
Abstract
Background:
Type 2 diabetes mellitus is usually associated with long-term macrovascular and microvascular complications that negatively impact the patient’s quality of life and add economic burden to the healthcare system. Understanding patients’ perspectives on medication nonadherence is essential for planning the appropriate methods and strategies to improve medication adherence among patients with uncontrolled diabetes.
Aim:
Therefore, this study aims to explore patients’ perceptions of the barriers to medication adherence through the Social Health determinants framework.
Method:
After obtaining ethical approval, qualitative face-to-face interviews with a sample of patients with type 2 diabetes mellitus (uncontrolled diabetes) were conducted. Interviews were audio-recorded, and then the data were analyzed using thematic analysis to identify essential themes related to the patient’s views.
Results:
Fifteen patients with type 2 diabetes mellitus were interviewed. Potential barriers to antidiabetic medications were identified and categorized based on the Social Determinants of Health domains. The patient’s health perceptions and behaviors were found to positively or negatively impact medication adherence. Beliefs toward antidiabetic medications, polypharmacy, medication-related problems, and the relationship between patients and their healthcare providers that related to healthcare access and quality domains were also reported as potential barriers to medications. Financial constraints, social stigma, and family support were other social health determinants factors that were found to have either positive or negative impacts on adherence. Nevertheless, using mobile health applications was suggested to facilitate medication adherence.
Conclusion:
Social Determinants of Health, such as education about type 2 diabetes mellitus, quality and access to healthcare, and social stigma and support, might significantly affect medication adherence among type 2 diabetes mellitus patients. This study’s findings can aid the development of suitable patient-specific tools and strategies to enhance medication adherence.
Introduction
The prevalence of diabetes mellitus (DM) in Saudi Arabia is projected to rise to 21.4% by 2045, 1 which could make the disease a clinical and public health concern and burden on the Saudi health system. DM has a serious impact on the morbidity and mortality of the Saudi population. According to the International Diabetes Federation (IDF), Saudi Arabia had the highest number of diabetes-related deaths among the Gulf countries. 1 DM is associated with long-term macrovascular and microvascular complications (e.g., cardiovascular, retinopathy, and renal failure), and with no specific cure to the condition, the mortality rate would increase significantly. 2 Thus, creating a very high economic burden on healthcare institutions. Based on IDF data, the total diabetic health expenditures in Saudi Arabia are projected to rise from 7459.5 to 10,045.2 million. 1
Treatment interventions for Type 2 Diabetes Mellitus (T2DM) patients include diet, increasing physical activity, and antidiabetic medications to achieve therapeutic goals and control blood glucose. 3 Nevertheless, despite the availability of these approaches and strategies, previous studies have shown that it is difficult for patients to achieve a good blood glucose level. Medication nonadherence is one of the main reasons that patients cannot reach an ideal glycemic control.4,5 The patient’s adherence to medication in T2DM is suboptimal on a global scale. Nonadherence to medications for oral hypoglycemic medications ranges from 7% to 64% and 19% to 46% for insulin only or insulin concomitant therapy.6,7
Several reports identified the barriers to medication nonadherence8,9 and the impact of these barriers on patients’ nonadherence, such as lack of knowledge related to DM and medications, lack of communication with healthcare providers, patient characteristics, and attitudes toward their disease and medications, and complexity of medication regimens.8,9 Similarly, understanding the patients’ voices and views was essential for treatment decision-making and facilitating adherence. Previous research highlighted that patients with T2DM tend to describe several barriers and facilitators in relation to medication adherence, such as emotion; positive health benefits from treatment and negative emotion (e.g., fear of complications) lead patients to do better and stay on track with treatment. 10 Besides the medication administration, lack of information and knowledge, social and cultural beliefs, financial burden, the patient-healthcare provider relationship, and communication were reported as important factors that might impact adherence. 10
Indeed, the barriers to medication adherence among patients with T2DM can be found in different communities, and several researchers have concluded the importance of investigating the barriers to medication adherence among patients through subjective methods. However, a recent study that assessed adherence to antidiabetic medications quantitatively reported that the nonadherence to antidiabetic medications remains unsolved, and further studies are needed to understand the reasons. 11 This study was conducted in Jazan, Saudi Arabia, and found that 34% of T2DM patients were not adherent to their antidiabetic medications. 11 The patients living in this community might have their own cultures, such as nutritional style, lack of appropriate exercise, gender and social norms, and economic status, which might lead to nonadherence. Accordingly, this study was planned and conducted to further understand the barriers and facilitators to antidiabetic medications among those populations to design and implement appropriate interventions to reduce these barriers. In addition, understanding the potential barriers to medication adherence by applying the Social Health determinants (SDoH) might provide a comprehensive view that might help improve medication adherence and health outcomes among T2DM patients. Based on the World Health Organization (WHO), SDoH is “the conditions in which people are born, grow, live, work and age.” 12 The SDoH is categorized into five domains based on the Healthy People 2030 initiative, led by the Office of Disease Prevention and Health Promotion in the United States of America: economic stability, education, healthcare access, neighborhood and built environment, and social and community context. 13 Indeed, providing high-quality healthcare services for T2DM patients requires policymakers to understand patients’ circumstances, balancing their health perceptions with social needs. Thus, conducting qualitative research would facilitate the identification of the factors from the patient’s perspective for effective interventions due to the complexity of medication adherence. Therefore, this study aims to explore the barriers to medication adherence via a holistic and qualitative approach through the SDoH framework in a natural clinical setting.
