
Abstract
This scoping review aimed to explore the water, sanitation, and hygiene status in Zimbabwe and its influence on health outcomes. A systematic search of the literature published in English with an unrestricted search until 31 May 2024 was performed using predefined search strings with Boolean operators, including PubMed, EBSCO, SAGE, SpringerLink, Cochrane Library, ScienceDirect, Scopus, and Web of Science databases. A total of 655 records were identified, of which 20 peer-reviewed articles and 10 other records met the inclusion criteria. The inter-rater agreement for 20% of the dual screening achieved a κ-value of 0.85, indicating almost perfect agreement. Lack of access to adequate clean water, inadequate WASH infrastructure, and unhygienic conditions and practices are among the primary risk factors for diarrhoeal diseases and their associated outbreaks, as identified in several studies. These factors have been reported to play a significant role in recurrent outbreaks of cholera, typhoid, and diarrhoea in Zimbabwe. The lack of adequate WASH facilities in rural schools significantly impacts the management of menstrual hygiene waste. The review concludes that poor Water, Sanitation and Hygiene (WASH) has led to an array of adverse public health outcomes in Zimbabwe over the decades. Despite the existence of a comprehensive WASH policy framework, weak implementation, inadequate funding, poor governance and community participation, and unreliable WASH data monitoring systems largely contribute to the water and sanitation disease burden. Therefore, this review recommends investing in the Rural Water Information Management System (RWIMS) and other digital platforms to improve monitoring and surveillance. Achieving the desired health outcomes requires a fundamental shift in community knowledge, attitudes, and practice. Hence, this review recommends strong community capacity building to support community-led WASH initiatives. The review further recommends strengthening the whole-of-government approach to achieve universal access to WASH in Zimbabwe.
Strengths and Limitations of the Study
✓ The scoping study included a broader variety of databases with a comprehensiveness rate of 96% or higher in the literature search, with the intention of maintaining a larger coverage.
✓ To examine the influence of WASH status on the health outcomes of various populations in Zimbabwe.
✓ This review focuses solely on research presenting findings on this topic of interest in Zimbabwe, perhaps limiting the generalisability of the study to different settings.
Introduction
Universal access to clean water, sanitation, and hygiene is a fundamental human right, as stated in the Sixth Sustainable Development Goal of the United Nations by 2030. 1 However, countries must overcome significant challenges to improve their health outcomes.2,3 This scoping review explored the water, sanitation, and hygiene (WAin SH) status and its influence on health outcomes in Zimbabwe. WASH collectively refers to water, sanitation, and hygiene, 1 which are critical components for preventing communicable diseases linked to contaminated drinking water, inadequate sanitation, and poor hygiene2,3 practices habits. Ensuring adequate access to safe water, proper sanitation facilities, and good hygiene behaviours directly reduces disease transmission and improves overall health outcomes.1,4
In 2022, millions of people worldwide 5 faced critical challenges accessing safe water, sanitation, and hygiene. During the same period, over 2 billion people 5 lacked safely managed drinking water. Approximately 3.5 billion people 5 lack access to safely managed sanitation facilities, and among this group, 419 million people 5 still practise open defecation in 2022. Basic hygiene services were unavailable to 2 billion people, 5 and 653 million 5 had no hygiene facilities at all by 2022. Furthermore, 1.8 billion people 5 collect drinking water from sources outside their homes, and in approximately two-thirds 5 of these households, women are primarily responsible for collecting water. The number