
Abstract
Objective
The objective of this study was to deliver an intervention to improve health awareness for infection prevention, hygiene, and sanitation to assess its impact. Furthermore, it aimed to identify the risk of multimorbidity in women of reproductive years from low socio-economic background.
Methods
A randomized control trial was conducted in Pakistan among women aged 15–45 years. Overall, 820 women participated in the baseline survey; 388 women were part of the control group and 360 of the intervention group. A digital health literacy intervention was delivered by 91 trained community health workers. Data were analyzed using descriptive statistics and multivariate logistic regression.
Results
About 35.9% of women suffered from multimorbidity. The intervention group showed higher odds of confidence in managing health with respect to skill and technique acquisition (AOR = 2.21; 95% CI 1.01–4.84), self-monitoring and insight (AOR = 2.97; 95% CI 1.29–6.80) as well as sanitation and hygiene (AOR = 1.42; 95% CI 1.07–1.93). Two primary outcomes related to hand hygiene and protective behavior against infection did not show any significant improvement. The secondary outcomes of the study related to impact on overall health-related quality of life, social integration and support, and emotional well-being also did not show any significant improvement.
Conclusions
Digital health literacy interventions and multimorbidity management for women of reproductive years at the primary level are a way forward to alleviate communicable and non-communicable disease burden in developing countries like Pakistan. These efforts are also critical to improve maternal and child health in developing regions.
Keywords
Introduction
Women of reproductive age in South Asia are at risk to face a lack of satisfactory services for primary healthcare.1,2 The majority of women in this region are from low socio-economic backgrounds and have low health literacy. However, only limited efforts to improve health awareness for improving self-management skills are available.3,4 Some local health education programs investigated via randomized-controlled trials (RCTs) have targeted services for women of reproductive age at community-level, but have concentrated specifically on awareness about preventing malaria, 5 early breast cancer detection, 6 and promotion of maternal health.7,8 There have been no broad interventions to improve health literacy in women for the management of non-communicable diseases, communicable diseases, and hygiene and sanitation. The importance of latter has considerable importance, because the management of the coronavirus pandemic is highly dependent on women's leadership in the homes for infection prevention and sanitation, for herself, her children, and family members.
The negligence of women's health at primary level and low health literacy also mean that there is limited evidence about the prevalence of multimorbidity in women of reproductive age in Pakistan. However, some research has highlighted that multimorbidity is a grave concern not just for aging women, but also for women in the reproductive phase.9,10 In fact, some research highlights that multimorbidity occurs a few decades earlier in disadvantaged communities 11 and is more prevalent in women. 12 Multimorbidity prevalence is best detected and managed at the primary level of healthcare. 13 It is also agreed that the best ways to manage multimorbidity and infection control is by educating and improving awareness to prevent deterioration of physical health, support mental health, and improve health policy services from primary to tertiary level. 12 Though local research has highlighted that chronic disease burden amongst poor women of reproductive age at community-level is a significant problem, 14 there has been no research with respect to multimorbidity prevalence in women across Pakistan.
In lieu of all this, the aims of this study were (a) to identify the risk of multimorbidity in women of reproductive age from low socio-economic background in Pakistan and (b) to deliver a digital health literacy intervention to women of reproductive age in primary communities to improve infection prevention and hygiene and sanitation, in order to measure the intervention's impact. The importance of introducing digital literacy interventions cannot be emphasized enough in developing nations like Pakistan, which face challenges of overpopulation and health sector service shortfalls. 15 Digital health service options can also provide improved communication and access to remote and rural populations. However, it is important that training for e-health services is provided to disadvantaged populations unfamiliar with technology. 16 This study also aims to deliver an intervention through community health workers (CHWs) as additional primary healthcare staff, thus lending impetus to strengthening the existing Lady Health Worker (LHW) program, which suffers from understaffing and overburden.17,18
Methods
This RCT received ethics clearance from Forman Christian College University, Internal Review Board (Reference number: IRB-252/06-2020), and the study was registered at clinicaltrials.gov (Trial registration number NCT04603092). Detailed information about the design of the study can be found elsewhere. 19
Settings and participants
The selection criteria for sampling were: (a) women of reproductive years (15 to 45 years), (b) women who were not receiving primary healthcare services from government providers due to lack of geographical access and the existing LHW program, and (c) women from poor socio-economic backgrounds. Data was collected based on permission and approval from the provincial health ministries through the Rural Support Programmes Network. The locations for data collection are summarized in Figure 1 and allocation of number of CHWs and participants per areas are summarized in Table 1. We were able to collect data from two provinces, Punjab and Khyber Pakhtunkhwa (KPK). Overall, six districts were sampled: (a) Punjab districts: Bhawalnagar, Jhang, Toba Tek Singh and Rahimyar Khan and (b) KPK districts: Mardan and Swabi. More information about the 89 Union Council areas where data collection took place can be found in Supplementary File 1.