Method
A qualitative research method, a face-to-face interview, was used in this study to enable an in-depth exploration of the participants’ views. This is a follow-up study of a previous cross-sectional study that was conducted to assess adherence among patients with T2DM in Jazan, Saudi Arabia. 11 A topic guide guided the interview to cover critical areas while allowing freedom to explore areas touched on by the interviewee. Each patient participated in one interview only. Patients with T2DM who had uncontrolled diabetes (fasting blood glucose ⩾ 126 mg/dl or glycated hemoglobin (HbA1c) > 6.5%) and had an outpatient follow-up visit at the Endocrinology and Diabetes Centre in the Jazan area were included in this study. Patients with other types of DM (e.g., prediabetes, Type 1 DM, gestational diabetes), or had controlled glycemic levels (HbA1c less than 6.5%) were excluded. All inclusion criteria were verified using patients’ medical records before commencing the interview.
Study design
Convenient purposive sampling was used to recruit the target patients based on the study inclusion criteria. The participant’s information sheet, which includes an invitation to this study, was handed to the physician at the diabetic center to introduce the study to their patients. The interview was conducted upon the patient’s approval in a convenient, quiet room in the diabetic center. Before starting the interview, the patients were given a fresh copy of the consent form to sign and an opportunity to ask further questions about the study. For illiterate patients, the study’s purpose and items of the informed consent were verbally explained to them, and then, upon their approval, they were asked to sign and date the form. Furthermore, the researchers emphasized that the participation was voluntary, there were no right or wrong answers, withdrawal, refusal, or their answers would not impact their care, and all responses would be anonymous and would not be communicated with their healthcare providers. The interviews were conducted by two researchers who are pharmacists in academia and have experience in the qualitative type of research.
The first two interviews were conducted as a pilot to test the topic guide; however, no changes were made to the topic guide, and the collected data were used in the final analysis. The topic guide was an active document continually revised and informed by previous interviews, as usual for this research method. The interviews were conducted until data saturation was reached (no new information had emerged).
Topic guide
An interview topic guide was developed to address the aims of this study. A topics guide was designed based on the literature search of factors that might impact medication adherence.
The interview topic guide involved the following broad topics: personal views and experience of T2DM and diabetic medication, barriers to diabetic medications, and suggestions to improve adherence. The developed topic guide included open-ended and follow-up questions for free patient discussion. The topic guide can be found in Appendix 1.
In addition to the topic guide, the researchers collected the following data: demographic data (age, gender, area of residence, educational status, marital status, employment status, duration of diabetes, diabetes-related complications, presence of comorbidities, medications used for diabetes or other conditions), and laboratory findings (HbA1c%).
Data analysis
Thematic analysis, mainly a deductive approach, was applied to identify the themes or patterns within the data. 14 The interviews were audio-recorded, and the audio files were typed word-for-word. Any information that could identify patients was anonymized. The analysis was carried out on the Arabic version of the transcripts, and the selected quotations for each theme and subtheme were translated into English by one of the research teams and then checked by another bilingual researcher. Two researchers independently conducted the analysis manually to ensure the reliability and consistency of the generated codes and themes. The analysis process was conducted systematically, and initial codes were identified during the transcribed stage by the primary researcher, who conducted the interviews and then compared and integrated with the final code matrix. All transcripts were coded and recorded according to a common idea or meaning. After extensive discussion, similar codes were clustered and placed under respective themes. During this, the data were synthesized based on four of the five domains of the SDoH: education access and quality, healthcare access and quality, economic stability, and social and community context. However, no data were identified that related to the fifth domain of SDoH, “neighborhood and built environment.” 13 Themes were reviewed, checked by all research teams, and finalized, as shown in Table 2 and Figure 1.

