
Abstract
Objectives:
This study aimed to outline water, sanitation, and hygiene (WASH) practices for children under 5 years of age among the households of St. Martin’s Island as well as examine the role of water, sanitation, and hygiene on child nutritional outcomes.
Methods:
A total of 256 children under 5 years of age were anthropometrically measured, and multiple linear regression was performed to understand the relationship between combined water, sanitation, and hygiene score and child nutritional outcomes: height-for-age, weight-for-age, weight-for-height z-scores.
Results:
The majority of the sampled households had improved drinking water facilities. Over one-third of the participants (36.5%) did not have access to better sanitation, and 12.4% reported defecating in open places. Just over one-third of those surveyed reported washing their hands with soap or detergents after defecation, with more than 22% of people not having access to a handwashing station on their premises. Stunting, wasting, and underweight were found to be prevalent in 34.4%, 17.6%, and 18.9% of the sampled children, respectively. Height-for-age (0.08 SDs) and weight-for-age (0.014 SDs) were greater on average in children from households with improved water, sanitation, and hygiene conditions, but weight-for-height did not significantly differ from those from WASH-unimproved households.
Conclusion:
Certain aspects of WASH, particularly, sanitation facilities and hygiene practices were not up to the mark in St. Martin’s Island, and consistent with findings from other studies, our study findings underlined the potential benefits of improved water, sanitation, and hygiene practices in addressing child undernutrition.
Introduction
Child undernutrition is one of the most pressing public health issues in low- and middle-income countries. 1 The indicators of undernutrition include stunting (low height-for-age), wasting (low weight-for-height), and underweight (low weight-for-age). 2 In 2020, around 149 million children throughout the world were stunted, 45 million were wasted, and 38.9 million were overweight. 3 Although Bangladesh has made significant progress in combating child malnutrition in the past few decades, the high prevalence of malnutrition is, even now, one of the leading causes of morbidity and mortality among children under 5 years of age. 4 An estimated 31%, 8%, and 22% of Bangladeshi children are stunted, wasted, and underweight, respectively, according to the Bangladesh Demographic and Health Survey 2017–18. 5
Children suffer from undernutrition for several reasons, which are classed as immediate (individual level), underlying (household or family level), and basic (societal level) in UNICEF’s conceptual framework. 6 One of the underlying causes of undernutrition is the poor health and environmental condition of households, including an insufficient supply of clean water and improved sanitation service. 7 There are a lot of studies on the adverse consequences of poor WASH practices on child nutrition, such as safe drinking water, improved sanitation, and hand hygiene practices.8–12
Poor water, sanitation, and hygiene (WASH) practices are linked to child survival, growth, and nutritional outcomes in a variety of direct and indirect ways, such as via diarrheal diseases, intestinal parasite infections, and Environmental Enteric Dysfunction (EED). 13 Unsafe water, inadequate sanitation, or insufficient hygiene mediate transmission of fecal pathogens14,15 that cause diarrhea, and frequent episodes of diarrhea, in turn, induce child growth deficits. 16 However, recent evidence suggests that the primary causal pathway for the impact of poor WASH practices on child undernutrition is via tropical or environmental enteric dysfunction, which is caused by the ingestion of fecal bacteria in large quantities by children living in filthy surroundings.13,17 In addition, indirect impacts of WASH also occur through walking long distances to find water and sanitation facilities and diverting mothers’ time for child care. 18
Nonetheless, research on the relative effectiveness of WASH interventions on child undernutrition provides conflicting results. There have been several cross-sectional studies that demonstrated the beneficiary role of WASH on child growth indicators.13,19,20 On the other hand, a cluster-randomized controlled trial (RCT) in rural Bangladesh demonstrated that integration of water, sanitation, and handwashing with nutrition did not result in superior linear growth of children. 21 Similar findings were reported in two other investigations conducted in Kenya and India.22,23
During the past decade, Bangladesh has made remarkable progress in expanding the use of water and sanitation facilities, following the adoption of the National Hygiene Promotion Strategy for Water Supply and Sanitation.24,25 Despite dramatic reductions in open defecation, many parts of the country still have unsafe sanitation and poor hygiene practices. 24 Besides, frequent diarrheal episodes are leading causes of childhood death in Bangladesh; likely due to inadequate WASH facilities. 5
Located just south of Bangladesh, St. Martin’s Island is the most south-easterly spot and is the country’s only coral-bearing tropical island. The island is separated from the mainland of Bangladesh by water, and the only way to reach there is via boat or ship (primarily for tourists) from Cox’s Bazar and Teknaf. Although this small continental island of the Bay of Bengal is famous for its natural beauty, ecological and biodiversity value, there are about 7000 inhabitants who live primarily on fishing and tourism whose lifestyle and livelihood are distinct from those of the rest of the country. However, the novelty of the study lies in the selection of the study area, since, to our knowledge, this community has not been brought under any health or nutrition survey investigating child nutritional status and WASH practices. Therefore, this study is the first-ever nutrition study that seeks to investigate WASH practices for children under 5 years of age among the households of St. Martin’s Island as well as examine the role of WASH on child nutritional outcomes.