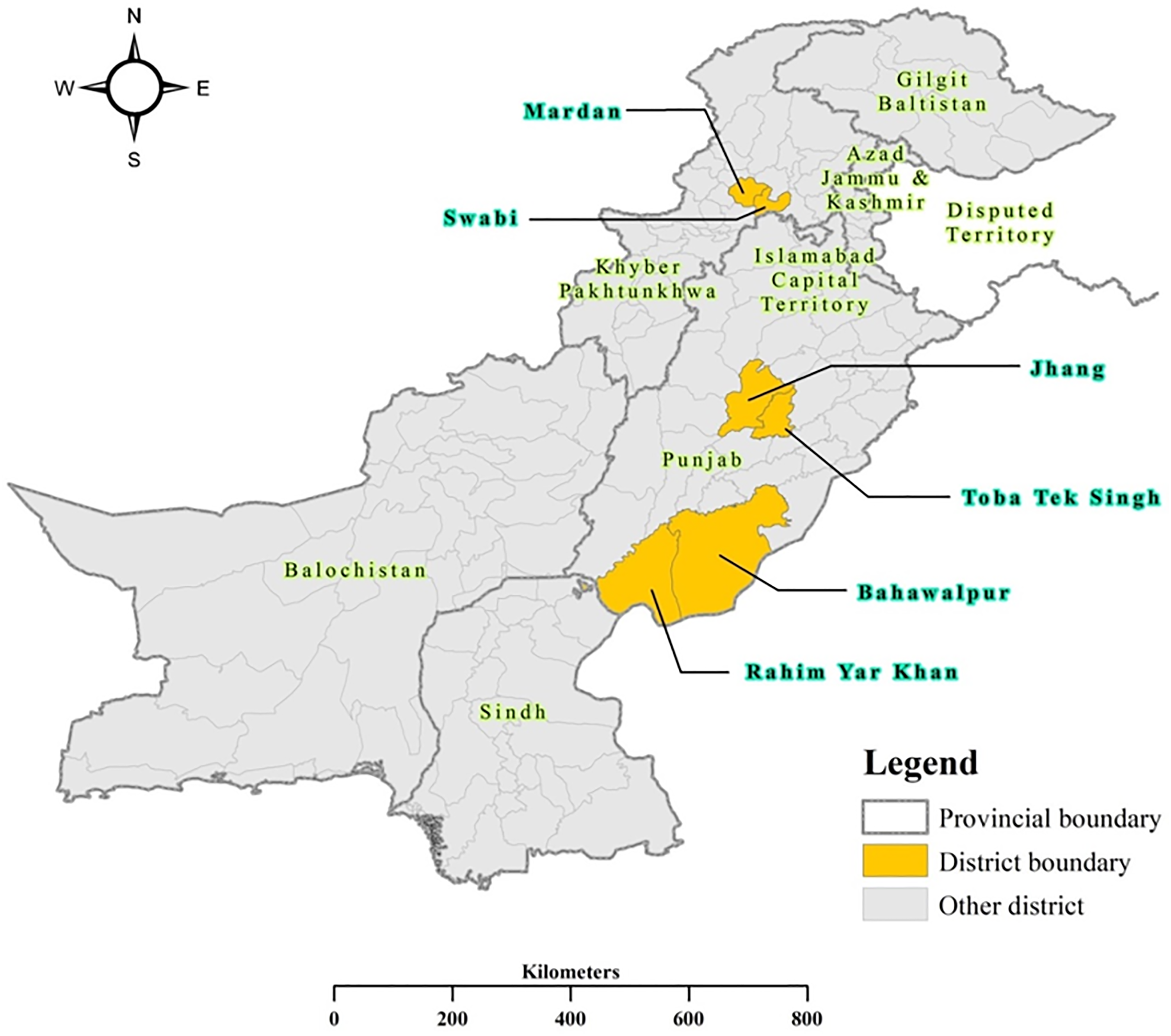
Data collection map.
Study sample and data collectors.

Intervention delivery and community health worker training
A total of 91 CHWs were recruited to deliver the intervention. The recruitment criteria for CHWs were: (a) married women from the community where data collection took place, (b) minimum education qualification of secondary schooling (grade 12 of study), and (c) minimum one-year experience working as health worker in the community. We assigned three CHW Team Leaders for each of the six districts that were sampled and one Field Coordinator for each district. In this way, a total of twenty-four District Team Leaders were responsible for ensuring that each CHW submitted their respective survey data on time and delivered their complete intervention according to the weekly schedule.
The CHWs were trained over a period of 4 weeks through a trickledown process. First the principal investigators (PIs) trained the District Team Leaders and Field Coordinators, and in turn the District Team Leaders and Field Coordinators trained the CHWs. CHWs were trained to understand (a) the objectives of each component of the project, (b) ethics of data collection and research, (c) use of digital tools, (d) communication skills and support of participants, and (e) communication protocols with health consultants and physicians. All CHWs were provided weekly supply of masks and hand sanitizers for themselves and the participants.
Apart from the initial training, written material and guidelines for intervention delivery were provided to the CHWs to help them during the intervention. This material has been attached as supplementary material to the study protocol. 19 The content was translated according to CHW region and differed between one-on-one sessions and group sessions. In addition, the audio and video tutorials were recorded by the PIs so that CHWs could access guidelines and support material on their phone apps. Whatsapp groups and video calls were also used to communicate daily with CHWs. This helped in surveillance of the intervention and also in trouble-shooting daily problems.