Themes for T2DM medication adherence based on the social determinant of health domain.
Results
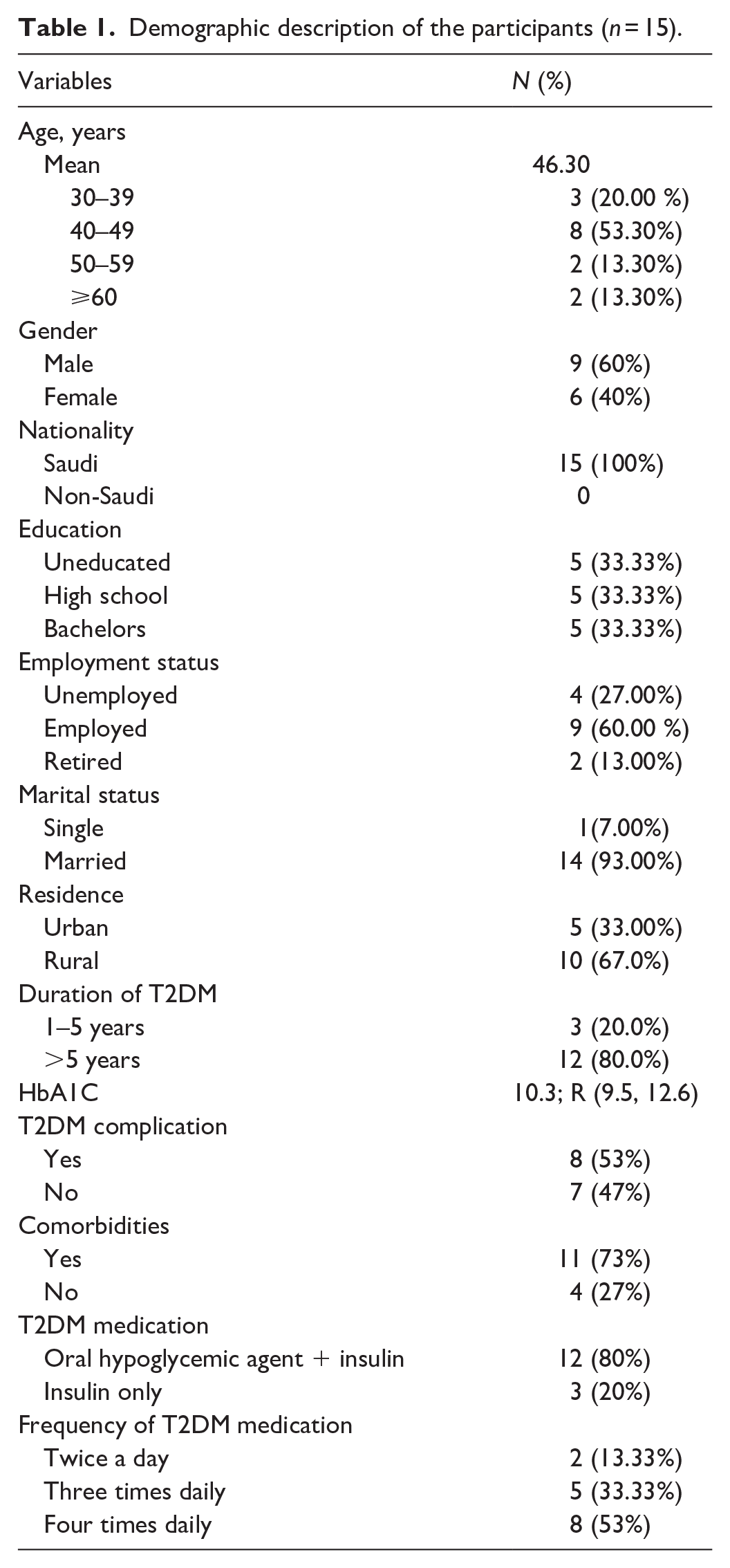
A total of 15 patients with uncontrolled T2DM participated in this study. Face-to-face interviews were conducted between February and June 2023. The interview duration ranged from 15 to 40 min. The interviews were conducted with 9 (60%) male and 6 (40%) female patients at the diabetic center. The mean age of the patients was 46.3 years, and the average HbA1C was 10.3, ranging from 9.5 to 12.6. Eight out of the 15 patients suffered from diabetic complications, such as neuropathy (1), diabetic foot (3), and retinopathy (4), and the majority of patients suffered from hypertension as a comorbid disease (73%). Most patients were on oral antihyperglycemic agents (i.e., metformin, sitagliptin, and gliclazide) and insulin injections (80%). Table 1 depicted further details of the demographic characteristics of the patients.