This study aimed to examine the association between WASH practices regrouped as child-sensitive WASH composite score and different child nutritional outcomes measured as height-for-age z-score (HAZ), weight-for-age z-score (WAZ), and weight-for-height z-score (WHZ) among children under 5 years of age. The outcomes of the study are expected to assist the Bangladesh government in implementing successful programs in St. Martin’s Island to enhance the overall living standard of the inhabitants that will ultimately improve their health and nutritional condition.
Methods
Study design, setting, and subjects
We conducted a household cross-sectional survey in St. Martin’s Island between 1 March 2020 and 7 March 2020, covering the entirety of the island with nine villages: Purba para, Deil para, Majher para, Konar para, Uttar para, Dakshin para, Zinzira, Pachim para, and Nazrul para. This study was based on a stratified sample of households; each village was designated a stratum, and with proportionate allocation, the entire sample was distributed into nine strata (nine strata because there were nine villages). A modified Expanded Program of Immunization (EPI) sampling approach 26 was applied to select the households since a complete list of the households was unavailable. The study’s inclusion criteria were that the household had at least one child under 5 years of age. We selected mothers or primary care givers of young children under the age of 5 as respondents.
Justification of sample size for children under 5 years of age
The required sample size was calculated as 254 considering the point prevalence of stunting in Bangladesh among children under 5 years of age (28%) after adjusting for known population effect according to the corrected Cochran’s formula (equation 1) since the population size was known from population and housing census report. 27 Because there were 256 children in this study, the number of children under 5 years of age was adequate to reflect St. Martin’s Island.

Data collection and analysis
Enumerators collected relevant data from study subjects using a paper version of the semistructured questionnaire and 1 week before the final study, 10% of the entire sample was examined in a pilot study. Children’s height/length, weight, and mid-upper arm circumference (MUAC) were measured by weight scale, height scale, and MUAC tape.
Demographic details, as well as WASH practices, were collected for the study population. Core questions on WASH were all included in the final version of the questionnaire as per recommendations by the WHO/UNICEF 28 Joint Monitoring Program (JMP) for household surveys. We also included three child-related questions: children’s use of sanitary latrines, child excreta disposal procedures, and mothers’ handwashing practices before child feeding. Fieldworkers conducted one spot check per household. They inspected water supplies and storage conditions for drinking and other uses and the type and conditions of the sanitation facilities. The presence of water, soap, or another disinfection agent was also noted at the handwashing location.
The respondents were requested to describe how they maintained hand hygiene and where their children defecated most frequently. Hand hygiene practices of mothers during complementary feeding were observed only in those who were feeding their children during enumerators’ home visits, otherwise, information from respondents was recorded.
Anthropometric data processing
To assess the nutritional status of children under the age of 5, WHO Anthro software (version 3.3.2) was used to calculate the HAZ, WAZ, and WHZ from anthropometric data. We adopted World Health Organization (WHO) 29 growth standard to classify children as stunted (HAZ <–2SD), underweight (WAZ <–2SD), and wasted (WHZ <–2SD). Moreover, following WHO recommendations, any subject with HAZ either above +6 or below −6 SD, WAZ above +5 or below −6 SD, and WHZ above +5 or below −5 SD were considered as incorrect z-score values (flag data); thus, excluded from the analysis. 30
WASH measurement
We assessed and categorized household access to WASH facilities, as well as handwashing practices of mothers or primary caregivers of children, using JMP’s standard categorization approach. Each facility or practice was considered either as “improved” or “unimproved” following the JMP monitoring definition for different WASH components 28 (Supplemental Table 1). Child-related WASH practices were categorized based on literature since it is not a component of JMP classification. 10 The values for each variable were rated as “improved” (coded 1) or “unimproved” (coded 0), giving each variable a possible score of 0 or 1. Then, utilizing household-level water, sanitation, handwashing facility, and handwashing habits of mothers, as well as child-specific WASH practices, a child-sensitive WASH composite score was calculated using 19 variables in total, resulting in a score range of 0 to 19 (Table 1).