of people in the rural community without access to proper sanitation declined from 2.2 to 1.9 billion between 2015 and 2022. However, population growth and persistent WASH inequalities have kept the global population lacking adequate sanitation relatively constant at around 1.6 billion people during the same period. Globally, billions of vulnerable populations still lack access to basic WASH facilities and services, particularly in rural areas and developing countries.2,6 The absence of basic services presents serious obstacles to optimal wellness, human population growth, and development. Progress must increase fourfold to achieve universal access by 2030, in line with Sustainable Development Goal 6, which aims to ensure the availability and sustainable management of clean water, proper sanitation, and hygiene.6,7
Poverty, climate change, and limited financing are major drivers of WASH challenges, 2 resulting in diseases such as typhoid, cholera, bloody diarrhoea, acute diarrhoeal illnesses, malnutrition, and neglected tropical diseases, including intestinal worms, bilharzia, and trachoma across Africa.2,7 These conditions contribute to millions of deaths and loss of millions of disability-adjusted life years (DALYs) each year, particularly in low- and middle-income countries (LMICs). 7 WASH-related illnesses can decrease productivity and impose significant economic burdens on households and communities, highlighting the need for sustainable water, sanitation, and hygiene interventions. 8 To address these challenges and ensure equitable, lasting improvements in WASH programmes, governments and stakeholders must sustain investments in infrastructure, enact legislative reforms, and actively engage communities. 9 Zimbabwe is one of several African nations fighting to reduce the morbidity and mortality associated with waterborne and water-related illnesses. 10 In pursuit of the transformative 2030 Agenda for Sustainable Development, like many other nations, Zimbabwe faces the pressing challenge of achieving Sustainable Development Goal 6 (SDG 6) to ensure access to clean water and sanitation. 11 Despite ongoing efforts by the government and stakeholders, the country continues to face significant challenges in WASH. 12 Zimbabwe had a total population of approximately 15.2 million, 13 of whom 61% (9.26 million) 13 resided in rural areas and 39% (5.92 million) 13 in urban areas. Nationally, only 34.6% 13 of the population has access to at least basic sanitation services, falling significantly short of the Sustainable Development Goal (SDG) 6 target of universal access to adequate and equitable sanitation by 2030. 5 There are significant disparities between urban and rural areas, with 56% 13 of the urban population having access to basic sanitation compared to only 36% in rural areas. 13
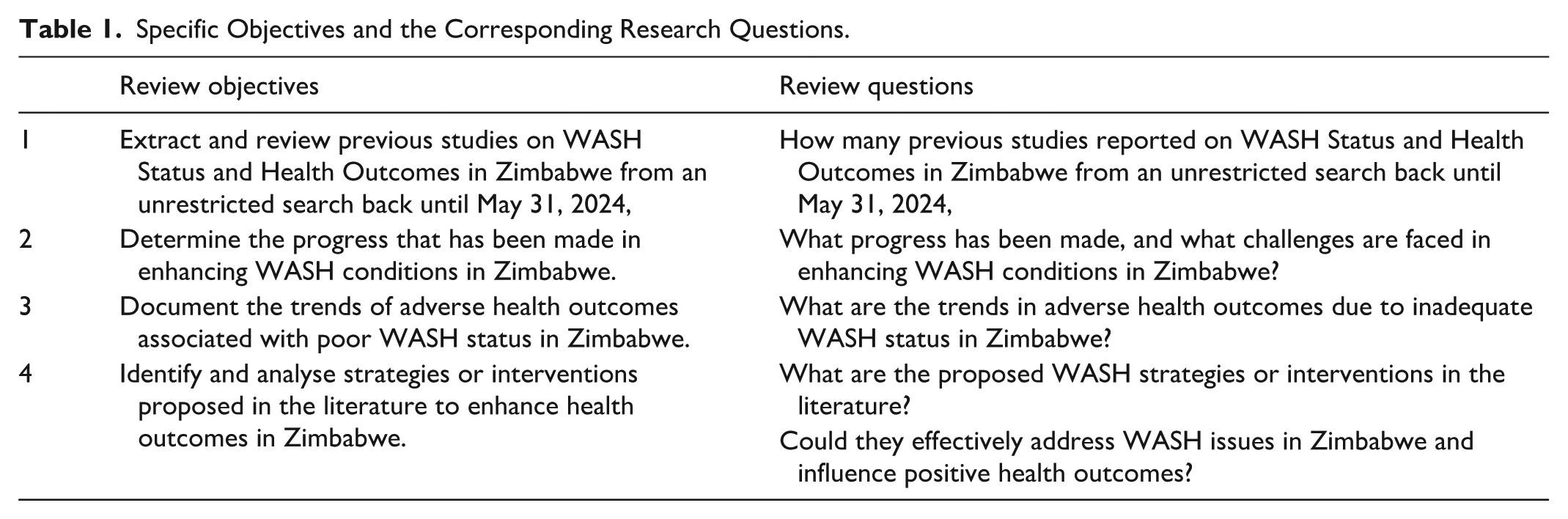
In 2022, the country had an estimated 3.82 million households, 13 comprising 2.80 million in rural areas and 1.02 million in urban areas. 13 More than 30% 13 of rural households rely on unimproved drinking water sources, indicating slow progress towards achieving universal access to safe and affordable drinking water (SDG 6.1).5,11 Furthermore, 67.4% of rural households 13 reported travelling 30 min or more to collect water, compared with 23.6% of urban households, 13 highlighting the persistent burden of water collection in rural settings. Access to handwashing facilities also remained low, with only 26.8% of rural households 13 having facilities with soap and water compared to 73.2% in urban areas. 13 Poverty remains a major factor, as limited financial resources hinder access to WASH in rural areas. 14 This scoping review examined the current state of Water, Sanitation, and Hygiene (WASH) and its impact on health outcomes in Zimbabwe. Aligned with its main objective, the review seeks to answer the overarching research question: “What is the impact of WASH status on health outcomes in Zimbabwe?” and utilises existing literature to address specific objectives and corresponding review questions, as detailed in Table 1.