Demographic description of the participants (n = 15).
The themes that might impact antidiabetic medication adherence were identified from interviewing patients based on the SDoH domains, as shown in Table 2 and Figure 1.
Themes for T2DM medication adherence based on the social determinants of health domain.

Author Declaration form—human research and in vitro studies.
Education access and quality: Two main themes that emerged under this domain are Health Perception and Health Behavior.
Health perception demonstrates the patient’s belief and understanding of their health condition. The majority of patients in this study revealed a lack of knowledge regarding the nature of T2DM and the cause of the disease: Only I know it is a disease that works in silence, so you need to protect yourself before it hurts you without knowing. P2 I got diagnosed 7 years ago, but I didn’t know what it is {diabetes}; only I knew it gets high and low. P5
A few patients showed sufficient knowledge about T2DM and its potential causes: It is a pancreatic failure, where it stops the secretion of insulin. P4
However, almost all participants were aware of the symptoms of hypo and hyperglycemia. The patients mentioned several symptoms, such as dry mouth, tiredness, sweating, tremors, and blurred vision: If the blood sugar decreases, I know that when my body shakes, my heartbeat increases, and I start sweating, whereas it increases when I frequently go to the bathroom and my vision gets blurred. P15
Similarly, the patients demonstrated sufficient knowledge regarding the potential complications of DM: Many complications {include} kidney failure, cardiovascular disease, and sight problems. P4 I know it might cause kidney failure and blindness. P9
Health behavior: This refers to the patient’s attitudes and actions that might impact their health and adherence to antidiabetic medications. Several factors related to the patients emerged that might negatively or positively impact adherence to diabetic medications. For example, education about DM, traveling, religion (fasting), exercising, physiological factors, and eating habits.
Some patients believed that being uneducated might negatively affect their adherence to medications: I am an educated teacher, so I try to take my medications on time; however, my sister is uneducated. She did not take her medications regularly and stayed 2 to 3 days without injections because she did not know about diabetic complications, P4.
Some patients also mentioned that traveling and attending special occasions might be a barrier to taking medications on time (intentional nonadherence): Sometimes, the time for my medications comes while I am on the airplane, and my medication is in the bag, so I do not take it. P3 Last week I went to a dinner at my neighbor’s, as it was her daughter’s wedding, I did not take my injection before the dinner. . . {Why} The people would start talking and asking, and I did not want anyone to know I had diabetes. P1.
However, some patients believe fasting helps them adhere better to their diabetic medications. Fasting during Ramadan helps them schedule the time to take medications with Iftar and Suhoor: The best time to control my blood sugar I took my pills at sunset on one date; I mean with Iftar, and again with Suhoor, I took another injection. P10
Other patients believed that diet, regular exercise, and diabetic medications were essential to control blood sugar: My blood sugar was 13, and I worked on myself for 4 months, and it dropped. . . {How} I started a diet; I ate brown bread, boiled eggs, and vegetables; I derived myself from many things, I took my medications regularly, and I walked for 40 min to 1 h during weekdays and weekends. P14
Physiological factors, such as fear of the long-term complications of diabetes and hypo or hyperglycemia symptoms, sought to impact medication adherence among patients positively: It is better to know the complications and symptoms of diabetes once you have been diagnosed to take the medications regularly. P5 Sometimes, I decide not to take my medications, and once I start sweating, I panic and take them. P2
Healthcare access and quality: This study identified four themes: medication belief, polypharmacy, medication-related problems, accessibility to healthcare services, and patient and healthcare–provider relationships.