The District Team Leaders and Field Coordinators were supervised by the PIs through weekly video meetings and the audit of an entry sheet. The data entry and intervention tracksheet (Appendix A) was maintained online as a shared document between the PIs and the District Team Leaders. This enabled immediate assessment and development of plans to counter problems. Some of the challenges that the PIs and District Team Leaders overcame through regular communication and simultaneous audit of data entry and intervention supervision included: (a) preventing large drop-out rates and improving attendance of participants, (b) ensuring no participant missed an intervention module by requesting CHW for repeat visits, and (c) increasing supply of masks and hand sanitizers for CHWs and participants.
All CHWs were required to submit photographic evidence of their location and field visits, which they transferred to their respective District Team Leaders. The District Team Leaders stored the pictorial proof in the shared online folder. This was considered important as PIs could not travel to remote locations for field audit of the intervention due to time and funding constraints. The CHWs were given a stipend of PKR 1500 (USD 9.07) per month for the project.
Randomized trial
Baseline data and randomization to control and experiment group
Participants completed an initial baseline survey, including questions about socio-demographics, health status, and multimorbidity. They were then invited to participate in a three-month intervention, which would be delivered by CHWs at participant's homes during the one-on-one sessions and at the home of a CHW or a volunteer participant within the community during group sessions. All participants gave written informed consent. Initials or thumb impression was taken from illiterate participants, and in some cases additional verbal consent had to be taken from family or husband for women to participate in the study. Patients were randomly allocated to the intervention and control group. As both the CHWs and participants knew which group they were allocated to, control or experiment, blind randomization was not possible. A pre and post-test survey was administered over a three-month period.
Health literacy booklet for both control and experiment group
Both the control and intervention group received a health literacy booklet which had information modules covering the study domains. It was important for the control group to be provided this health literacy booklet so that we could better understand the impact of the digital literacy intervention on the experiment group. The health literacy booklet was translated in the provincial languages and the participants were informed about the importance of keeping this booklet for the next three months to: (a) use the information for revision regularly and (b) to discuss the content with family members. The booklet material was designed in line with international health communication standards to support communication with illiterate women through the use of colors, symbols, and pictures (Appendix B). The initial steps of sharing the health literacy booklet were helpful in trust and rapport building with participants.
Intervention delivered to the experiment group
The intervention group received the following additional services over a 3-month period. None of these services were provided to the control group, which only received the health literacy booklet as mentioned above:
Health literacy video: this was communicated at least 5–6 times to each participant through the intervention for reinforcement (Appendix C). Live video consultancy with specialists: each participant gained from at least 2–3 live video consultancies through the intervention. One-on-one training: each participant gained from 12 weekly one-on-one sessions, which on average lasted 1–1.5 h. Group training: each participant gained from 3 monthly group sessions. The sessions were held at CHW home or volunteer participant garden area, for an average of 1–2 h. Self-management chart: one booklet provided to each participant, with training and discussion about chart maintenance held 6 times in one-on-one and group sessions. The self-management chart has been published in the appendix of the study protocol.
19
Though the intervention details are provided elsewhere,
19
it is important to summarize again that the intervention content to improve health literacy included: (a) Coronavirus awareness and prevention; (b) Hygiene and sanitation, (c) Self-management of health and chronic disease(s); and (d) Creating awareness for group and peer support for sustaining health. Table 2 summarizes the specific content for each literacy area and also provides information about which tools were used in order to measure the study outcomes.
Summary of intervention literacy areas, specific content for each literacy area and use of tools for delivery.

Note. EW, Emotional wellbeing; HDB, Health-directed behavior; HH, Hand hygiene; HQOL, Health-related quality of life; HSN, Health services navigation; PBC, Protective behavior against coronavirus infection; SH, Sanitation & hygiene; SIS, Social integration and support; SMI, Self-monitoring and insight; STA, Skill and technique acquisition.
Instruments
The “Multimorbidity Assessment Questionnaire for Primary Care” 20 was used to collect baseline data, including information about sociodemographic characteristics, healthcare utilization, chronic diseases, mental health, disease severity, and health-related quality of life.
The pre- and post-test survey included items from three instruments:
The “Health Education Impact Questionnaire”
21
was used to evaluate seven domains: (a) Health-related quality of life; (b) Health-directed behavior; (c) Skill and technique acquisition; (d) Self-monitoring and insight; (e) Health services navigation; (f) Social integration and support; and (g) Emotional wellbeing. The “National Sanitation and Hygiene Knowledge, Attitudes, and Practices Survey”
22
evaluated two domains: (i) Sanitation and hygiene and (ii) Hand hygiene. The “Community-Based Assessment of Knowledge, Attitude, Practices and Risk Factors Regarding COVID-19 Survey”
23
was used to measure one domain of: Protective behavior against infection.
Both the baseline and pre and post-test surveys measured the perceptions of respondents and recorded answers on a 5-point Likert scale. Both instruments have been published as appendices elsewhere.
19
Reliability tests were performed on the pre and post-test survey. All scales revealed satisfactory reliability (Table 3).
Reliability of study scales.

The primary outcomes for this study were positive and active changes in health-directed behavior, skill and technique acquisition, self-monitoring and insight, health services navigation, sanitation and hygiene, hand hygiene, and protective behavior against infection. The secondary outcomes for this study were improvements in health-related quality of life, social integration and support, and emotional wellbeing.