Specific Objectives and the Corresponding Research Questions.
Methods
Protocol Registration
The protocol for this scoping review was registered in BMJ Open (https://doi.org/10.1136/bmjopen-2023-082224) with an online issue publication on 19 August 2024. This protocol is available as an open-access article under the Creative Commons Attribution Non-Commercial (CC BY-NC 4.0) Licence.
Study Setting
Zimbabwe is a landlocked country located in south-central Africa, covering an area of 390,757 square kilometres (150 872 square miles). The country lies between the Zambezi and Limpopo Rivers, with the Zambezi River forming its northern border with Zambia and the Limpopo River marking its southern boundary with South Africa. 15 Zimbabwe shares a border with Mozambique to the east and Botswana to the west.16,17 The country lies between -19.015438° south latitude and 29.154857° east longitude 15 and is entirely north of the Tropic of Capricorn.
Zimbabwe has three broad climatic regions: The Central Plateau, which covers most of the country and generally has a temperate climate. In contrast, low-lying areas, such as the Zambezi Valley, are warmer and drier, with hot summers. 18 The Eastern Highlands are cooler, with significantly higher year-round rainfall.18,19 However, the country experiences largely subtropical climatic conditions, characterised by a single rainy season that occurs from November to March. 18 Rainfall becomes less reliable when moving from north to south and from east to west, 15 contributing to water scarcity that affects the WASH status and health outcomes in the country. The period from August to October is typically hot and dry. Only 37% of the country receives adequate rainfall for agriculture.18,20 The largest inland water body, Lake Kariba, lies along the Zambia-Zimbabwe border. The major rivers in Zimbabwe are the Zambezi, Limpopo, Sabi, and Runde. The country’s topographical features include the central watershed, which stretches from southwest to northeast, with elevations ranging from 1200 to 1500 m above sea level.15,16
Zimbabwe is divided into 10 administrative provinces 17 : Bulawayo, Harare, Manicaland, Mashonaland Central, Mashonaland East, Mashonaland West, Masvingo, Matabeleland North, Matabeleland South, and Midlands.13,16 Harare, the capital city, serves as the main hub for administrative and commercial activities (Figure 1).13,18,19 Zimbabwe’s population is estimated at approximately 15.8 million,13,16 and the country is among several African countries working to reduce the burden of waterborne and water-related diseases. 10

Figure showing the study boundaries.
Study Design
A scoping review was employed because its methodology adheres to a pragmatic research perspective, highlighting the relevance of feasible and flexible approaches to meet the study objectives. 21 This review is ideal because it is time-efficient and successfully answers the study questions. The scoping review methodically investigates key findings from previous studies and literature gaps relevant to a particular subject. 22 In contrast to other types of reviews, this review is not limited to certain study designs, allowing for the incorporation of diverse results from qualitative and quantitative studies and policy documents. 22 This wide approach provides a solid understanding of Zimbabwe’s WASH status and health outcomes (Table 1).
Data and Information Sources
In this review, records that satisfied the inclusion and exclusion criteria were sourced from the main databases (Table 2), including PubMed, SAGE, SpringerLink, Cochrane Library, ScienceDirect, Nature, Scopus, EBSCO, and Web of Science, and an unrestricted search for English-language publications was conducted until 31 May 2024. The chosen databases are reliable and span many fields, guaranteeing a variety of excellent sources and a thorough comprehension of Zimbabwe’s WASH situation and health achievements. Particular incidents, policy modifications, or environmental, socioeconomic, and political elements that may have previously occurred and impacted WASH status and health outcomes in Zimbabwe should be considered.