Medication belief: The patients expressed diverse opinions regarding the efficacy of antidiabetic medications. Some patients were aware of their effectiveness in controlling their blood sugar: My medications help me maintain the balance of sugar levels in my body. P5
However, some patients believed that the other approaches to diabetic management were better than the medications themselves in controlling their blood sugar: The best treatment for diabetes is diet. . . {what about the diabetic medications} . . . It improves slightly, but exercise and avoiding soft drinks, whole sugars, and white toxins are more effective. P2
Polypharmacy and medication-related problems: The appropriate use of medications was an essential factor that may impact patients’ adherence. While the patients emphasized the importance of taking their diabetic medications, they mentioned several factors that might have affected their adherence, such as taking multiple medications (polypharmacy): I had three different medications for diabetes for 4 years, and 3 months ago, I started taking insulin injections. And I had to use my antidepression medications, so I could not take this and this, and sometimes I got tired and confused and stopped taking it. P8. I just felt bored taking too many medications multiple times every day, So I missed some days without taking them. P5
Medication-related problems, such as side effects, might impact medication adherence; the majority of the patients mentioned the potential side effects of medications, such as heartburn, hypoglycemia, and skin pigmentation, as a barrier to taking medication: I used to use two pills of Glucophage and Jardiance, but the Glucophage caused me heartburn and nausea, so sometimes I take one pill or don’t take it. P 14 I was suddenly diagnosed with diabetes during Ramadan 7 years ago; since then, I have used the insulin pen injection. Now, I have black skin pigmentation and scars in several places. I went to the dermatologist, who said it was because of the injection; this is annoying, and I try to avoid it. P9
Accessibility to healthcare services: Having easy access to healthcare services, clinic appointment booking services, and multiple prescribers were identified as potential barriers that might directly or indirectly impact medication adherence.
Two patients expressed difficulty accessing healthcare facilities and services because they live in remote areas: I had a time when I didn’t have any medications left, so I did not take them for 2 days. . . I lived out of town; it is a 4-h drive; you know it is hard. P3
In addition, some patients complained about waiting times for clinical appointments with their healthcare providers and inadequate follow-ups : My medications are not helping; the last blood tests showed that my blood sugar was not controlled. . . {did you take them regularly} . . . no, I had a problem, but nobody cared. I called them, but I was given a 6-month appointment. P6
However, most patients reported no concerns regarding multiple prescribers as they saw the same doctors every time they had an appointment. I saw the same physician every time; he knew me and my medications. P10
Patient–healthcare providers relationship
The care of diabetic patients is always facilitated by a multidisciplinary diabetes team that includes a physician, a diabetes nurse educator, a dietitian, and a pharmacist. The effective relationship and communication between the patients and their healthcare providers were described by most of the participants: I saw the same physician every time I went to the clinics, and he explained to me the benefits and harms of each medicine and gave me enough information. P7 Once I got the diabetic diagnosis and started taking the diabetic medications, they transferred me to a health education clinic, where they explained everything and gave me advice. P4
A few patients described how the pharmacists participated in their diabetic medication management by educating and counseling them about their medications: Pharmacists always explained the medications to me, the time to take the medications, and if my blood sugar increases, I have to increase five units of my insulin dose; instead of 20, I take 25. He told me to do that. P3
However, most patients mentioned having no communication with pharmacists; they see their role in diabetic management as limited to dispensing medications and writing instructions on them: They just handed me the medications after writing on the box how many times I had to take them. . . {They did not counsel you} . . . sometimes. P5
Economic stability: Financial constraints
The cost of medications might impact medication adherence; however, all the participating patients mentioned no financial concerns related to the medication or the healthcare services: I did not find difficulty in getting the medications; everything is free and provided by the Ministry of Health. P1 My insulin, “the orange pen,” was unavailable in the center 3 months ago. I got it from the pharmacy store outside the center, and I did not pay any Riyals; the Ministry of Health could afford that. P10
Social and community context
Two themes emerged under this domain that might impact adherence to diabetic medications: family support and social stigma.