Indicators of water, hygiene, and sanitation (WASH) practice that was used to develop child-sensitive WASH score.

Receiver Operating Characteristics (ROC) curve analysis was performed to identify WASH cut-off points optimizing sensitivity and specificity for different anthropometric indices. The ROC curve is a useful tool for establishing the best cut-off point for a measurement that optimizes true positives (sensitivity) while minimizing false positives (1—specificity), and so maximizes the likelihood ratio. For all of the anthropometric measures, a cut-point ⩾ 14 was considered appropriate in predicting the nutritional status of children (Table 2). Therefore, we categorized the child-sensitive WASH composite score as “improved WASH condition” with a WASH score of ⩾ 14 and “unimproved WASH condition” with a WASH score < 14. Because the WASH score was discrete and resembled count data, it was categorized into a binary variable so that it could be included in the parametric linear regression model. Although a similar study conducted in Cambodia 10 utilized WASH composite score as a continuous variable; Lin et al. 13 treated WASH as a binary variable like ours.
Sensitivity and specificity at different WASH score cut-off points for classifying children as stunted, wasted, and underweight.
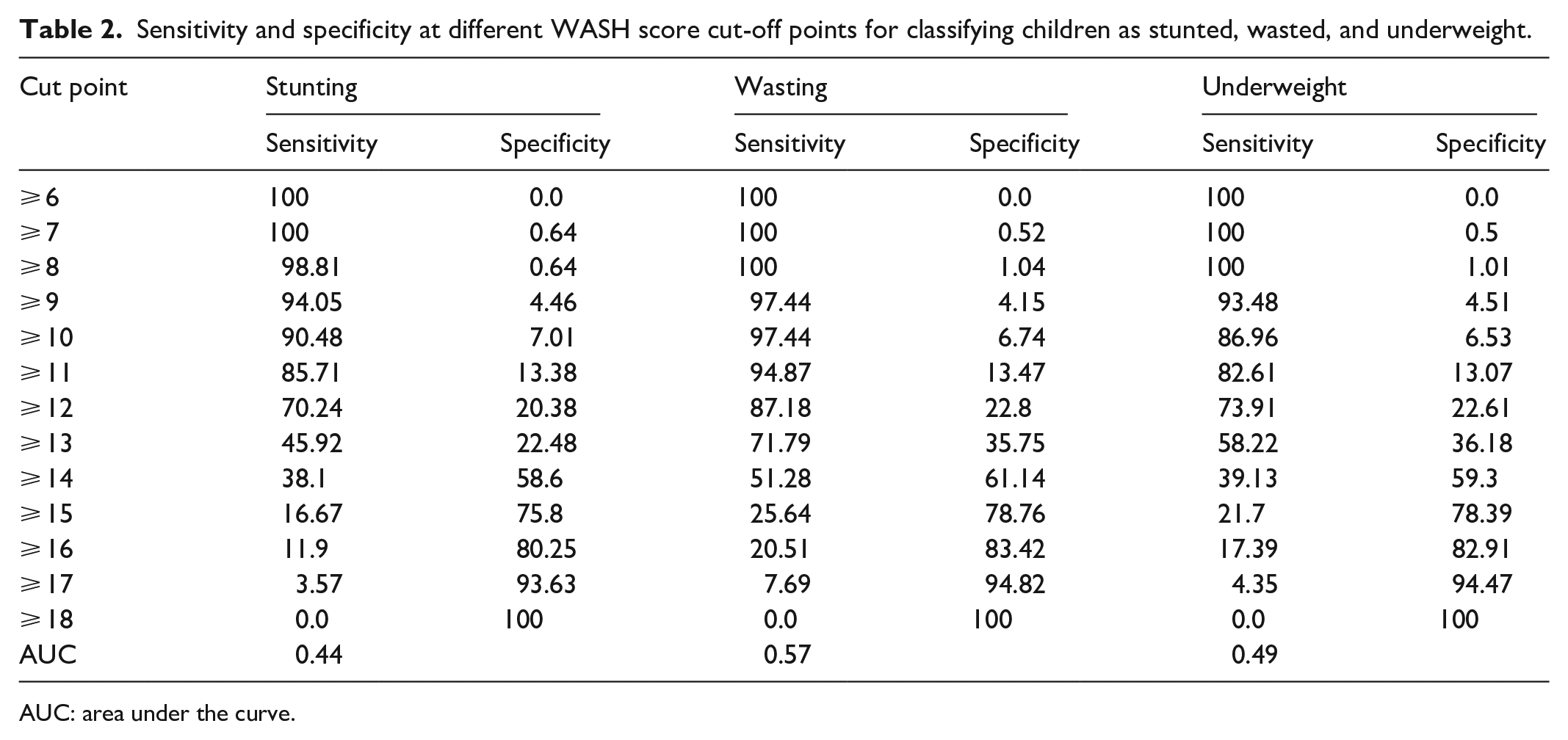
AUC: area under the curve.
