
Abstract
Adapted physical activity (PA) programs benefit patients with non‑communicable diseases, but access barriers limit reach. Hybrid programs mixing in‑person and telehealth sessions may overcome these constraints. The purpose of this study was to evaluate the acceptability and effectiveness of a 3‑month hybrid APA program compared with usual face‑to‑face care and to examine whether benefits persist up to 36 months. Twenty patients with chronic diseases completed an APA program that began onsite and transitioned to videoconference plus home exercises. A historical cohort of 100 patients who received the standard onsite program and matched baseline characteristics served as controls. Changes in self-reported PA, physical capacities, and body composition of patients from both programs were measured at baseline and 3, 6, 12, 4, 36 months and analyzed using random-effect models. Adherence and satisfaction were also evaluated. Participants in the hybrid program showed high adherence and acceptability to the program, significant improvements in cardiorespiratory capacity, and reported increased PA levels. Overall effect sizes between the two groups were small. Importantly, the effects of both programs on these variables persisted 3 months after the end of the program with meaningful effect sizes and up to 33 months after the end of the program for 6 MWT. However, dropout rates during follow-up were high. Despite high acceptability and adherence for most patients of the hybrid group, some patients demonstrated lower participation. In conclusion, a hybrid program including telehealth was feasible, well‑accepted, and produced durable, clinically meaningful gains in cardiorespiratory fitness, and physical activity that matched conventional rehabilitation. Larger randomized trials are warranted to confirm these findings.
Keywords
A hybrid program combining face-to-face and videoconferencing sessions significantly improved cardiorespiratory fitness and self-reported physical activity, with effects sustained 3 months post-intervention—and maintained up to 33 months for the 6-minute walk test.
Effect sizes between the hybrid and traditional face-to-face programs were small, suggesting that hybrid delivery may be a viable and efficient alternative to standard supervised rehabilitation programs.
While overall acceptability and adherence to the hybrid program were high, some participants showed lower engagement, underscoring the need for screening tools to personalize program allocation and optimize individual treatment.
Introduction
The burden of noncommunicable diseases (NCDs), including cardiovascular diseases, cancers, type 2 diabetes mellitus (T2DM), and chronic obstructive pulmonary diseases (COPD), is today a priority public health issue, contributing to 70% of all deaths worldwide. 1 If the roots of these pathologies are complex and multifactorial, physical inactivity and sedentary behaviors are considered major factors in the appearance and development of NCDs. 2 Given the significant role of physical activity (PA) in mitigating the risk of developing complications related to NCDs3 -6 and limiting the progression of these pathologies,7,8 PA programs stand as a cornerstone in the management of these conditions.
In consequence, patients with NCDs can usually benefit from supervised PA programs tailored to their abilities and health conditions, known as adapted physical activity (APA). These programs aim to enhance functional capacity and muscle strength without having detrimental effects or complications on disease progression. 9 APA programs are based on the WHO PA’s recommendations for health, provided by qualified personnel, and incorporate motivational and educational elements designed to foster a healthy lifestyle. In addition to its potential benefits on the PA of individuals, APA has demonstrated efficacy in improving physical functioning, alleviating pain severity, mitigating fatigue, and enhancing psychological and social well-being.10 -13
However, while these programs are considered the gold standard, they face several limitations for both patients and the healthcare system. On the one hand, the adherence and observance rates of APA programs are limited14,15 as these programs can be difficult to access for patients, due to lack of availability on the scheduled sessions, lack of economic means, climatic constraints, limited knowledge, perceived difficulty or discomfort of exercise, competing family responsibilities, or geographical distance from the care center.16 -18 These concerns are exacerbated in rural and low-income areas and during the COVID-19 outbreak, 19 which had a direct impact on the rehabilitation of patients with NCDs. 20 On the other hand, as these face-to-face sessions require qualified professionals, are provided at specific times and within clinics or hospitals, partitioners, hospitals, and clinics are overloaded, waiting lists for care appear, and the current system cannot handle the rising number of patients with NCDs who need APA.