Family support
The findings of this study highlighted that patients’ families might play an essential role in their disease management and medication adherence. Almost all the patients mentioned that family support was essential to provide emotional and practical support: My wife made specific meals for me; other than the meals she tried to make for me a healthy food. P4 My daughter always helps me when I forget the insulin dose; she counts the dose in the pen injection and gives me the pills if I forget to take them. P11
Social stigma
Being stigmatized by other people was found to be one of the potential barriers to medication adherence: a few of the patients described not taking their medications in front of other people because of the fear of being known for their disease: How people look at you is important; honestly, I did not take my medication, especially the insulin injection, unless I returned home or went to the bathroom and took it. P10
However, most patients had not expressed any pressure or fear of taking their medication in public. They believed that diabetes had become the sickness of the century, and both older and younger populations suffered from it: Diabetes is widespread in our family. It is no longer a guest. We are 10 brothers, and all of us have diabetes. I told my friends that if I go out with them, they follow up with me on what I ate and drank and whether I took my medication. P3
Others—suggestions for improving adherence
Patients were asked what helped them to take their medication or improve medication adherence. Patients mentioned several approaches and tools, such as alarms and dispenser boxes: I used an alarm, especially for night injections. P4
Patients were also asked about their perception of using mobile applications to aid their medication use. Most patients agreed that this would be a potential solution for younger and more educated patients: I heard about such applications, but I did not use them. It is more for educated and younger patients. P7
However, some of the patients mentioned that older patients could use the mobile application if they receive assistance from their families: I would not mind using programs or applications to remind me of my medicines; I would need my daughter’s help. P3
Discussion
This is the first study to explore in detail the experiences and barriers to medication adherence among individuals in Jazan, Saudi Arabia, who have uncontrolled T2DM. Chatterjee and Davies have stated that a proper medication regimen is essential to control DM, and medication adherence is crucial to ensuring treatment success. 15 However, medication nonadherence is a common issue when it comes to managing chronic diseases. 16 This study aimed to identify the potential barriers to antidiabetic medications beyond individual barriers to other economic and environmental factors. Indeed, several previous studies highlighted the impact of socioeconomic factors on adherence to medications.8,9,16,17
The findings of this study provide insights into other factors that might impact adherence directly or indirectly; these were grouped into four domains based on SDoH 13 : education access and quality, healthcare access and quality, economic stability, and social and community context. This indicates that factors contributing to medication nonadherence are not restricted to patient-related causes but encompass a wide range of external factors.
The findings indicate that education or knowledge about T2DM might significantly impact medication adherence. Many patients were not aware of the disease’s nature or cause, which can lead to poor medication adherence. Ignorance of the implications of the disease and the role of medication in its management can also lead to poor treatment adherence. 18 Limited knowledge about their health conditions may hinder patients from understanding the importance of taking medication as prescribed and adhering to it. This aligns with earlier studies, suggesting that enhancing patients’ understanding of T2DM can significantly improve their medication adherence.19,20 Therefore, healthcare providers (HCPs) must prioritize patient education to comprehend the disease process thoroughly, the significance of consistent medication intake, and the potential consequences of nonadherence. Ampofo et al. 21 reported that regular verbal educational interventions by HCPs can boost patient engagement and involvement and improve medication literacy and adherence.
Consistent with previous studies that assessed the relationship between medication adherence and health behaviors,8,9,16,17 our finding highlighted that the patient’s behaviors and actions, including traveling, religion, and eating habits, might impact medication adherence.16,17,22 These factors might relate to intentional nonadherence, such as the denial about the seriousness of diabetes, eating healthy food, and practicing physical activities. The belief that “everyone’s got it” or “eating unhealthy food” most commonly are patients’ decisions to not adhere to medication regimens. Therefore, a holistic approach to patient care that considers these factors is essential in promoting medication adherence and, thereby, more effective management of T2DM.23,24 The patients in this study reported positive impacts of the holy month of Ramadan on their attitude toward establishing routines that facilitated medication adherence. On the contrary, a previous study conducted in another region in Saudi Arabia reported that religious factors, such as fasting in Ramadan, negatively impacted medication adherence among T2DM patients, as they used to forget to take medication. 4 Given that this study did not assess any direct association between religious factors and medication adherence, future studies must focus more on how these factors might impact adherence among T2DM.