Confounders
Based on the UNICEF conceptual framework for childhood undernutrition 31 and relevant literature,4,8,9,20 a set of variables were identified prior to analyzing the potential confounding effect of various determinants of child undernutrition. Both individual- and household-level factors were considered as exposure variables in the analyses. Child age (in months), gender, birth order, and child dietary diversity score (DDS) were important individual factors. Child dietary diversity was measured following WHO 32 guidelines. Household factors included wealth index, household monthly income, family size, number of living children, and food security status. Household food security status was measured by the Food Insecurity Experience Scale (FIES) as developed by FAO. 33 Over a 12-month recall period, FIES elicits self-reported experiences and behaviors related to food access owing to a lack of money or other resources, regardless of the frequency of occurrence. The FIES comprised eight questions ranging from low food insecurity (question 1) to severe food insecurity (question 8) (Supplemental Table 2). After that, “Yes” responses were coded as 1, and “No” responses were coded as 0. The total raw score ranges from 0 to 8 and a food secure household was defined as a FIES score of zero, whereas, a household FIES score of ⩾1 was defined as food insecure. The household wealth index was calculated through principal component analysis (PCA) 34 and the variables used for wealth index calculation are listed in Supplemental Table 3. In addition, the education level of the child’s parents and the nutritional status of the mothers were also treated as a confounding variable. The body mass index (BMI) was calculated and Asian-specific cut-offs were used to measure the nutritional status of mothers. 35
Statistical analysis
Descriptive statistics were computed in terms of frequency, percentage, mean and standard deviation. We also investigated the normal distribution of variables before analysis through visual inspection of the histogram, Q–Q plot, detrended Q–Q plot, Box plot, and using statistical test—Kolmogorov–Smirnov and Shapiro–Wilk test. 36 Primary outcome variables were HAZ, WAZ, and WHZ. While dichotomously categorized child-sensitive WASH composite score was the major exposure variable. Independent sample t-test and ANOVA (factorial ANOVA, MANCOVA) were performed to compare the unadjusted and adjusted differences in mean HAZ, WAZ, and WHZ between two WASH conditions. The adjusted analysis, in contrast to the unadjusted analysis, took into consideration the effects of a variety of factors.
Regression models
The relationship between WASH and different indicators of child nutritional status was examined using simple and multiple linear regression models. Three different linear regression models were fitted for three response variables (HAZ, WAZ, WHZ). At a significance level of 0.05, simple linear regression models examined the strength of the association between individual factors and child nutritional indicators. The stepwise forward entry method was used to select those variables that were significant (p < 0.05) in simple linear regression analyses for inclusion in multiple linear regression models. Multiple linear regression models explored the impact of WASH on child nutritional indicators after adjusting for potential confounding factors.
Furthermore, particular measures were taken to investigate the interaction between WASH and food insecurity, as UNICEF’s 31 theoretical framework suggested both WASH and household food insecurity as underlying determinants of child malnutrition. Using multiple linear regression analyses, we looked at the interaction effect between WASH and food insecurity to determine whether food insecurity is a mediating factor in the association between WASH and child nutritional outcomes. The interaction was not significant at p < 0.05 level, therefore, was left out of the final regression models.
Before final model building, the underlying assumptions of the linear regression models were tested. Variance inflation factor (VIF) was examined to check the amount of multicollinearity in the model and a VIF greater than two was considered to indicate multicollinearity. 36 The residual for each case was calculated and the normality of residuals was inspected. We also observed Cook’s distance and leverage values to identify multivariate outliers and the critical value for Cook’s distance was set to 1 which is 0.05 for the leverage value. Statistical Package for Social Science (SPSS), version 25 was used to perform all statistical analyses.
Ethical approval
The ethical review committee of the Faculty of Biological Sciences, University of Dhaka reviewed and approved the study (Ref. No. 116/Biol. Scs.). The nature and purpose of this study were described to all study participants, and because most of the respondents were illiterate, verbal rather than written consent was obtained prior to study initiation. This sort of informed consent was authorized by the Institutional Review Board.