Therefore, in a context of decreasing financial resources for patient care and increased constraints, 21 there is an urgent need to develop and test more effective and cost-effective therapies. In this vein, leveraging technologies and e-health platforms emerges as a promising strategy to enhance care accessibility. Telerehabilitation and telehealth represent modalities for delivering services to patients and clinicians by minimizing the barriers related to distance, time, and costs.22,23 Several devices and approaches have been used to provide APA at patients’ homes. First, unsupervised home training with or without video content (eg, on VHS, DVD, or Internet) or semi-supervised training with phone calls to monitor compliance and participants’ progression have been proposed. More recently, remote-supervised APA programs have been developed using videoconference software.
Telehealth has emerged as a rapidly expanding safe alternative 24 service delivery model for managing chronic diseases and has been tested in several studies. A recent systematic review and meta-analysis conducted by Brown et al 25 revealed that telehealth interventions including videoconferencing sessions appear to be feasible and effective for improving exercise capacity and quality of life. Interestingly, the effect was statistically significant when compared to both non-exercising and exercising control groups, with a standardized mean difference (SMD) of .24 (95% CI: .06-.43) for the latter comparison.
However, the authors of this review emphasized a moderate certainty of effect due to the risk of bias in the included studies and the limited number of controlled trials. Indeed, most evaluations of telehealth interventions have to date been conducted through single-group designs, thereby precluding rigorous comparisons with existing modalities such as supervised physical activity programs. Furthermore, no studies included in this review have assessed the sustainability of these programs’ effects, despite the crucial challenge associated with the long-term effectiveness of interventions in promoting PA.
It is essential to scientifically and rigorously test the use of this type of program in comparison with usual care before democratizing its use. In this regard, randomized controlled trials represent the gold standard for assessing the efficacy and effectiveness of digital health tools.26,27 However, the implementation of RCTs can entail significant time and financial resources. 28 Hence, pilot studies and case studies play a pivotal role in providing preliminary insights and informing the design of larger-scale trials.
In addition, previous studies always tested full digital telehealth interventions. Yet, hybrid programs combining on-site rehabilitation visits and real-time videoconferencing may optimize the benefits of the intervention and allow efficient use of resources. 21 In particular, hybrid programs could be interesting to demonstrate the right movement to the patients and to have a first in-person meeting between the coach and the participant before online sessions. Considering the pivotal role of the APA teacher in facilitating links, supervising the exchanges, and thus, ensuring the conviviality of the sessions and the need of patients to perceive programs as accessible to engage in telehealth programs, 29 these hybrid programs could be helpful. Finally, including long-term follow-up is essential in order to evaluate the sustainability of such programs.
To answer these two research questions, the present case-control study—initiated in the context of the first lockdown due to the COVID-19 pandemic in France (Spring 2020)—aimed to evaluate the acceptability and effectiveness of a hybrid program combining initial face-to-face sessions followed by telehealth, on self-reported PA, cardiorespiratory fitness, and muscular capacities. These variables were assessed before and after the 3-month program, with follow-up measures conducted over the 33 months following the program, for a total of 36 months and six experimental visits. The second objective of this pilot study was to compare the efficacy of this program in comparison to the usual care of the same hospital (ie, face-to-face supervised PA) using a database of previous patients, who were also followed for 36 months.
We hypothesized that the hybrid program would have good acceptability among patients, with good continuity between face-to-face sessions and online sessions. Furthermore, we anticipated that it could potentially be as effective as, if not more effective, than the usual care.
Methods
Participants
Between January and March 2020, we proposed to 20 patients (mean age = 54.3 ± 13.4 years; 65% women; BMI = 30.6 ± 7.7 kg/m²) involved in a supervised APA program at the University Hospital of Clermont–Ferrand (France), to finish their program remotely with telecoaching sessions. To be included in the present study, participants must have had at least 30% of the planned sessions remaining. In this sample, participants were treated for obesity (n = 9), cancer (n = 5), COPD (n = 3), and T2DM (n = 3).
To test the effectiveness of this program in comparison to the usual care, we selected 100 patients (mean age = 54.8 ± 13.8 years; 65% women; BMI = 31.8 ± 7.6 kg/m²) in an anonymized database of 473 individuals who had already completed a 3-month face-to-face program in the same conditions (ie, same coaches, same evaluators, and the same planned number of sessions) at the University Hospital of Clermont-Ferrand between 2015 and 2020. To make this comparison relevant, we randomly selected the participants in the database on the basis of matching age, sex, baseline PA, and baseline BMI between both the hybrid group and the face-to-face group. The selected participants were treated for obesity (n = 49), cancer (n = 8), COPD (n = 20), and T2DM (n = 23).
