians’ prevention-related practices. 36 The study found that female physicians were more likely to engage in preventive counseling and screening, but these differences diminished when controlling for training and institutional support, reinforcing our conclusion that training is the primary determinant of adherence-supporting behaviors.
Several studies have looked at how gender affects decisions about what to wear. Researchers looked at differences in prescribing practices between men and women among older people and found that female doctors tend to be more conservative and patient-centered when they write prescriptions. 37 This fits with our finding that female doctors had higher practice scores. However, the study also said that prescribing habits are shaped by training and institutional standards. This supports our conclusion that training is the main factor that affects doctors’ practices.
In our study, older physicians had better practice scores in the univariate analysis, but this link wasn’t important in the multivariate model. A previous study looked at how age affects health-related behaviors and found that older doctors were more likely to do preventive health practices. However, their behaviors that helped them stick to their plans were greatly affected by their training and the rules of their institution. 38 This supports our conclusion that age alone does not determine adherence-related practices, but rather structured training programs play a more decisive role.
A systematic review examined the effectiveness of educational interventions in improving evidence-based practice skills among healthcare professionals. 39 The study found that multifaceted training programs, including mentoring and tutoring, significantly enhance clinical decision-making and adherence-supporting behaviors. This supports our conclusion that structured training programs should be integrated into medical education and professional development.
Limitations
This study has several limitations. First, its cross-sectional design precludes any inference of causality. Second, the use of self-reported questionnaires may introduce reporting bias. Third, the relatively small sample size may limit the generalizability of the findings. Additionally, the study was conducted in northern Saudi Arabia, Madina, and Riyadh, which may further restrict the applicability of the results to the broader national population.
Conclusion
Knowledge scores were inversely affected by age and private practice in the multivariate analysis, emphasizing the importance of focusing on advancing knowledge among those groups. On the other hand, training, gender, and age were significantly associated with higher practice scores in the univariate analysis, with trained practitioners, females, and older individuals performing better, highlighting the importance of targeted training and demographic factors in improving adherence-related practices. However, in the regression model, training was the only significant predictor of higher practice scores, with a strong positive association, while age, gender, and working in the private sector showed no significant impact, underscoring the pivotal role of formal training in improving practitioners’ adherence-related practices.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261427422 – Supplemental material for Physicians’ Awareness and Knowledge of Barriers to Medication Adherence in Cardiovascular Patients and Strategies Employed in Clinical Practice in Saudi Arabia: A Cross-Sectional Study
Supplemental material, sj-docx-1-inq-10.1177_00469580261427422 for Physicians’ Awareness and Knowledge of Barriers to Medication Adherence in Cardiovascular Patients and Strategies Employed in Clinical Practice in Saudi Arabia: A Cross-Sectional Study by Ahmed R. Gardouh, Mahmoud S. Abdallah, Khalid Dhaiffallah Alanazi and Khlood Mohammad Aldossary in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
Many thanks to Princess Nourah Bint Abdulrahman University Researchers Supporting Project Number (PNURSP2026R486), Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia.
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board of the Faculty of Pharmacy, Jadara University with IRB number (PHARM-JA-8/2024) and the ethical approval was exempted by the department of training, institutional development, and academic affairs in AL-Jouf region, Ministry of Health, Kingdom of Saudi Arabia.
Consent to Participate
Written informed consent was obtained from all participants prior to recruitment. All data were anonymized to ensure confidentiality.
Author Contributions
Ahmed R. Gardouh, Mahmoud S. Abdallah, Khlood Mohammad Aldossary: conceptualization and methodology. Khalid Dhaiffallah Alanazi: participant’s recruitment and follow-up. Ahmed R. Gardouh, Mahmoud S. Abdallah, Khalid Dhaiffallah Alanazi, Khlood Mohammad Aldossary: data analysis, data curation, writing—original draft preparation, visualization, investigation, and data interpretation. Ahmed R. Gardouh and Mahmoud S. Abdallah: supervision. All authors: writing—reviewing and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusion of this article will be made available by the authors upon request.