Inclusion and Exclusion Criteria.

Search Strategy
The search strategy for the review focussed on 3 key constructs: (i) WASH status, (ii) health outcomes related to WASH, and (iii) WASH interventions. Boolean operators (AND, OR) were applied systematically, with parentheses used to structure the search terms to ensure logical consistency. This approach allowed for the combination of multiple related terms within each construct while making “Zimbabwe” a mandatory term across all searches, as follows:
("Water, Sanitation, and Hygiene" OR "WASH" OR "Sanitation services" OR "Sanitation facilities" OR "WASH Infrastructure" OR "Water treatment" OR "Toilet facilities" OR "Sewage disposal" OR "Open defecation") AND ("Health inequalities" OR "Health disparities" OR "Health determinants") AND ("Hygiene-related diseases" OR "Sanitation-related diseases" OR "Water-borne diseases") AND ("Hygiene practices" OR "Handwashing" OR "Personal hygiene") AND ("Behaviour change" OR "Interventions" OR "WASH programs" OR "WASH initiatives" OR "Policy measures") AND ("Health impacts" OR "Population health" OR "Child health" OR "Maternal health") AND ("Household health") AND ("Health Outcomes" OR "Health effects" OR "Health impacts" OR "Public health") AND (Zimbabwe).
Minor syntax adjustments were made for individual databases, such as PubMed, Scopus, and Web of Science, to accommodate differences in search functionalities while maintaining the core structure and conceptual integrity of the search strategy. In this comprehensive review, EndNote was used to efficiently organise, store, and cite references. 23 The titles and abstracts of publications retrieved from databases in response to search queries were loaded into Rayyan, a cloud-based platform designed to help reviewers collaborate more efficiently. This tool helps locate and organise appropriate sources for scoping reviews.24,25 The integration of these tools results in a more effective and coordinated scoping review process.
Screening Process
This study adopted a two-step screening process to identify relevant literature. This multistage approach is crucial because systematic searches often generate large volumes of potentially relevant studies. 22 In the initial phase, 2 independent reviewers screened the titles and abstracts of all articles retrieved through a systematic search. One reviewer screened all entries, whereas the other independently screened 20% of the records screened. Articles were included in the next stage if their titles and abstracts met the predefined inclusion criteria (Table 2). The second stage involved a thorough review of the full-text articles. This two-step process aligns with established methods for enhancing the rigour of literature reviews. This study used Cohen’s kappa coefficient for inter-rater reliability (IRR). A citation-mining approach was used to ensure comprehensive literature identification. The reference lists of the included studies were examined using EndNote and Rayyan to identify potentially relevant sources that may have been missed during the initial search. Backward and forward citation chaining was conducted for all included studies to identify any additional relevant literature.
Strategies for Enhancing Rigour
The assessment of study quality was based on the established Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension (PRISMA-ScR) criteria to ensure a comprehensive evaluation of the included studies. The results were analysed descriptively, and the review adhered to the PRISMA-ScR for the scoping review checklist, which guided the reporting process (using the main website: https://www.equator-network.org/).
Data Extraction
Data extraction is a vital prerequisite because it enables the analysis, summarisation, and interpretation of evidence.26,27 The PRISMA-ScR framework also guided the extraction of structured data in response to the identified variables from the specific review questions and objectives listed in Tables 1 and 2. These variables included information about the study context (including study population, design, and setting/location in Zimbabwe), WASH interventions from policy to activities, and all WASH-related health outcomes beyond diarrhoeal conditions/diseases.
Analysis and Synthesis
Given the limited number of previous studies and variations in interventions and health outcome measures, a meta-analysis was not feasible. Therefore, the results were analysed using a mixed-methods approach. The quantitative analysis focussed on identifying patterns, relationships, and trends between WASH-related variables and health outcomes in the extracted data. Qualitative analysis, guided by thematic analysis aligned with the research objectives and questions (Table 1), was used to further explore and interpret the findings. Data charting was employed to streamline the data synthesis and enhance accessibility for analysis and interpretation. Conclusions were drawn directly from the collected and analysed evidence, ensuring that they directly addressed the research objectives.