The specific study hypotheses are:
H1: Multimorbidity risk is higher in women of reproductive years (i) from lower socio-economic background and (ii) who have low health awareness and inadequate health services. H2: There is a greater positive impact of the digital health literacy intervention on the intervention group compared to the control group with regard to improvements in primary outcomes, which are: (i) Health-directed behavior, (ii) Skill and technique acquisition, (iii) Self-monitoring and insight, (iv) Health services navigation, (v) Sanitation and hygiene, (vi) Hand hygiene, and (vii) Protective behavior against infection. H3: There is a greater positive impact of the digital health literacy intervention on the intervention group compared to the control group with regard to improvements in secondary outcomes, which are: (i) Health-related quality of life, (ii) Social integration and support, and (iii) Emotional wellbeing.
Data analysis
Both the baseline and pre and post-test data were analyzed using descriptive statistics and bivariate odds ratios (OR). At the first step, univariate logistic regression was used to determine the predictors of multimorbidity among participants. The independent variable was multimorbidity prevalence, defined as more than two chronic diseases in participants. The dependent variables included socio-demographic characteristics, household characteristics, and health-related questions. At the second step, multivariate logistic regression was applied, holding participant's age, education, and household income constant.
With regard to the pre and post-test data, we compounded the ten study domains for the analysis and used “improved confidence in managing health” as the independent variable. Based on the Likert scale, responses of “Strongly agree” and “Agree” or “Always” and “Very Often”, depending on the scale, were considered to be improvements in confidence. Improved confidence was coded “1”, whereas no improvement (including categories of “Neutral” and “Sometimes”, depending on the scale) was coded “0”. Multivariate logistic regression was run in order to identify higher confidence in managing health following the intervention in the intervention versus control group. IBM SPSS Statistics 25.0 was used for all analyses. The level of significance was assigned at p < 0.05. Confidence intervals (CI) for OR have also been reported. There was no missing data, as the responses were filled with assistance of CHWs. An intention-to-treat analysis was undertaken.
Results
The flowchart of participant recruitment and retention is shown in Figure 2. The study started in February 2021 and ended by May 2021. A total of 1010 women were approached for participation in the study, with 820 agreeing to participate. Though all 820 completed the baseline data, only 793 agreed to participate in the intervention. The control and intervention participants at pre-test stood at 405 and 388 respectively, whereas after three months 388 and 360 participants completed the post-test survey, respectively. The dropout of 17 members from the control group was due to inability to contact women at their homes despite three visits, with reasons by family members reporting that the women were visiting relatives. The dropout of 28 participants from the intervention group was due to: (i) unwillingness to continue with the intervention due to time needed for home and child care, (ii) traveling to visit relatives and family, and (iii) not being able to continue due to revocation of permission from family or husband.
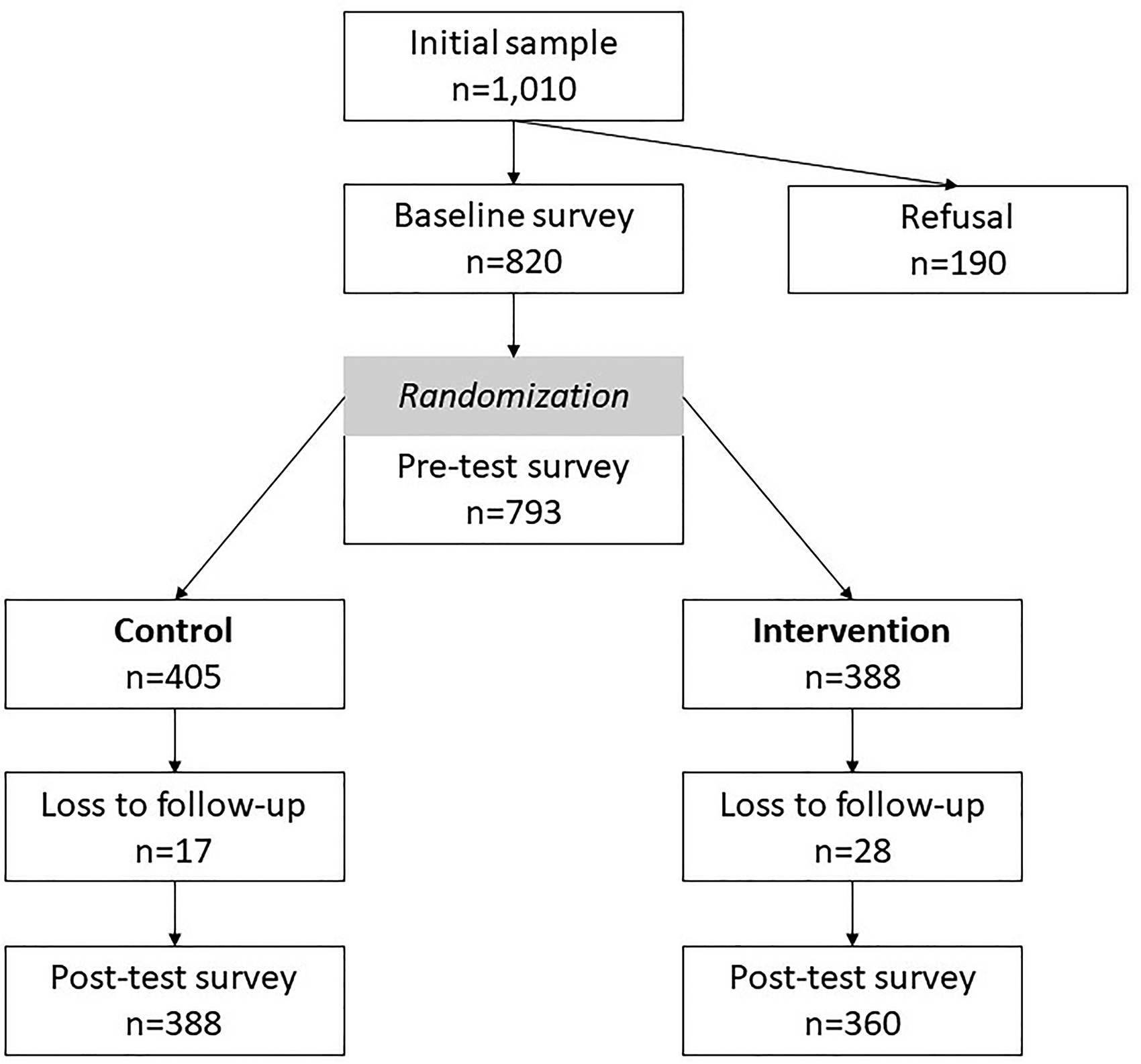
Participant flow for study.