The healthcare access and quality domain incorporated multilevel factors that might impact medication adherence. These factors include patient-level factors, such as polypharmacy and medication-related problems (e.g., side effects of medications), and patients’ belief in the efficacy of medications. This is consistent with previous studies showing that patients’ perceptions of medication’s side effects and effectiveness can significantly impact adherence. 25 Kassahun et al. 25 found that patients who experienced medication side effects were less likely to adhere to their treatment. 26 Another study reported a significant association between lower medication adherence and hypertensive patients who experienced medication-related side effects. 27 Similar to the previous study, the belief about the medication’s efficacy in reducing blood glucose was also raised in this study. 17 Others were the frequency of daily doses and taking multiple medications (polypharmacy), which were shown to be a potential barrier to medication adherence. A systematic review reported that polypharmacy poses many challenges to patients that impact their quality of life and medication adherence negatively. 28 However, a US study found that polypharmacy alone does not lead to reduced medication adherence. Instead, patients with suboptimal adherence tend to have problems with one specific medicine, either because of unreported side effects or because the patient feels that the medication is not of value to current or future health. 29 Moreover, a previous study reported that patients with stroke who took less frequent doses or medications were more likely to adhere to their medications. Therefore, healthcare providers should simplify antidiabetic medication regimens whenever possible.
Regarding the interpersonal level factor, this study highlighted that the relationship and effective communication between the patients and their healthcare providers might play a vital role in medication adherence. Regular contact with healthcare professionals can enhance understanding of the disease and its management and foster a sense of support and reassurance, leading to better medication adherence. This finding aligns with previous studies demonstrating the positive impact of good patient–provider communication on medication adherence,30,31 underscoring the positive influence of good patient–provider communication on treatment adherence. As posited by Young et al., 31 healthcare providers can enhance medication adherence and patient outcomes in conditions like asthma by employing communication strategies designed to build patient trust and motivation. 30 Another study highlighted the importance of creating a relationship between healthcare providers and patients with hypertension to facilitate effective communication and improve the patient’s confidence in healthcare, which leads to improved health literacy and adherence. 32 However, healthcare providers’ lack of collaboration, lack of interest in the patient’s life and context, poor communication, or time constraints during consultation were previously reported by patients with T2DM that might interfered with their interest in adhering to their medications. 10 This suggests that fostering a strong patient–provider relationship could be a powerful tool in enhancing medication adherence across various chronic diseases, including T2DM.
In addition, organizational-level factors, such as accessibility to healthcare and long clinic appointments, were described as potential barriers to medication adherence. However, previous studies showed that telemedicine and medication delivery programs could solve these logistical challenges and significantly improve patient medication adherence.33,34 Indeed, virtual diabetic clinics have been implemented during the COVID-19 lockdown in Saudi Arabia alongside several services, such as postal delivery of medications, which have shown a significant positive impact on glycemic control among T2DM. 35 Virtual clinics have become a part of patient care services in Saudi Arabia to enhance the provided healthcare services and promote long-term behavioral adherence among patients.
Contrary to previous studies, this study found that the cost related to the medications or healthcare services was not a significant concern for T2DM.9,16,17 A possible explanation is that the Saudi government’s health policies cover the cost of all health-related services for Saudi citizens. However, cost-related nonadherence could influence non-Saudi T2DM patients; therefore, further investigations are needed to assess the financial burden for non-Saudi diabetic patients and their impact on medication adherence.
Healthy People 2030 initiative reported that relationships with family, friends, or community members would positively impact patients’ health and well-being. 13 In the current study, family support and social stigma were identified as significant social factors affecting medication adherence. Previous studies have highlighted that having a robust social support system was an essential factor in their ability to stick to their treatment plans and manage their illness effectively. They found that receiving emotional and practical support from family, friends, and healthcare professionals helped them to feel more motivated, less isolated, and better equipped to deal with the challenges that came with their illness.36,37 This realization highlighted the importance of encouraging patients to seek social support as a part of their overall management plans. The social stigma surrounding the diagnosis of T2DM can indeed have a significant impact on medication adherence, as revealed in a Kuwaiti study. 9 This stigma can manifest in various ways, such as dread of being labeled as “sick,” fear of social exclusion, or the burden of coping with a chronic illness considered an important community-level factor that impacts medication-taking behavior. This social stigma can lead to denial, concealment, or avoidance of the disease, subsequently affecting a patient’s willingness to adhere to their medication regimen.38,39
Moreover, previous studies reported that diabetic patients usually describe feelings of fear, blame, and embarrassment that sometimes lead to depression.16,40 Therefore, it is essential to underscore the importance of addressing the societal perceptions and stigma of T2DM in healthcare approaches. It also highlights the need for supportive environments that encourage acceptance and understanding of this chronic condition and promote better disease management and medication adherence. Indeed, the social and community context must be incorporated into patients’ routines in managing their antidiabetic medications. Patients should have the courage to talk about their health conditions, and family members have to be involved in the care of patients to improve medication adherence. Healthcare providers should counsel family members and involve them in the patient’s care plan, as well as enlighten the public and share information about T2DM.