Procedure
Patients of both groups had stable conditions and an APA prescription from their referring physician or specialist. They were tested at baseline (M0), at the end of the program (M3), and during four additional follow-up visits (M6, M12, M24, M36). Participants were voluntary patients who were required to be covered by social health security and had no prior experience with APA interventions. The presence of any of the following criteria resulted in exclusion: a medical or surgical history deemed incompatible with the study, unstable psychiatric conditions, pregnancy or breastfeeding, disability or contraindications to PA, progressive cardiovascular or neoplastic diseases, known neuromuscular pathologies (eg, myopathy, myasthenia, rhabdomyolysis, paraplegia, hemiplegia), refusal to provide written informed consent or participation in another study. Eligible patients were invited to participate during a medical consultation prior to baseline assessments, where the inclusion process was finalized. As this study was a pilot control case, blinding of outcome assessments was not implemented, as the APA coach responsible for assessing participants’ outcomes was aware of their program assignment. Participants of the hybrid program must have attended at least one face-to-face and one videoconference session to be included in the analyses. The study was approved by local Ethics Committee (IRB00013412, “CHU de Clermont Ferrand IRB #1,” IRB 2024-CF247) with compliance to the French policy of individual data protection. All data were obtained during the patient care path. Written informed consent was obtained from all participants and all the used and analyzed information was obtained exclusively from anonymous data (CNIL no. 0164).
Intervention Content
The usual care of the University Hospital of Clermont-Ferrand consisted of a 3-month program of face-to-face APA, 3 sessions a week on non-consecutive days, for a total of 36 sessions. These individual sessions were composed of a warm-up, followed by 50 minutes of endurance exercises, muscle strengthening exercises, and stretching—all supervised by an APA coach. Aerobic and resistance exercises were performed in a circuit organized as a row of six exercise stations (3 aerobic and 3 resistance exercises). Aerobic exercises were performed at 50% of VO2max the first week and the intensity was gradually increased by 10% every 2 weeks to target at least 80% of VO2max over the last 9 weeks. For resistance exercises, patients performed a single set of 8 to 12 repetitions of unloaded exercises the first week and the number of sets was gradually increased to 3. These exercises were performed at 50% of 1RM during the first week. Then the load was gradually increased by 10% every 2 weeks, and remained at 80% of 1RM over the last 5 weeks. The patients from the database group benefited from this program.
In the hybrid program, participants started with the same content described above (ie, supervised face-to-face PA). These sessions were then substituted by a telehealth program combining exercises in autonomy and live videoconferencing sessions. In the telehealth part, patients were proposed each week (a) paper or video content with exercises to be done in autonomy comprising each time 3 levels of difficulty for a duration of 40 to 50 minutes and (b) collective live sessions by videoconferencing lasting 45 minutes to 1 hour. More specifically, these sessions were similarly constructed to those conducted usually in face-to-face using patients’ available material, and were proposed several times a week by an APA coach. These videoconference sessions were open access for patients, meaning they could participate in more than 36 sessions in total. Online sessions were conducted using Zoom software (Zoom, USA), with connection links provided to each participant for easy access. If a participant was unable to attend a session, a recorded version was made available. Additionally, participants were offered video sessions on YouTube to practice autonomously. These videos were specifically designed by the coach from the Clermont-Ferrand University Hospital to complement the program. To further support engagement, a 15 to 30-minute telephone interview was conducted with each participant weekly. Compliance and progression to the exercises performed in autonomy were monitored by the coaches each weekend via phone calls. This hybrid program lasted 3 months and comported on average 50% of online sessions (range = 40%-70%).
Measures
The 6 experimental visits were conducted in the same conditions for both groups and measured physical characteristics, body composition, self-reported PA, and physical capacities of patients. All measures were performed at the same time of the day to control for circadian variations in the University Hospital of Clermont-Ferrand.
Anthropometric Measurements and Body Composition
Body mass was measured to the nearest 0.1 kg using a calibrated digital scale, and height was measured to the nearest 0.1 cm using a wall-mounted stadiometer. BMI was calculated as body mass (kg) divided by height squared (m2). Body composition was assessed by bioelectrical impedance analysis (BODYSCAN QuadScan 4000, Belgium).