Result
The demographic and socioeconomic characteristics of the study population are presented in Table 3. Over half of the children (53.9%) were boys, and 40.6% of them were between the ages of 48 and 59 months. In addition, 34.4%, 17.6%, and 18.9% of children were found to be stunted, wasted, and underweight respectively. Moreover, 26.4% of children under 5 years of age had diarrhea in the 2 weeks preceding the survey, and deworming medication was not provided to almost 100% of children. More than half of the children’s fathers had completed up to the primary level of education (53.9%) and less than half of them were engaged in fishing (47.4%).
Demographic and socioeconomic characteristics of study subjects (N = 256).

Almost every household on St. Martin’s Island had improved water supplies, and around 73% of the sampled households had access to a private water source (Table 4). Nearly two-thirds (63.2%) of households had improved sanitation facilities, while 12.4% reported open defecation. Only 16.4% of families reported having soap and water for handwashing, even though more than 75% of families had a handwashing facility on their premises. In two-thirds of the households (66.2%), only water/ash/soil was used for handwashing after defecation, while the remainder reported using soap/detergent. Furthermore, nearly three-quarters (74.5%) of the mothers reported washing their hands before feeding their children, but only one-quarter (25.6%) disposed of their child’s excreta in the latrine.
WASH practices among households of St. Martin’s Island.

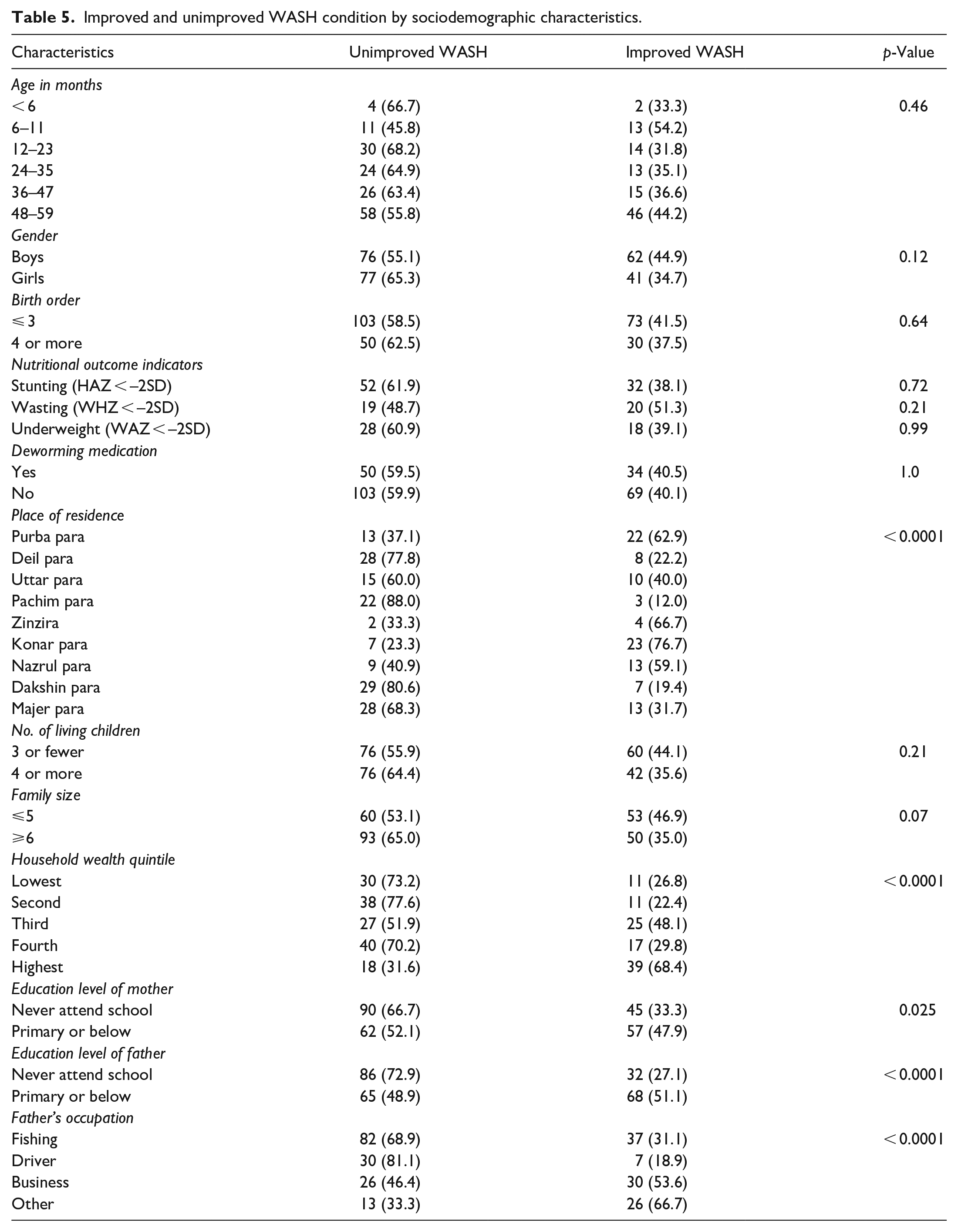
WASH conditions by the sociodemographic characteristics have been presented in Table 5. Improved and unimproved WASH conditions were significantly associated with the place of residence, household wealth quintile, education level of parents, and occupation of the father. Higher percentages of residents of Purba para (63%), Zinzira (67%), Konar para (77%), and Nazrul para (59%) were found to have improved WASH conditions. In the wealthiest quintile, there were more households with improved WASH conditions. Furthermore, parents without formal education were more likely to practice unimproved WASH practices and WASH conditions were less improved in households with a principal earning member involved in fishing (31%) and driving (19%).