Sociodemographic characteristics at baseline
The majority of the sample is between 16 and 39 years (64.4%), and illiterate (39.6%) or has only received primary schooling up to grade 5 (25.1%). Nearly all participants belong to poor households. Comparable to the population density within Pakistan, the majority of study participants are from Punjab (79.8%) and 20.1% are from KPK province. The majority is unemployed (65.5%) and living in rented houses (72.9%). A total of 35.1% have a mobile phone with internet.
With regard to health characteristics, nearly all sampled women had no health insurance (92.1%) or savings (95.1%). A large majority has taken a loan in the last 5 years (89.0%) and 35.9% suffer from multimorbidity. Nearly half of the sample (41.1%) suffered from a mental health challenges in the previous 12 months and 72.3% perceived problems with physical mobility due to ill-health. Almost 80% suffered from some health challenge in the previous 12 months and almost 70% had undertaken some medical test for health issues. A large proportion has not received any information or only irregular information about health (52.0%) and nutrition and food safety (30%). More than half of participants was not taking the prescribed medicines or multivitamins advised to them by consultants (59.5%). The characteristics at baseline and pre-test are shown in Supplementary File 2.
Predictors of multimorbidity
Multivariate regression analysis of baseline data (Table 4) revealed that women from KPK are at higher risk of multimorbidity (AOR = 1.71; 95% CI: 1.19–2.45). Women who are unemployed (AOR = 1.46; 95% CI: 1.02–2.90) were also at higher risk. Furthermore, women who had taken a loan in the previous five years (AOR = 2.21; 95% CI: 1.40–3.48) or who faced unplanned hospitalization (AOR = 2.39; 95% CI: 1.62–3.52) are also at higher risk of suffering from multimorbidity. Suffered from mental health symptoms in the last 12 months (AOR = 3.18; 95% CI: 2.29–4.42) as well as lack of information and awareness about medical issues (AOR 2.23; 95% CI 1.32–3.79) and nutrition and food safety (AOR 1.84; 95% CI 1.31–2.58) are also predictors for multimorbidity.
Simple bivariate logistic regression for predictors of multimorbidity amongst women of reproductive years (n = 820).
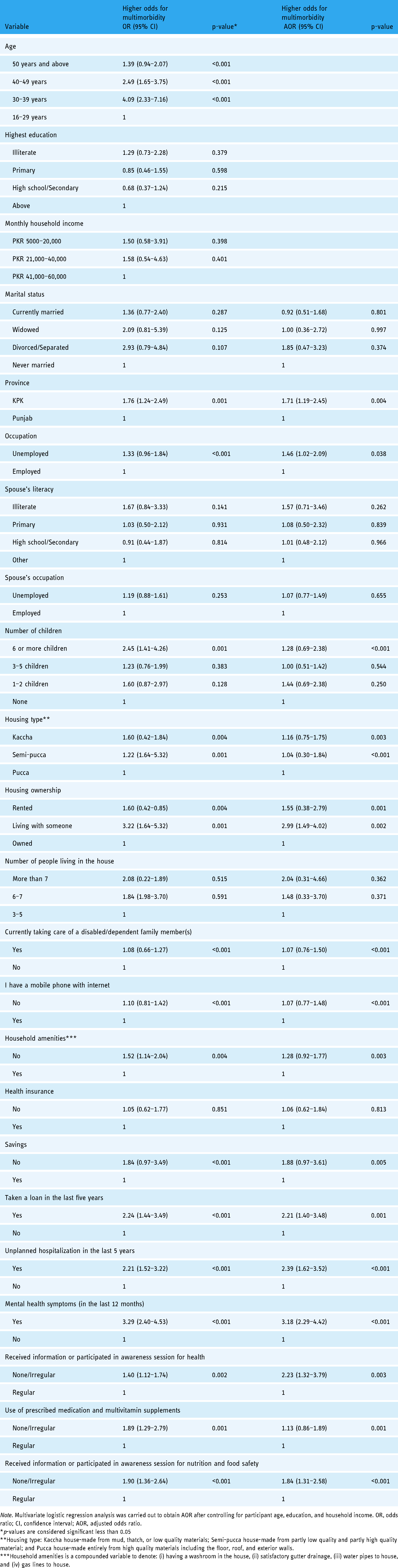
Note. Multivariate logistic regression analysis was carried out to obtain AOR after controlling for participant age, education, and household income. OR, odds ratio; CI, confidence interval; AOR, adjusted odds ratio.