Self-Reported PA
PA and sedentary behaviors during transportation time, leisure time, and work time were assessed using the Global Physical Activity Questionnaire (GPAQ). 30
Physical Capacities
Muscular strength of the upper limbs was assessed by a series of three handgrip test measurements for right and left hands, in the seated position. The best performance measured for each hand via dynamometer (Takei Grip-D, Takei, Japan) was conserved. 31 Aerobic endurance was estimated via the 10 Meter Walk Test (10 MWT) which measures the shortest time to walk 10 m in a standardized corridor. 32 Two measurements were conducted and only the best performance was conserved. Functional capacity at sub-maximum intensity was assessed via the 6-minute walk test (6 MWT), which measures the distance covered in meters in a standardized 30-m-long corridor. 33
Acceptability and Satisfaction
Satisfaction with the hybrid program was assessed with an ad-hoc questionnaire at T1. A first question aimed to evaluate if the patients found the addition of videoconferencing sessions beneficial with a single item: “Did you find that the videoconferencing sessions had a positive, negative, or no effect on your program?” A second question assessed what type of program patients would prefer to do if they had the opportunity in the future with the following item: “If you had to redo a physical activity program, would you prefer a full face-to-face, totally remote, or hybrid program with one face-to-face session per week?”
Statistical Analyses
Sample Size and Power Analysis
As this study is a pilot with a control case design, the sample size was limited by the recruitment capacity at the time of enrollment. We were able to offer the hybrid program to 20 participants. Then, we conducted a sensitivity power analysis to evaluate the probability of a Type II error for effects of interest. 34 With a sample size of 20 participants in the hybrid group, we can demonstrate a pre/post difference equivalent to an effect size of d = .66 for 80% power, a 2-sided type I error at .05, and 2 measurements with a correlation of .5 among repeated measures. For the comparison with the database, with 20 participants in the experimental group and 100 participants in the database, we can demonstrate a difference equivalent to an effect size of .7 for 80% power and a 2-sided type I error at .05. Selecting more participants from the database was not associated with an increase in power, so we considered using a 1:5 ratio.
Data Analyses
Continuous data were expressed as means and standard deviations (SD). The normality of the distribution was checked with a Shapiro–Wilk test. We conducted random-effect models with the following fixed effects: time, group (hybrid program vs usual care), and their interaction. Participant effect was considered as random (effect) in order to model between and within-subject variability. The normality of residuals was checked for all models. When appropriate, a logarithmic transformation of the dependent variable was performed. Thus, random-effect models were conducted to assess (1) the effect of time in hybrid program group, (2) the effect of time in the usual care group, and (3) the interaction group × time. Additionally, a separate model was performed to control the number of videoconferencing sessions attended in the hybrid group, and another model was conducted incorporating follow-up data from baseline (M0) to 36 months (M36). For non-repeated data, the 2 groups were compared for quantitative variables using Student t-test or Mann–Whitney test when the assumptions of t-test were not met. The study of homoscedasticity was studied using equality of variance Fisher–Snedecor test. For categorical variables, Chi-squared and Fisher’s exact test were applied. Differences were considered statistically significant at P < .05. As analyses were exploratory, the individual P-values have been reported without applying systematically mathematical correction according to several works reported in the literature,35,36 but with a specific attention paid on the magnitude of differences and to the clinical relevance expressed using effect-size and 95% confidence interval. 37 Statistical analyses were performed using Stata software (version 15, StataCorp, College Station, TX, USA). The data of the present study is available on Open Science Framework (https://osf.io/a89zw/).
Patient and Public Involvement
Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Results
Figure 1 displays the number of participants who completed assessments at each time point. Notable dropout rates were observed in both groups during the follow-up periods.