Lastly, approaches and tools to enhance medication adherence, such as reminders and pillboxes, were mentioned, and possible strategies and approaches that might assist patients in becoming adherent to medication, especially younger patients, were also suggested. Indeed, several previous studies reported the interest of patients in using mobile phone applications to aid medication adherence among patients with chronic disease.41,42 However, further research is needed to determine the value and acceptance of mobile phone applications among T2DM patients to enhance medication adherence.
Strengths and limitations
All participants interviewed in this study represented a broad spectrum of the patient population with T2DM in the Jazan region in terms of the level of education and number of years of taking medications. Thus, the findings of this study provided a meaningful insight into the complexity of factors that might hinder medication adherence among patients with T2DM. However, this study is not without its limitations. First, as participants were recruited from a single center in the Jazan region, their perspectives might not be generalizable. Second, selection bias might have occurred as the patients who came to their follow-up appointments were invited and recruited to participate in the study; patients who did not attend their follow-up appointments might have other perspectives regarding the barriers to medication adherence. Even though the method used in this study was the best to explore the reason for nonadherence and the associated factors among T2DM patients, the social desirability and recall bias might have impacted the quality of the collected data. Even though most patients had co-morbidities (n = 11), this was not mentioned as a potential barrier to medication adherence. One explanation could be that the patients are in sample medication regimens, and the patients formed their routines and experiences to comply with these health issues. Similarly, other potential barriers (e.g., cognitive or mental impairment and cost) were not raised by the patients; this could be because this study included younger patients (mean age was 46 years old) and Saudi citizens. Therefore, further studies are needed to comprehensively understand all potential factors influencing medication adherence in various populations. Finally, all interviews were conducted by the same researchers with experience and training in conducting qualitative interviews to reduce the impact of researcher bias.
Conclusion
SDoH factors, such as education, health perceptions, healthcare quality and accessibility, and social support, can significantly influence patients’ ability and willingness to adhere to their antidiabetic medications. To promote medication adherence among T2DM patients, multilevel interventions and approaches are needed to target the patients, healthcare system, and community. This approach should include educating the patient to enhance disease understanding and medication adherence, personalized care plans that consider each patient’s unique lifestyle and needs, simplified medication regimens to reduce the burden of polypharmacy, effective communication between healthcare providers and patients to foster trust and understanding, and strong social support to mitigate the effects of stigma and provide encouragement in disease management. Such a holistic approach could significantly improve the quality of life and health outcomes for individuals living with T2DM. The intervention focused on utilizing digital health technology, which could improve medication adherence.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121241271820 – Supplemental material for Exploring patient’s perspective of barriers to diabetic medication adherence in Jazan, Saudi Arabia, using the social determinants of health model
Supplemental material, sj-pdf-1-smo-10.1177_20503121241271820 for Exploring patient’s perspective of barriers to diabetic medication adherence in Jazan, Saudi Arabia, using the social determinants of health model by Amani Khardali, Alanood Aladwani, Fahad Alzahrani, Osama A Madkhali, Saad Al Qahtani, Marwa Qadri, Morghma Deffeallah Adawi and Mohammed Hakamy in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank all patients who provided valuable insights for the study.
Author contribution
AK contributed to the conception of the study. AK, AA, FA, OAM, SA, and MQ designed the study. AK, AA, MH, and MDA contributed to the acquisition of the data. All authors contributed to the analysis and interpretation of data. AK and FA drafted the manuscript. All authors revised the manuscript critically for important intellectual content and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors extend their appreciation to the Deputyship for Research and Innovation, Ministry of Education in Saudi Arabia, for funding this research work through project number ISP23-72.
Ethical considerations
The study was approved by the Jazan Health Ethics Committee, Ministry of Health Affairs, Jazan Province, Saudi Arabia (Approval Reference No. 2304). Informed consent was obtained from participating patients in this study.
Informed consent
Signed and written informed consent was obtained from each patient before data collection. For illiterate patients, the study’s purpose and items of the informed consent were verbally explained to them. Upon their approval, they were asked to sign and date the consent form. After obtaining informed consent from the patients, the patients’ right to withdraw or refuse to answer a few or all the questions was also respected.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.