Improved and unimproved WASH condition by sociodemographic characteristics.
The unadjusted and adjusted differences in mean HAZ, WAZ, and WHZ between the improved and unimproved WASH conditions are presented in Table 6. Both unadjusted and adjusted analyses revealed that children from households with unimproved WASH conditions were on average shorter than those from households with improved WASH conditions. The unadjusted difference in mean HAZ between unimproved and improved hygiene conditions was −0.39 SDs (p < 0.0001). While, after statistical adjustment for potential confounding factors, children from households with unimproved WASH conditions had −0.288 SDs lower HAZ (p < 0.05). In the unadjusted analysis, there was no significant difference in WAZ between the two household environmental situations; while, following statistical correction, similar to HAZ, children with an unimproved environment had substantially lower WAZ (–0.298 SDs) on average (p < 0.05). In contrast to the other measures, even after statistical adjustment, the mean WHZ did not differ substantially between the two WASH conditions.
Unadjusted and adjusted differences in nutritional outcomes among children living in different household environmental condition (N = 256).

Improved WASH condition: WASH score ⩾ 14, Unimproved WASH condition: WASH score < 14.
For unadjusted difference: independent sample t-test. Age and sex-adjusted difference: general linear model (factorial ANOVA/three-way ANOVA). Fully adjusted difference: analysis of covariance (MANCOVA); adjust for age, sex, hygiene, and one or more continuous variables (Covariate). Covariates were selected based on their association with outcomes. A list of possible covariates was prepared (Supplemental Table 4), then linear regression analysis was performed. Covariates are those that have a linear association with outcome.
p < 0.05, ***p < 0.0001.
Association between WASH and child nutritional outcomes
Table 7 depicts the adjusted and unadjusted linear association between potential predictors of child nutritional status and child nutrition outcome measures (HAZ, WAZ, and WHZ). Children from households with improved WASH condition had on average higher HAZ (0.08 SDs) than those from unimproved WASH condition. Among other factors, HAZ was found to have a significant association with child age, gender, household food security condition, and household wealth score.
Association between different nutritional indices and child-sensitive WASH composite score (N = 256).

ref: reference.
Results from simple linear regression model.
Results from multiple linear regression model.
p < 0.05, **p < 0.01, ***p < 0.0001.
Our study analyses showed no evidence of WASH having a major impact on WHZ, even though, in addition to the child’s age and gender, WHZ was associated with the education level of the father and household food security status. In food secure households, WHZ was on average 0.65 SDs higher than in food-insecure households.
On the other hand, similar to HAZ, children from families with improved WASH practices, had on average higher WAZ (0.014 SDs) than children from households with unimproved WASH practices. Our analyses also suggested the education level of fathers and diarrheal occurrence as significant predictors for WAZ. Children, who did not have diarrhea in the 2 weeks preceding the survey had a higher WAZ score.
Discussion
The findings of this cross-sectional study revealed suboptimal sanitation and handwashing facilities, as well as hygiene practices for children under 5 years of age among the households of St. Martin’s Island. Almost all of the studied households had access to improved drinking water facilities, while nearly a third lacked sanitation facilities. Moreover, three-quarters of child’s mothers stated that they washed their hands before feeding their children, yet only 16% had access to soap or detergent for washing their hands. In the adjusted analysis, it was found that improved WASH practices were positively associated with the HAZ and WAZ which implies that in the improved WASH group, the z-score of height-for-age and weight-for-age was greater than in the unimproved group.