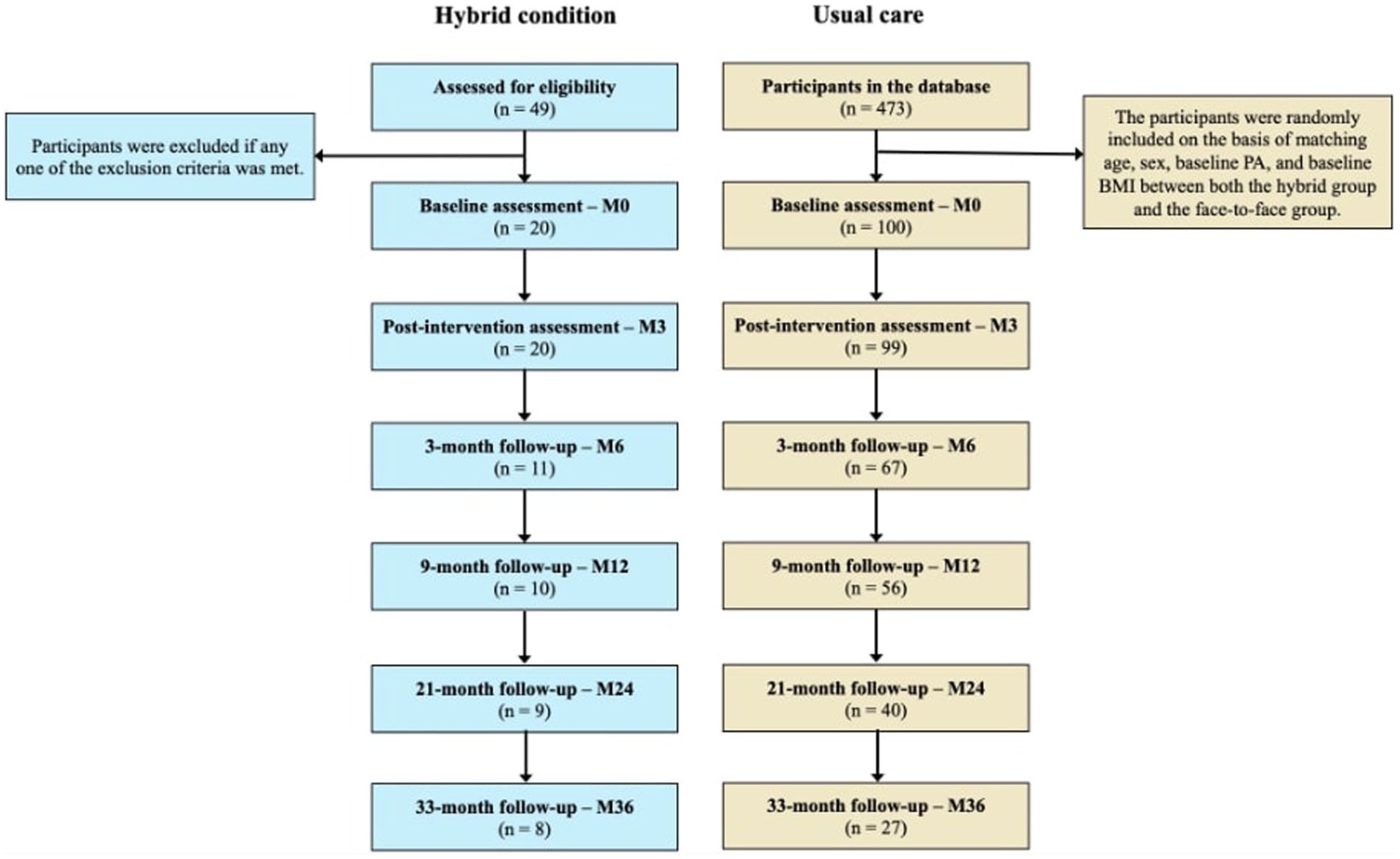
Study flow diagram.
Acceptability and Adherence to the Hybrid Program
Adherence
All included participants completed the study. Among the 20 patients, good continuity between face-to-face and telehealth sessions was observed for 19 patients, with a ratio of attended face-to-face sessions to attended videoconference sessions ranging from .5 to 2. In other words, aside from 1 patient who experienced a marked reduction in session attendance, the transition to digital sessions did not appear to disrupt adherence. However, participation rates varied among patients. If on average these participants have completed 37 sessions (SD = 15.65), some patients completed more sessions (ie, videoconferencing sessions were in self-service) while others showed poorer participation. Specifically, 11 patients completed more than 36 sessions (M = 49, range = 39-60), 5 patients completed between 18 and 36 sessions (M = 30, range = 25-35), and 4 patients completed less than 18 sessions (M = 14, range = 10-17).
Satisfaction
Overall, patients reported a high level of satisfaction with the program. Responses from the ad hoc questionnaire revealed that 75% (n = 15) of patients found the videoconferencing sessions to have a positive effect on the program’s benefits, 15% (n = 3) found no differences between face-to-face and online sessions, and 10% (n = 2) found a negative impact of telecoaching sessions. The majority of patients (65%, n = 13) expressed a preference for a hybrid program if given the choice, while one patient preferred a fully digital program, and 30% (n = 6) preferred a fully face-to-face program. Notably, patients with the lowest online participation rates were more likely to express a preference for face-to-face sessions.