*p-values are considered significant less than 0.05
**Housing type: Kaccha house-made from mud, thatch, or low quality materials; Semi-pucca house-made from partly low quality and partly high quality material; and Pucca house-made entirely from high quality materials including the floor, roof, and exterior walls.
***Household amenities is a compounded variable to denote: (i) having a washroom in the house, (ii) satisfactory gutter drainage, (iii) water pipes to house, and (iv) gas lines to house.
Pre- and post-test for control and intervention group
The pre and post-test results in terms of descriptive percentages of the respective study domains highlight that both the control and intervention group show improvements following the intervention (Table 5). Chi-square results after cross tabulating with the independent variable of “improved confidence in managing health” showed significant associations for all ten study domains.
Participant improvement in measured domains at post-test (n = 748)

Multivariate regression results of the control versus intervention group are presented in Table 6. The control group showed significantly higher odds of confidence in managing health with respect to three domains: (i) Health-directed behavior (AOR = 1.73; 95% CI: 1.13–2.63); (ii) Health services navigation (AOR = 2.29; 95% CI: 1.34–3.92); and (iii) Sanitation and hygiene (AOR = 4.06; 95% CI: 2.94–7.44). Comparatively, the intervention group showed higher odds of confidence in managing health also in three—although different—domains: (i) Skill and technique acquisition (AOR = 2.21; 95% CI: 1.01–4.84); (ii) Self-monitoring and insight (AOR = 2.97; 95% CI: 1.29–6.80); and (iii) Sanitation and hygiene (AOR = 1.42; 95% CI: 1.07–1.93).
Likelihood of higher confidence in managing health following the intervention in both the control and intervention groups (n = 748)

Note. Multivariate regression has been calculated while controlling for variables of age, education, income, region, occupation, and number of children. AOR, adjusted odds ratio; CI, confidence interval.
*Adjusted Odds Ratios (OR) and 95% confidence intervals (CI).
**p-values are considered significant below vales of 0.05.
Discussion
We found that more than one-third of women of reproductive years suffer from multimorbidity. Other studies have highlighted that unless developing countries prioritize multimorbidity detection and management at primary level, health costs and disease burden would increase. 24 In addition, multimorbidity in women of reproductive years may be a reason for unfavorable maternal and child health outcomes, 25 which is already a major health predicament in the region. 26
After adjusting for age, education, and household income, it was confirmed that predictors for multimorbidity include unemployment and unfavorable household characteristics such as not having amenities like water supply, gas, and gutter drainage. In addition, living in rented houses and living in houses made of non-permanent material are also predictors of multimorbidity. Other research confirms that joblessness and low pay 27 as well as unfavorable household characteristics 28 contribute to multimorbidity. Women who have more than six children and are taking care of one or more physically dependent family members are also at higher risk. Other research suggests that a combination of physical, psychological and social morbidities in women, post childbirth, prevents them from taking care of their health, thus contributing to greater risk of multimorbidity. 29
When people do not have access to health information through smartphones, internet, television and radio, it contributes to higher risk of multimorbidity and prevents effective management of self-health. 30 Lack of access to health centers and barriers to geographical mobility can also extend health conditions or worsen multimorbidity. 31 Women from conservative and poorer regions, particularly South Asia, have higher caregiver burdens which prevents them from having the time and energy needed for managing health. 32
Our study indicates that women without savings, who had taken a loan in the last 5 years, and who are not taking their prescribed medicines or multivitamins are also at higher risk of multimorbidity. Previous research has shown that when women have more finances and savings, they are better able to manage health problems and prevent development of multimorbidity or chronic disease. 33 We also found that women who suffer from mental health problems or had experienced unplanned hospitalization in the last five years are at higher risk of multimorbidity. Previous research confirms the relationship between multimorbidity and higher risk of unplanned hospitalization. 34 Similarly, there is a complex relationship between multimorbidity and mental health, especially with respect to underprivileged patients belonging to regions where mental health is not prioritized. 35
The second and third hypotheses of this study are partially proven correct. Both the control and intervention groups experienced significant improvements after the intervention in the area of sanitation and hygiene. The results imply that the health literacy booklet is a valuable literacy intervention for disadvantaged and semi-literate or illiterate populations. Women from low socio-economic backgrounds are known to benefit from written and printed material to improve health education and awareness as it helps in retention of information. 36 In addition, health literacy booklets are useful in sharing information and communicating with household and family members. The intervention group, compared to the control group, experienced significant improvement after the intervention in the domain areas of skill and technique acquisition as well as self-monitoring and insight. Other research reveals that interventions to improve self-management and monitoring of health in women empower them to believe that their health and wellbeing is in their control. 37 Such interventions can have long-run benefits of improving early detection and even providing support to family and children for health management and monitoring.