Results
General Characteristics
The studies included in this review spanned a range of methodologies, including spatial analysis, cross-sectional surveys, clinical trials, and qualitative studies, covering urban and rural settings. A total of 655 data searches were conducted for the papers, as shown in Figure 2. Of the identified articles, 20 peer-reviewed and 10 national policy/strategy/survey report documents met the inclusion criteria for this review. Backward and forward citation chaining was performed on all the included studies to identify any additional relevant literature. However, this process did not yield any studies that met the inclusion criteria. The inter-rater agreement for the 20% dual screening was κ = 0.85, indicating almost perfect agreement. A brief of the 10 policy documents and survey reports included in the review focussed on improving sanitation and hygiene practices, ensuring access to clean water and proper sanitation for all citizens, emphasising sustainable water management and access to clean water for everyone, and strategic government planning to reduce the disease burden, foster sustainable economic growth, and improve infrastructure and services.

PRISMA flow diagram showing steps followed to select articles.
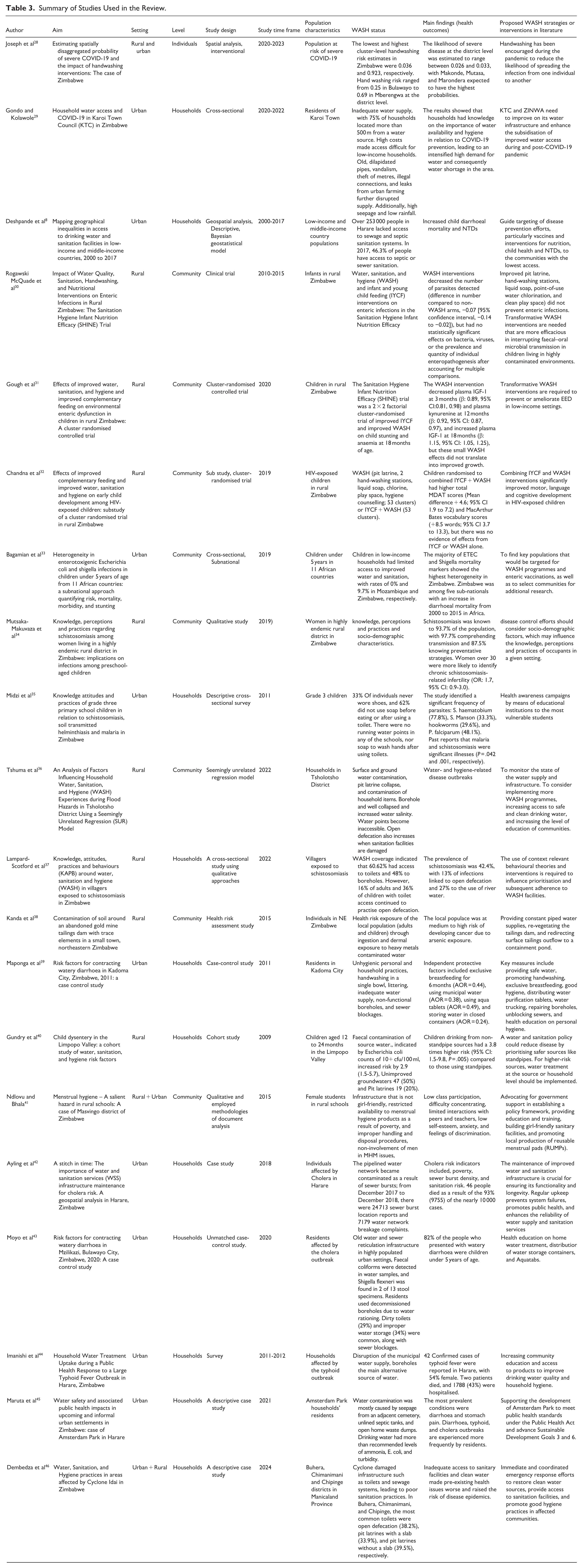
The distribution and focus of the studies revealed that out of 20 articles, the majority 16 of the studies were observational in nature, indicating a strong emphasis on understanding real-world contexts and behaviours related to WASH interventions and their health impacts (Table 3). The distribution of these articles in the context of rural and urban settings revealed that they were equally represented, and this balanced approach allowed for a comprehensive understanding of how WASH conditions and health outcomes differ across environments. The distribution of the articles showed that 11 studies were conducted at the household level, 8 at the community level, and 1 at the individual level, contributing to valuable information that could inform targeted interventions aimed at improving WASH status and health outcomes (Table 3).