Safety
Injuries were rare (<5% of the two cohorts). These were mainly flare-ups of osteoarthritis of the knees (ie, gonarthrosis) in obese or overweight subjects who had prior gonarthrosis, all of which resolved spontaneously after 2 weeks’ cessation of training in the lower limbs (continued in the lumbar, abdominal, and upper limbs) and were not group-specific.
Effect of the Programs on Pre/Post Evolution of Clinical Outcomes
Table 1 displays patients’ baseline characteristics stratified by group.
Baseline Demographic and Clinical Characteristics (Mean ± SD).

Participants enrolled in the hybrid program showed significant improvements in their performance on both the 6MWT (+166.75 m, d = 1.66; 95% CI: 1.04-2.28, P < .001) and the 10MWT (+0.11 m/s, d = .68; 95% CI: .06-1.30, P = .027). They also reported performing significantly more PA at the end of the program (+21.47 MET.h/week, d = .77; 95% CI: .15-1.39, P = .002) compared to baseline. The other variables were not significantly impacted by the program (Table 2). The results followed the same trends when the number of videoconferencing sessions performed was controlled—with significant improvements on self-reported PA (P < .001), 6 MWT (P = .019), and 10 MWT (P = .007) performances whereas there was no significant improvement on other outcomes.
Changes in Parameters Before and After the Hybrid Program and the Usual Care (Mean ± SD).

Bold values indicate statistically significant differences and effect sizes (P < 0.05).
On the other hand, participants receiving usual care demonstrated improvements in their performance on the 6 MWT (+39.53 m, d = 1.12; 95% CI: .85, 1.40, P < .001), the 10 MWT (+.09 m/s, d = .83; 95% CI: .55, 1.10, P < .001), and the handgrip test (+1.13 kg, d = .54; 95% CI: .26, .82), P < .001 on the right hand and + 1.54 kg, d = .74; 95% CI: .47, 1.02, P < .001 on the left hand). Weight (−.42 kg, d = −.32; 95% CI: −.60, −.04, P = .023), fat mass (−.56%, d = .83; 95% CI: −1.11, −.56, P < .001), and self-reported physical activity (+10.81 MET.h/week, d = .33; 95% CI: .05, .61, P = .002) were also improved at the end of the program compared to baseline (Table 2).
Effect of the Programs on the Long-Term Evolution of Clinical Outcomes
The follow-up data of patients of both groups are presented in Table 3 with the related effect sizes and 95% confidence interval of changes in Table S1. In the hybrid group, significant differences in the 6 MWT were observed up to M36 (d = 1.71; 95% CI: 1.09, 2.33 at M6 to d = .80; 95% CI: .18, 1.42 at M36), whereas improvements in the 10MWT performance and PA level were statistically significant up to M6 (d = 0.76; 95% CI: .14, 1.38 for the 10 MWT and d = .70; 95% CI: .08, 1.32 for the PA level). Other significant differences appeared over time, but these are likely to be related to the drop-out and diversity of participants’ pathologies, with a small number of participants that provided assessments at the last visits (see Figure 1).
Changes in Parameters for Both Conditions During Follow-Up Periods (Mean ± SD), Elements in Bold Represent Within-Group Significant Differences with M0.

Bold values indicate statistically significant differences and effect sizes (P < 0.05).
In the usual care group, significant improvements were also maintained up to M36 for the 6 MWT (d = .99; 95% CI: .71, 1.27 at M6 to d = .40; 95% CI: .13, .68 at M36), to M12 for the handgrip (d = .42; 95% CI: .15, .70 at M6 and d = .30; 95% CI: .02, .57 at M12 for the right-hand grip) and the 10 MWT (d = .60; 95% CI: .32, .88 at M6 and M12), and to M6 for the PA level (d = .35; 95% CI: .08, .63 at M6). Evolutions in weight, BMI, or fat mass are discontinued, and significant differences could be linked to dropout issues (Figure 1).
The effect sizes for each outcome and each datapoint are available in Table S1 in Supplemental materials.