The control group, compared to the intervention group, experienced significant improvements after the intervention in the domain areas of health-directed behavior and health services navigation. There can be numerous reasons for the improvement in the control group, the main being the impact of the health literacy booklet as discussed above. Also, participants in the control group volunteered to participate in the study and thus were motivated to show commitment to retaining information from the booklet and show improvement in health. Given that the CHWs were from the same community as the participants, there may also be a case of social desirability bias, where participants felt compelled to respond positively. 38 We were unable to separate the intervention and control group who lived in the same community and the CHWs were delivering services to both intervention and control groups. Thus, contamination may also be an explanation for improved results in the control group.
There is concern that the intervention group did not show any significant improvement in the two domains of hand hygiene and protective behavior against coronavirus infection. Results imply that women are not confident about the management of infection and that they may still be uncertain of infection control practices due to mixed messages from different sources, such as religious and community leaders and government sources. 39 Also, this intervention was delivered during the second peak of the coronavirus in Pakistan, and it may be that a lot of people still face confusion and uncertainty about the disease which has impacted results. Women of the region are heavily influenced by social norms and cultural attitudes with respect to management of infection and thus may be less confident about international guidelines for infection control practices. 40 In lieu of this, we believe there is a critical need for collective mobilization in supporting education for infection prevention and to target whole families, especially the heads of households. 41
Furthermore, the intervention group did not show any significant improvement in health-directed behavior and health services navigation. Research suggests that improvements in women's health in South Asia are highly dependent on multiple external factors, such as type of family, in-laws, and husband, 42 poverty and financial situation, geographical mobility and transport access, 43 and public sector health services and health insurance. 44 Similarly, health service navigation is dependent on mobility and service outreach by the public sector at community-level. Sampled women in our study belong to conservative regions with distant access to public sector services. Deriving from this, we must recognize that though digital health literacy interventions are critically needed, they must be partnered with an adequate social protection floor in order to help women translate health literacy to satisfactory health behaviors and management. 45
Secondary outcomes of the study—which have been health-related quality of life, social integration and support, and emotional wellbeing—show no significant improvement. The results confirm that these areas need more attention for intervention delivery and also collective stakeholder support. Overall, only three out of ten domains showed improvements in the intervention group. Results highlight the difficulties in developing successful interventions for women of reproductive years from disadvantaged backgrounds. 46 However, our digital literacy intervention has the benefit of assistance of CHWs from within the community, which encouraged participation and response of women from conservative and semi-literate backgrounds.
Limitations
Limitations of the study include selection bias. We were unable to sample all provinces of Pakistan due to a lack of permission and safety issues. We were unable to sample more women due to lack of funding and time. Also, our intervention was planned for three months and the post-test was taken immediately after the intervention ended. Future studies may benefit from longer intervention periods which may show the long-term impact. As participants could not be blinded, some results may be due to desirability bias. Furthermore, this study was limited to participant's perceived responses. For future studies, we recommend baseline clinical assessment and the measurement of clinical outcomes post the intervention.
Two main findings communicated by CHWs with regard to participant's experience was that: (i) women did not want to share their medical issues with family members, as it was associated with cultural shame; (ii) they did not want to ask male family members to take them for treatment and checkup due to financial burden and time issues; and (iii) a few participants initially did not want to see the video as they believed the screen will strain their eyes and give them a headache. For future studies, we recommend holding interventions for awareness with husbands and family members to inculcate importance for women's health and seeking referral access from specialists outside the home. We also recommend free health services at tertiary level for disadvantaged women and transport stipends for health visitation to strengthen the link between primary to tertiary level health access.
Some of the main challenges that the CHWs faced included: (i) need for higher stipend for their efforts and work, (ii) internet connectivity issues, (iii) need for additional training in speech confidence and some basic level of counseling support, and (iv) inability to manage or deny requests from other women in the community to attend the group sessions. With regard to the latter, these women were from either the control group or non-participants of the study, thus leading to problems of contamination and also extra work hours for CHWs, as larger group sessions ended up lasting three to four hours. We recommend additional support for training of CHWs and partnership with third party training centers to deliver digital training to health workers for communication and informal counseling. Lastly, Pakistan needs good internet access across the nation for digital health literacy interventions to be effective.