Summary of Studies Used in the Review.
Water, Sanitation, and Hygiene Status in Zimbabwe
Inadequate WASH Infrastructure and Limited Services
WASH infrastructure and services in Zimbabwe encounter considerable obstacles.8,29,36,42,43,45,47 While numerous rural communities continue to depend on unsafe practices such as open defaecation, 29 a previous study conducted in the Masvingo district revealed that the upkeep of Blair Ventilated Improved Pit Latrines (BVIPs) is inadequate, highlighting that even when toilets are available, inadequate maintenance can result in unsafe waste management and associated health hazards for households that utilise them. 41 In urban areas, residents often lack access to adequate sanitation and solid waste services because of ageing and deteriorating sewer infrastructure. Factors such as vandalism, metre theft, illegal connections, leaks, and pressure from urban agriculture further compromise water supply and sanitation delivery.8,29,37,39,43 Zimbabwe’s National Health Strategy (2021-2025) highlights that the availability of safe water and sanitation facilities remains a huge challenge in the country. Despite these persistent challenges, the Zimbabwe National Sanitation and Hygiene Policy emphasises the need to provide sufficient and sustainable WASH facilities nationwide. This policy framework aims to address infrastructure gaps, promote hygiene practices and sanitation services to enhance public health and achieve national and global sustainable development goals.
Water, Sanitation, and Hygiene (WASH) Intervention Inequities
Gender-sensitive WASH interventions remain a significant challenge, particularly in rural areas.8,32 -35,37,41,43 Additionally, several records shown in the WASH equity framework (Table 4) further revealed that rural areas and low-income households had limited access to improved water and sanitation.29,33,35,37,46 The lack of basic WASH infrastructure that accommodates girls’ needs has emerged as a critical issue, especially in schools. Facilities frequently lack functional locks, sufficient lighting, and menstrual hygiene support, including inadequate access to water, disposal options, and hygiene materials. These gaps expose girls to health risks, safety and privacy concerns, and discomfort, contributing to increased absenteeism and negatively impacting their overall well-being and school performance.37,41 A previous study conducted in Shamva District in Mashonaland Central Province and Mutare District in Manicaland Province highlighted that the lack of adequate facilities contributed to poor hygiene practices among students, with 62% not using soap before eating or after using the toilet. 35 However, school WASH programmes are critical for promoting health and hygiene among children.35,37,41 Inclusive policies that address the specific needs of vulnerable populations are critical for improving WASH outcomes. 36
Water, Sanitation and Hygiene (WASH) Equity Framework in Zimbabwe.

Inadequate WASH Knowledge and Unsanitary Practices
Unsanitary practices at both the personal and household levels, including handwashing in a single basin, littering, and open defaecation, are prevalent issues.37,39,40,43 Faecal contamination of source water was evidenced by Escherichia coli counts exceeding 10 CFU/100 ml. 40 Hygiene promotion was essential for improving health outcomes, yet many communities lacked effective education on hygiene practices. A previous study indicated that individuals did not adhere to hygienic practices because of cultural beliefs and a lack of facilities. 39 Several studies have indicated a significant gap in community knowledge of WASH practices, particularly regarding schistosomiasis and other neglected tropical diseases.34,35,37 Research on women’s knowledge, attitudes, and practices regarding schistosomiasis has indicated that while awareness is high, misconceptions about transmission and prevention persist. The article highlighted that demographic factors influence women’s knowledge and practices, with uneducated women being more likely to be exposed to unsafe water sources. 34
Contaminated Drinking Water Sources
The studies revealed that water contamination was exacerbated by seepage from nearby cemeteries, unlined septic tanks, open waste dumps, open defaecation, and sewer bursts.29,42,45 Poor source water quality was evidenced by Escherichia coli counts exceeding 10 colony-forming units (CFU) per 100 ml. 40 In a previous study, the results showed that groundwater had higher concentrations of contaminants during the dry season than during the wet season because of trace elements near abandoned mines. 38 The geo-accumulation and contamination degree indices revealed significant to severe soil contamination by cadmium (Cd), chromium (Cr), and copper (Cu) within a 10-m radius of the tailings dam. The analysis showed that contamination was most pronounced near the dam, reflecting the immediate environmental impact at the site. 38
Adverse Effects of Climate Vulnerability