Comparison Between the Hybrid Program and the Usual Care
Random-effects models revealed a significant interaction group × time on the 6 MWT (d = .24, 95% CI: .04, .43, P = .019). In other words, the pre/post change in the 6MWT performance was significantly higher in the hybrid program compared to the usual care. This interaction was no longer significant in the model with follow-up data. Other group × time interactions on weight (d = .11, 95% CI: −.07, .31, P = .235), fat mass (d = .10, 95% CI: −.10, .29, P = .338), lean mass (d = .06, 95% CI: −0.13, .26, P = .527), hand grip right (d = .10, 95% CI: −.10, .30, P = .313) and left (d = −.16, 95% CI: −.36, .02, P = .093), 10 MWT (d = .02, 95% CI: −.17, .21, P = .840), and self-reported PA (d = .14, 95% CI: −.06, .37, P = .161) outcomes were not significant. There were no significant interactions in the models including follow-up measures.
Discussion
This case-control study aimed to assess the acceptability and long-term effectiveness of a hybrid APA program—integrating 50% of videoconferencing sessions in average and physical exercises in autonomy at home—on PA, body mass, body composition, and physical capacities among patients with NCDs. The majority of patients had great adherence rates and expressed a high level of satisfaction with the hybrid program. However, individuals with lower engagement in online sessions tended to prefer the usual care approach. The pre-post outcome analyses revealed that progressively substituting supervised face-to-face PA sessions with telehealth, was effective to increase total PA and improve cardiorespiratory fitness. Moreover, this improvement in cardiorespiratory fitness was significantly more efficient compared to patients who had completed the supervised 3-month APA program exclusively in face-to-face. Nevertheless, the magnitude of the effects was similar between the two programs. Importantly, the effects of both programs on some variables (6 MWT, 10 MWT, PA level) persisted 3 months after the end of the program with meaningful effect sizes, and up to 33 months after the end of the program for 6 MWT. However, notable dropout rates were observed in both groups during the follow-up periods.
Overall, these findings are consistent with previous meta-analyses suggesting that telerehabilitation and telehealth are feasible with good acceptability among patients, and associated with positive clinical results, even comparable to conventional face-to-face approaches.25,38,39 These results are important considering the health benefits of such physical improvements. Indeed, any gain in cardiorespiratory capacities of 1 MET is accompanied by a 12% reduction in mortality both in healthy individuals and in subjects with NCDs, 40 whether they are between 20 and 65 years old or over 65. 41 In addition, PA plays an essential role in improving physical and mental health and overall quality of life.42,43
A major strength of this study was its extended follow-up period of 36 months. While high dropout rates are an inherent challenge in such long-term designs and limit the generalizability of the present findings, the results provide encouraging evidence for the sustainability of the intervention's effects on cardiorespiratory fitness and self-reported PA. Crucially, many of the most significant health benefits of physical activity—such as reduced risks of cardiovascular disease, cancer, type 2 diabetes, and other chronic conditions—are contingent upon long-term changes in PA. 44 The results suggest the maintenance of PA and clinical benefits over several months post-intervention, which are promising in this line. The decrease in effect sizes over time also highlights the importance of deploying additional intervention doses, also known as boosters. Including various follow-up maintenance and reinforcement strategies such as phone calls, home visits, app-based interactions, or additional sessions, these elements could be an effective strategy for prolonging positive treatment effects. 45
While our results must be treated with caution due to multiple not-corrected comparisons and the small number of patients included, and therefore the fact that we can't rule out the existence of type I and II errors, it is worth noting that the magnitudes of the effects are similar to those of Brown's meta-analysis (ie, around d = .2, 95% CI: .06, .47). Even with these low effect sizes, these results are promising from an interventional point of view, opening new perspectives of care. Indeed, even smaller improvements or equivalence in the effectiveness of e-health interventions in comparison to usual care are important, given the potential reach and economic impact of these interventions. Because of its digital nature and its associated assets as the opportunity to practice easily from home, telehealth interventions can answer the time, cost, and geographical limits of current programs. Moreover, telehealth is an interesting way to provide APA when face-to-face management is impossible (eg, patients with cystic fibrosis).46,47 Lastly, this study introduces a novel approach by proposing a hybrid program that combines face-to-face and telehealth sessions. Patient feedback indicates a favorable reception to this approach, highlighting its potential value in establishing initial patient rapport and providing hands-on guidance before transitioning to remote sessions.