In the latest National Hygiene Survey of Bangladesh in 2018, 25 97.5% of households had access to an improved water source and the estimate for households on St. Martin’s Island is consistent with the national figure (99.5%). In the case of sanitation, the situation among residents of St. Martin’s Island appears to be worsening as compared with the rest of the country as per the findings of the national hygiene survey, which found that 86% of Bangladeshi households had access to improved latrines (including shared). Of particular note is that the number of households practicing open defecation was 12.4% in this island against only 1.7% of all households in Bangladesh. 25 Further, a basic handwashing facility was available to around 16% of households, whereas more than two-fifths of them reported no access to a handwashing facility in their yard. Nearly, one-third of the sampled households were observed to have a handwashing facility for postdefecation use with water and soap/detergent which was lower than that reported by the national hygiene survey of Bangladesh and UNICEF/JMP 2019.
The adjusted analyses found that HAZ and WAZ were significantly lower among children living in unimproved WASH conditions, which is in agreement with a previously conducted observational study in rural Bangladesh. 13 Moreover, both adjusted and unadjusted analyses showed evidence for a significant association between WASH practices and child nutritional outcome indicators. The adjusted model for HAZ and WAZ predicted that improved WASH practices were significantly associated with an increase of 0.08 SDs in HAZ and 0.014 SDs in WAZ. A similar study among Cambodian children also stated that for each unit increase in the JMP child-sensitive WASH composite score, HAZ and WAZ increased by 0.21 SDs, and 0.28 SDs, respectively. 10
Several observational studies clinched that household sanitation coverage, handwashing behavior, and drinking water availability were all significantly associated with HAZ or stunting.8,11,12 Similarly, improved WASH practices were positively associated with HAZ and WAZ in this study. Evidence from three RCTs suggested a reduction in child stunting after sanitation intervention37–39 and Dangour et al. 40 stated a positive effect of water quality and handwashing intervention on child linear growth. In the same way, a child’s WAZ was found to be increased with sanitation coverage and handwashing practice with soap and water in an observational study in Nepal. 12 According to our findings, as was the case in two other studies in Ethiopia and Nepal,8,12 WHZ was not significantly associated with overall WASH conditions in this study, although that did not hold for a study in Bangladesh. 41
In addition to WASH, the literature suggests that household food insecurity is associated with child nutritional outcomes such as stunting and underweight.31,42 One of the prime concerns of this study analysis was to examine the effect of WASH on child nutritional indicators after controlling the effect of potential confounding factors including food insecurity. In simple linear regression, where confounding factors were not considered, a statistically significant association between WASH and HAZ and WAZ was revealed. Even after controlling for potential confounding factors with multiple linear regression models, the results remain the same, although the magnitude of association (beta coefficient) declines. Furthermore, there was no interaction effect between WASH and food insecurity, implying that WASH’s impact on child nutritional outcomes was unaffected by food insecurity.
Poor WASH practices along with higher diarrheal occurrence among children 2 weeks before the study was also an important finding of this study. There is a direct association between diarrhea and malnutrition; WASH is majorly perceived and proved to be one strongest predictors of diarrhea. 17 The latest data from the Demographic and Health Survey of Bangladesh indicates that 4.8% of children had diarrhea which is almost five times higher (26.4%) in our study area. Besides, on this island, all forms of child undernutrition: stunting, wasting, and underweight are more prevalent than it is on the mainland of the country. 5
Water quality is important for the health condition of children since contaminated water can spread diseases like diarrhea, cholera, dysentery, typhoid, and so on. The prevalence of childhood undernutrition and diarrhea was high in St. Martin’s Island although the majority of the households had improved drinking water facilities. Even if drinking water facilities are upgraded, water can still be contaminated, for example, water can become contaminated during storage or microbial contamination can occur. However, scientific evidence suggests that helminth and parasitic infection have been strong predictors of child nutritional status 43 which is cinched with poor sanitation practices as well. Therefore, due to the poor sanitation status in the sampled households, there is a greater probability that the proportion of soil-transmitted helminth infections may be higher than that transmitted from poor-quality water. Furthermore, just one-fourth of the child’s mothers used a toilet to dispose of their child’s excreta, increasing the risk of helminth infection. In addition to helminths, children can acquire infections that affect their nutritional status from a variety of sources (e.g., filthy hands, polluted surroundings, contaminated food).