The impact of natural disasters such as Cyclone Idai, on Water, Sanitation, and Hygiene (WASH) services in Zimbabwe has underscored the vulnerability of communities to health risks associated with inadequate access to clean water and sanitation facilities. Water, Sanitation, and Hygiene (WASH) practices are frequently influenced by severe and recurrent natural disasters. The aftermath of Cyclone Idai resulted in widespread damage to water supply systems, leaving many communities without access to clean drinking water. Cyclones also cause extensive damage to sanitation infrastructure, including latrines and sewage systems. 46 Floods cause extensive damage to water supply systems, leading to shortages of clean water and an increased risk of contamination. 36 According to international standards, an contrast, low rainfall significantly strains WASH services, leading to water challenges, and compromised hygiene. 29
Governance and Financial Constraints
Effective governance and a robust policy framework are essential for the successful implementation of WASH programmes in Zimbabwe.29,53 While few studies provide an oblique reference to the Zimbabwe WASH policy in the context of Sustainable Development Goal Six (6) in Zimbabwe, the ongoing challenges within the Water, Sanitation, and Hygiene (WASH) sector suggest a weakened policy framework and its operationalisation. 53 A person is entitled to 50 L 29 of water from an improved source each day, according to international standards. Additionally, the Zimbabwe National Water Policy states that water for domestic use should be available in amounts of at least 25 L/day 29 for each individual. This means that a household should not spend more than 5% of its monthly income on water services. 29 However, the studies revealed that residents had become victims of the Zimbabwe National Water Authority (ZINWA), receiving exorbitant monthly water bills despite going weeks without tap water,29,53 which exposed governance constraints and financial mismanagement in the provision of water services. 29 Technology that can be utilised to enhance WASH services is still not widely funded in Zimbabwe.36,41 Limited funding for the Rural Water Information Management System (RWIMS) has weakened real-time data-driven water infrastructure and quality monitoring. 36 Some studies also recommended that the government commission review the current multi-stakeholder platform to align its governance structure with the 2013 national constitution and WASH policy framework. 53
Interventions should strike a balance between capital and operational spending while addressing key issues identified in the studies to reduce Non-Revenue Water (NRW). Capital expenditures (Capex), such as investing in the RWMIS, implementing transparent and subsidised smart metring billing systems, rehabilitating assets, and installing modern infrastructure with support from the government and private sector, can help reduce billing disputes and high-water costs. These investments provide long-term benefits.28,29,42 Operational expenditure (Opex) activities, including regular inspections of water supply and sanitation systems, prompt leak repairs, ongoing data analysis, and the use of Key Performance Indicators (KPIs), as well as quick responses to RWMIS failures and routine staff training, can lead to a more sustainable and fair water supply system. Furthermore, community involvement in reporting damage, marking underground pipes, prohibiting farming near water lines, and enforcing laws against vandalism are essential protective measures. Good management of Capex and Opex allows utilities to reinvest savings from reduced water losses, which improves the financial stability, reliability, and sustainability of the water system.28,29,42
Schools should adopt Standard Operating Procedures (SOPs) for menstrual hygiene-friendly WASH facilities. These procedures include providing private and secure toilets with locks and good lighting, a reliable water supply for washing and cleaning, and proper disposal methods, such as covered bins or incinerators, for menstrual waste. Schools should also provide access to hygiene materials and designated changing areas. These procedures highlight the need for regular maintenance and cleanliness. By implementing these SOPs, schools can create a safe, inclusive, and supportive learning environment that respects girls’ dignity while improving their attendance and academic performance.35,37,41
Discussion
This review collectively and consistently highlights the multifaceted relationship between unsafe Water, Sanitation, and Hygiene (WASH) and a range of adverse public health outcomes in Zimbabwe. The review indicates that poor infrastructure, rapid urbanisation, climate change, 36 environmental stress, cultural barriers, inadequate financing, and ineffective governance contribute to poor WASH in Zimbabwe. The evidence provided by the reviewed literature suggests that prolonged unsafe water, sanitation, and hygiene (WASH) were driven by a combination of these key challenges over several decades in the country. Several studies have further revealed that human behaviours characterised by unhygienic households and personal practices, tied with knowledge gaps, increase the risk of adverse health outcomes.