Conclusion
The results of this study reveal the critical need to integrate services for detection, prevention and management of multimorbidity at primary level for women of reproductive years in Pakistan. The study also confirms the value and benefits of digital health literacy interventions. It is recommended that government and private bodies collaborate to fund and strengthen primary care services, specifically for health literacy and multimorbidity management across the country. Collaborative efforts would support comprehensive outreach, financial sustainability, cross monitoring, continued assessment of impact, and policy development over the long-run. Finally, services must be delivered by recruitment and training of supplementary community health workforce at primary level and integrated with the existing LHW services for greater impact.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076221144506 - Supplemental material for Impact of a digital health literacy intervention and risk predictors for multimorbidity among poor women of reproductive years: Results of a randomized-controlled trial
Supplemental material, sj-docx-1-dhj-10.1177_20552076221144506 for Impact of a digital health literacy intervention and risk predictors for multimorbidity among poor women of reproductive years: Results of a randomized-controlled trial by Sara Rizvi Jafree, Anam Muzammil, Syeda Khadija Burhan, Nadia Bukhari and Florian Fischer in Digital Health
Supplemental Material
sj-docx-2-dhj-10.1177_20552076221144506 - Supplemental material for Impact of a digital health literacy intervention and risk predictors for multimorbidity among poor women of reproductive years: Results of a randomized-controlled trial
Supplemental material, sj-docx-2-dhj-10.1177_20552076221144506 for Impact of a digital health literacy intervention and risk predictors for multimorbidity among poor women of reproductive years: Results of a randomized-controlled trial by Sara Rizvi Jafree, Anam Muzammil, Syeda Khadija Burhan, Nadia Bukhari and Florian Fischer in Digital Health
Supplemental Material
sj-docx-3-dhj-10.1177_20552076221144506 - Supplemental material for Impact of a digital health literacy intervention and risk predictors for multimorbidity among poor women of reproductive years: Results of a randomized-controlled trial
Supplemental material, sj-docx-3-dhj-10.1177_20552076221144506 for Impact of a digital health literacy intervention and risk predictors for multimorbidity among poor women of reproductive years: Results of a randomized-controlled trial by Sara Rizvi Jafree, Anam Muzammil, Syeda Khadija Burhan, Nadia Bukhari and Florian Fischer in Digital Health
Supplemental Material
sj-docx-4-dhj-10.1177_20552076221144506 - Supplemental material for Impact of a digital health literacy intervention and risk predictors for multimorbidity among poor women of reproductive years: Results of a randomized-controlled trial
Supplemental material, sj-docx-4-dhj-10.1177_20552076221144506 for Impact of a digital health literacy intervention and risk predictors for multimorbidity among poor women of reproductive years: Results of a randomized-controlled trial by Sara Rizvi Jafree, Anam Muzammil, Syeda Khadija Burhan, Nadia Bukhari and Florian Fischer in Digital Health
Supplemental Material
sj-docx-5-dhj-10.1177_20552076221144506 - Supplemental material for Impact of a digital health literacy intervention and risk predictors for multimorbidity among poor women of reproductive years: Results of a randomized-controlled trial
Supplemental material, sj-docx-5-dhj-10.1177_20552076221144506 for Impact of a digital health literacy intervention and risk predictors for multimorbidity among poor women of reproductive years: Results of a randomized-controlled trial by Sara Rizvi Jafree, Anam Muzammil, Syeda Khadija Burhan, Nadia Bukhari and Florian Fischer in Digital Health
Footnotes
Acknowledgments
The authors gratefully acknowledge the contribution of all participants, their family members, counselors and community health workers who participated in this project. We would also like to thank the research assistants for support in data management including Kundan Raza, Amna Maryam, and Hania Afzal. The following people are acknowledged for assistance in data collection and gaining permissions: Sanam Jhatial, Tanzeela Naz, and Arzu Moosvi. We also appreciate the support of Mr Adeel Ahmad, from the University of the Punjab, Dr Sobia Javed and Dr Sabeen Fatima Haque. Finally, we are indebted to the (i) 18 District Team Leaders for this project: Samina Jafri, Zahida Zubaida, Noureen Irfan, Zareena Anjum, Saima Noureen, Irshad Bibi, Tahira Batool, Shamim Akhtar, Anila Shakeela, Nargis Parveen, Samina Tabasum, Nasreen Akhtar, Rubina Shaheen, Nabila Anjum, Shazia Maqbool, Shakeela Kousar, Sayeeda Rafia Batool, Shazia Kanwal; and the (ii) 6 Field Coordinators for each district: Sajid Iqbal, Khalid Bashir, Sidra Kashif, Sehrish Khan, Shazia Begum, and Arshad Mohammad. We also must thank community members who helped in providing confirmation about translations and in coordinating group sessions during the intervention: Anila Nazish, Kalsoom Anwar, Shahnaz Akthar, Sughra Bibi, Asma Naseer, and Safia Arbai.
Contributorship
SRJ drafted this article and was principal investigator for the project. AM, SKB, and NB supervised the data collection. FF provided supervision for the entire project and helped draft the manuscript. AM provided support for baseline data analysis and SKB provided support for the pre and post-test data analysis. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was obtained from the Research Ethics Board of Forman Christian College University, Lahore, Pakistan (2010–044).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by doctHERS, in partnership with University of Health Sciences (UHS), Punjab Population Innovation Fund (PPIF), Women Chamber of Commerce and Industry (WCCI) and Rural Support Programmes Network (RSPN), under their joint agreement to provide maternal, child, health and family planning services via telemedicine to underprivileged women of Pakistan. The contact point for doctHERS is asher@docthers.com. The funds have been used for the following expenses: digital assets (smartphone, Wi-Fi and video development), stipend for community healthcare workers for field visits and intervention delivery. The principal and co-investigators did not receive a salary for this project. The funding body was not involved in study design, data management, or interpretation of the data.
Guarantor
FF
Trial registration
NCT04603092
Supplemental material
Supplemental material for this article is available online.
Appendix A
Appendix B
Health litearcy booklet provided to control and intervention group
Appendix C
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.