These findings underscore the importance of future investigations aimed at rigorously testing the effectiveness of APA programs integrating telehealth versus usual care through well-powered randomized controlled trials. In particular, conducting equivalence tests considering Minimal Clinically Important Differences (MCID) will be essential to demonstrate the equivalence between the two forms of interventions. Additionally, given the significant disparities in the number of sessions attended by patients in the hybrid group, it will be crucial to examine the determinants explaining optimal engagement in a remote program and develop screening methods to identify individuals who will benefit most from such interventions. Factors such as the motivational profile, 48 the acceptability of the technologies, 49 or some physiological characteristics 50 could play a critical role in determining whether a digital or in-person program would be more appropriate. 51 Finally, if randomized controlled trials confirm the potential of such interventions, future research should investigate the implementation of telehealth and hybrid programs. Addressing challenges such as funding constraints, the training of healthcare professionals, digital accessibility, and organizational readiness will be crucial for successfully scaling remote care. 52
Limitations
This study has several limitations that constrain the conclusions that can be drawn. First, the design was observational without a proper control group or objective measure of PA. Yet, causal inference is not possible and self-reported measures of PA are likely to be overestimated. 53 Future studies should implement randomized controlled designs and objective measures of PA via accelerometers to improve accuracy. Moreover, intervention effects are often non-linear and vary across timescales, making the traditional 7-day measurement bursts used in PA trials insufficient for capturing the true impact of PA programs. 54 Longitudinal intensive assessments and real-world data, can offer more robust evaluation methods of the intervention effect and patterns of responses in time.51,55
Additionally, the temporal sequence of evaluations implies that a selection-history effect may be a potential concern in this context. Also, the sample size was small as this study was a pilot test, which limits generalizability. Furthermore, acceptability was assessed using an ad-hoc questionnaire, which may not fully capture this concept. Complementary qualitative methods, such as think-aloud protocols, interviews, or focus groups, could provide deeper insights into acceptability. 56 Finally, participants were not involved in designing the intervention. Co-creation with end-users is increasingly recognized as a strategy to enhance adherence and effectiveness by tailoring programs to users' specific needs, preferences, and barriers. 57 Future studies should integrate participatory design approaches to optimize intervention outcomes.
Conclusion
This study suggests that a hybrid APA program combining face-to-face sessions and telehealth is acceptable and effective in increasing PA and improving cardiorespiratory fitness among patients with NCDs. Interestingly, some of the interventional effects were maintained several months after the end of the intervention. Such a program could be an interesting alternative to face-to-face programs allowing to remove logistical barriers, while keeping some face-to-face sessions that allow coaches and patients to get to know each other and to teach the exercises to participants. Rigorous trials are needed to confirm these perspectives and compare these novel interventions to the usual care.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580251390287 – Supplemental material for Three-Year Follow-Up of a Hybrid Adapted Physical Activity Program Including Telehealth in Comparison to In-Person Care for Chronic Conditions
Supplemental material, sj-pdf-1-inq-10.1177_00469580251390287 for Three-Year Follow-Up of a Hybrid Adapted Physical Activity Program Including Telehealth in Comparison to In-Person Care for Chronic Conditions by Alexandre Mazéas, Félix Rausch, Bruno Pereira, Stéphane Penando, Melissa Roland, Aïna Chalabaev and Martine Duclos in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors wish to thank the participants of the University Hospital Clermont-Ferrand for their time and dedication.
Ethical Consideration
Written informed consent was obtained from all participants and all the used and analyzed information was obtained exclusively from anonymous data. The study was approved by local Ethics Committee (IRB00013412, “CHU de Clermont Ferrand IRB #1,” IRB 2024-CF247).
Author Contributions
Conceptualization: AM, FR, AC, and MD; Investigation: FR, SP, MR, and MD; Data curation: FR; Methodology and statistics: AM, BP, and MD; Formal analysis, AM and BP; Software: BP; Writing – original draft: AM; Writing – review & editing: all the authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work of AM was supported by a grant from the French National Association for Research and Technology (Cifre PhD Thesis) and by the company Kiplin. None of the sponsors were involved in any other aspect of the project, such as the design of the project’s protocol and analysis plan, the collection and analyses. The funders had no input on the interpretation or publication of the study results. The authors wanted also to thank the challenge 3 I-SITE Clermont Auvergne Project 20-25 for their grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.