This review identifies key equity dimensions of water access/service, water quality, 49 sanitation,50,51 gender roles, 49 and poverty quintiles.48,49 The lack of girl-friendly WASH infrastructure in rural schools constrains menstrual hygiene waste, 41 suggesting gender and educational disparities between institutions. The review further reflects that rural-urban disparities remain a major concern in the WASH landscape in Zimbabwe. 48 Despite concerted efforts and the implementation of WASH interventions, low-income households, 33 and vulnerable individuals, such as people with disabilities, continue to face significantly greater challenges in accessing basic sanitation and improved water supply. This situation implies limited progress towards equitable access to WASH in Zimbabwe
The recurrent WASH-attributable diseases from the reviewed articles include increased prevalence of diarrhoeal diseases, persistent enteric infections, and outbreaks (ETEC, Shigella, typhoid, and cholera),33,36,39,43 -45 and higher burdens of neglected tropical diseases (schistosomiasis and STH),8,34,35 coupled with the risk of malnutrition. Likewise, the cumulative negative health impacts were reported to be most prevalent among children under 5 years old,8,43 poor households, and rural areas due to these water and sanitation-related preventable illnesses. Therefore, the reviewed articles and records suggest that decades of inadequate water, sanitation, and hygiene (WASH) infrastructure and services have contributed to numerous negative public health outcomes in Zimbabwe.
Overall, the studies reviewed provide a solid foundation to conclude that despite numerous WASH initiatives and interventions, improving various health outcomes in Zimbabwe still faces substantial obstacles. Therefore, the present study recommends improvements in water infrastructure, water supply management, sanitary facilities, and community-led WASH practices to improve health outcomes in Zimbabwe’s rural areas. Achieving the desired health outcomes related to WASH requires a fundamental shift in the community’s knowledge, attitudes, practices, and behaviours (KAPB). Funding the Rural Water Information Management System (RWIMS) is crucial for monitoring the water supply infrastructure, interventions, and activities in Zimbabwe. However, the reviewed articles and other records call for urgent policy action, and there is a lack of discussion on how to implement these policies effectively. Future research should focus on the barriers to policy implementation and strategies for overcoming them.
Strengths and Limitations
A key strength of this review is its longitudinal timeframe, which enables the assessment of both short- and long-term impacts of WASH interventions on health outcomes. This provided a comprehensive understanding of the temporal dynamics. Furthermore, the scope of this review extends beyond diarrhoeal diseases and encompasses a broader range of WASH-related health outcomes. This holistic approach contributes to a more comprehensive understanding of the subject matter. The reliability of this study was enhanced by rigorous searches across highly comprehensive databases. Although focussing on Zimbabwe enhances the contextual relevance of this study, it may limit the generalisability of the findings to other settings. Furthermore, the heterogeneity observed across studies in terms of interventions, populations, and outcome measures poses significant challenges. This variability can hinder the seamless integration of findings into broader contexts.
Footnotes
Acknowledgements
Not applicable.
Author Note
SB holds an MSc in Public Health degree from the Universitas Indonesia and an MSc in Biostatistics and Epidemiology degree from the Midlands State University of Zimbabwe. The author is the District Environmental Health Officer for the Zvishavane District within the Ministry of Health and Childcare in Zimbabwe. VN holds an MSc in Public Health from the University of Zimbabwe. The author works as the Environmental Health Director of Zimbabwe’s Ministry of Health and Child Care. WNN is a PhD in Public Health and an Associate Professor and Acting Head of School of Public Health in the Faculty of Health Sciences at the University of Botswana.
Ethical Considerations
Ethical approval was obtained from Universitas Indonesia (Ket26/UN2.F10.D11/PPM.00.02/2024), the Zimbabwe Medical Research Council (MRCZ/B/2629), and the Ministry of Health and Child Care.
Consent for Publication
Not applicable.
Author Contributions
SB, WNN, and VN conceptualised the research idea. SB, WNN and VN conducted a literature search, performed data extraction, and drafted the manuscript. WNN provided visualisation. WNN supervised the manuscript writing process. All the authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable.
Human and Animal Rights
Not applicable.
Patient and Public Involvement
None.