The implication of the study findings
The statistically significant (p < 0.05) effect of WASH on HAZ and WAZ as found in the current analysis has substantial practical implications. A small change in HAZ is important since stunting or a low HAZ score is an indicator of poor environmental conditions or a long-term restriction of a child’s growth potential, and this indicator is frequently used to target development initiatives. On the other hand, low WAZ or underweight reflects both chronic and/or acute undernutrition and evidence shows that children who are even mildly underweight have a higher mortality risk, while severely underweight children have a higher risk. 44 The findings of the study imply that both government and Non-governmental Organizations (NGOs) should collaborate in St. Martin’s Island to integrate WASH interventions such as hygiene promotion, provision of sanitation infrastructure into nutrition programs. Long-term exposure to high-quality hygiene and sanitation may be required to improve child linear growth.
Strength and limitation
With a high response rate, this study utilized population-based data representative of all local administrative entities of St. Martin’s Island. The findings of this study could be generalized to St. Martin’s Island and provide supporting evidence on the effect of WASH on child nutritional status, which could be useful for policymakers, WASH, and nutrition advocates working to improve child health. However, this study is not beyond all limitations. A cause-effect relationship could not be established due to the cross-sectional nature of the study although a recent study suggested that a cross-sectional study can provide valuable insight into local, regional, and national policy decisions. 45 Moreover, rather than examining the impact of individual WASH components, we assessed the impact of the overall WASH condition, as measured by the child-sensitive WASH composite score. The use of such an indicator score and the dichotomization of WASH scores may cause some of the household’s WASH practices to be misclassified. Even though we adjusted for the majority of the confounders discovered in other nutritional research, the possibility of residual confounding due to unknown factors could not be completely ruled out. Although we sought to reduce self-reported bias in our study by integrating various replies and observations, there is still a possibility of self-reported bias. However, Ram et al. 46 stated that observing practice is expensive, intrusive, results in reactive behaviors, and is only practical on a small scale. In addition, area under curve (AUC) was very low in some cases implying that the models could not distinguish the binary outcome variables well.
Conclusion
This study sought to evaluate WASH practices for children under 5 years of age among the households of St. Martin’s Island, as well as the role of overall WASH condition, defined as child-sensitive WASH composite score, on child nutritional status. On the island, several aspects of WASH, such as sanitation facilities and general hygiene practices, were in disarray, raising the risk of intestinal parasite diseases. It was noteworthy that a high proportion of children on St. Martin’s Island suffered from malnutrition and diarrheal disease although most of the households had access to improved drinking water facilities. In addition, this study also identified the protective role of improved WASH practices on the risk of stunting (low height-for-age z-score) and underweight (low weight-for-age z-score) in children under 5 years of age on this island. We recommend that a qualitative study should be conducted on this island for a better understanding of WASH-related practices and behaviors among permanent residents, which was beyond the scope of the present study. Furthermore, randomized controlled trials would be imperative to elucidate a closer association between different WASH components and child growth.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221095966 – Supplemental material for Child-sensitive water, sanitation, and hygiene composite score and its association with child nutritional outcomes in St. Martin’s Island, Bangladesh
Supplemental material, sj-docx-1-smo-10.1177_20503121221095966 for Child-sensitive water, sanitation, and hygiene composite score and its association with child nutritional outcomes in St. Martin’s Island, Bangladesh by Ahmed Jubayer, Md. Hafizul Islam and Md. Moniruzzaman Nayan in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121221095966 – Supplemental material for Child-sensitive water, sanitation, and hygiene composite score and its association with child nutritional outcomes in St. Martin’s Island, Bangladesh
Supplemental material, sj-docx-2-smo-10.1177_20503121221095966 for Child-sensitive water, sanitation, and hygiene composite score and its association with child nutritional outcomes in St. Martin’s Island, Bangladesh by Ahmed Jubayer, Md. Hafizul Islam and Md. Moniruzzaman Nayan in SAGE Open Medicine
Footnotes
Acknowledgements
The authors fill to express heartful thanks to Md. Nazrul Islam Khan, former professor of, the Institute of Nutrition and Food Science, the University of Dhaka for his encouragement, support, and cooperation in the study.
Data availability
Original dataset cannot be shared right now since we have a plan to submit another research work using the same dataset.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from ethical review committee of the Faculty of Biological Sciences, University of Dhaka (Ref. No. 116/Biol. Scs.)
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The nature and purpose of this study were described to all study participants, and because most of the respondents were illiterate, verbal rather than written consent was obtained prior to study initiation. This sort of informed consent was authorized by the Institutional Review Board. Moreover, no minor subjects were involved in this study and child mothers (respondents) were not minor subject.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.