
Abstract
Objective
To determine the perspectives to the adoption, scale-up, sustainability, and spread of technology-supported models of nutrition care, in hospital and ambulatory care settings.
Methods
Thirty-one health service providers participated in individual semi-structured interviews from a tertiary health service in Queensland, Australia. The Non-adoption, Abandonment, and challenges to the Scale up, Spread and Sustainability (NASSS) framework, designed to evaluate technology-supported models’ success, informed the qualitative design.
Results
Key findings were that technology-supported models of care could benefit many chronic condition patient groups; dietitians are well suited to adopting this technology: and the value proposition in creating efficiency gains in the health service. However, challenges of transitioning and sustainability were identified. Perceived enablers for technology supported models of care included: previous intentions for technology supported models of care prior to the 2019 novel coronavirus pandemic; opportunity for clinicians to complete higher valued tasks; and integration of technology systems and assisted staff roles. Perceived barriers included: suitability for patients is dependent on experience and ability to use technology, varied confidence by clinicians when conducting clinical assessments; high investment required for set up and ongoing maintenance; and patients desire for adopting face-to-face care over technology. Health service providers perceived that embedding and adapting such models requires maintenance of high-quality service and continued research.
Conclusions
Health service providers recognize adopting, scaling, and sustaining technology-supported models of nutrition care benefits patients, clinicians, and health services in general. Robust clinical trials and health service evaluations of technology-supported models of care, across practice settings are now needed.
Keywords
Introduction
Poor diet is one of the greatest contributors to the burden of lifestyle-related chronic conditions worldwide and in Australia. 1 Health services are struggling to meet the demands, with over 60% of the global burden of disease attributable to non-communicable chronic conditions 2 and in an Australian context more than half of the population living with at least one chronic condition. 3 Management of these conditions involves frequent visits to specialized health care for long periods of time which is resource intensive. Thus, a real challenge exists for health care services to provide high-quality care in a scalable and sustainable way.
Technology-supported models of care are disrupting traditional health and nutrition care, emerging as a feasible and sustainable way to optimize equitable access to services. It allows for the necessary repeated contact between patients and health service providers which is recommended for management of chronic conditions.4–7 Furthermore, asynchronous platforms such as mobile applications or web-based materials, allow patients targeted access to information and support at any time, supporting many approaches to self-management. 8 It also addresses geographical barriers which may exist due to a lack of mobility or transport.9,10 Recent trials have indicated that tailored nutrition advice delivered via telehealth has been found to be feasible and acceptable among patients with complex chronic conditions and their therapists within hospital and outpatient settings.11,12 The coronavirus disease of 2019 (COVID-19) health pandemic has also brought accelerated use of technology-supported models such as video conferencing and telephone, however, limited experience in mobile health (mHealth) as a model of care is considered a barrier to adoption. 13 Assessing readiness in the health service is essential for successful sustainability of various technology-supported models of care.
Understanding how to leverage technology supported model of care require stakeholder engagement with the health care system. There are many studies reporting on why technology-supported models succeed or fail, with clinician's adoption 14 and organizational challenges being some of the key determining factors. 15 Theoretical frameworks are useful tools for guiding the development and evaluation of technology supported models of care and can be useful for understanding clinicians-readiness. 16 The Non-Adoption Abandonment and challenges to the Scale up, Spread and Sustainability of health care technologies (NASSS) framework was developed to guide technology-supported health care success. 17 This framework is an ideal framework to explore readiness with areas that focus on health care staff adoption and organizational changes. The NASSS framework incorporates seven domains, namely the condition; the technology; the value proposition; the adopter system; the organization; the wider context and embedding and adaption over time (Figure 1). Although this framework is becoming more widely used in the literature to assess adoption, scale and sustainability of technology supported models of care from health service providers perspectives,18,19 it appears that it has not been tested within a nutrition and chronic condition context.

The seven domains of the Non-adoption, Abandonment, and Challenges to Scale up, Spread and Sustainability (NASSS) framework. 17
Identifying the barriers and enabling factors of technology-supported models of nutrition care will provide greater knowledge and insights for planning such interventions. Therefore, the aim of this study is to determine health service providers’ perspectives to the adoption, scale-up, and sustainability of using technology-supported models of nutrition care, in hospital and ambulatory care settings.
Methods
Study design
This was a multi-site qualitative study involving semi-structured interviews, reported according to the Standards for Reporting Qualitative Research. 20 The study used the NASSS framework to inform the interview guide and analytical approach. 17 Human ethics approval was granted by the Royal Brisbane and Women's Hospital Human Research Ethics Committee (63049) and Griffith University Human Research Ethics Committee (2020/432).
Participants and recruitment
Participants were recruited into the study across four hospitals and community services within a large health service in Queensland, Australia from September 2020 to January 2021. Participants were eligible if they were: (1) employed in the Health Service as an allied health practitioner, or executive-level management; (2) be involved with or have the potential to provide or lead teams to deliver technology-supported models of care.
A clinical working group was established to determine the recruitment strategy and refine the semi-structured interview guide. This group consisted of dietitians from each recruitment site and all members of the research team. Promotional material for the study was provided to the working group representatives for email distribution. In addition, a snowball sample was utilized from those who had already completed an interview. Once written consent was obtained, then an interview time was arranged for each participant. Interviews were offered over the telephone or via Microsoft Teams using the video and/or audio settings. To obtain varied perspectives, participants were purposively sampled to include primarily dietitians, with some representation across other allied health clinicians and executive-level management with maximal variation sampling for demographic diversity (sex, age, employment type, years of experience).
Data collection
A 9-item questionnaire was sent to participants prior to their interview to collect basic demographic information (including sex, age, area of practice, and employment type). In addition, a preparation guide was sent to participants prior to their scheduled interview. This gave participants the opportunity to reflect on the topics for discussion and ensured the interviews would run to schedule.
Semi-structured one-on-one interviews were conducted by researchers who are dietitians with qualitative research training (AB, CW, JK) and were scheduled for approximately 30 minutes. Field notes were taken during or immediately after the interviews. Decisions to refine the interview schedule were informed by two pilot interviews. Each audio recording was securely uploaded to an online transcription service developed by Microsoft Azure Cognitive Services 21 and then checked for clarity in Microsoft Word. The additional field notes helped to guide the interview discussion and if necessary, provided clarification for any inaudible parts of the recording. Interview transcripts were deidentified and then transferred to NVIVO for analysis (version 1.3.2).
Data analysis
Applied thematic analysis was used to code and theme the data with a combination of deductive (themes from the interview questions) and inductive (themes that emerged from data during analysis) approaches based on the NASSS framework. Information power guided decisions of ceasing recruitment at 31 participants rather than our target of 60. This was dependent on the assessment of the study aim, specificity of the sample, application of the NASSS framework, quality of the interview dialogue, and plans for analysis. 22 Triangulation of data occurred with researchers (AB, CW, JK) familiarizing themselves with the data through repeated readings. In addition, field notes were used to triangulate codes against transcripts. A total of 142 codes were generated and this evolved iteratively down to 57 final codes. These codes were then categorized into enablers and barriers. To ensure trustworthiness, these codes were remapped to the original transcripts to check each iteration was still reflective of the initial meaning. Themes and codes were tabulated to visually represent the relationship between and within themes of the NASSS framework. Quotes were then selected to capture key perspectives and divergent views between participants within the same sub-theme.
Results
Demographics
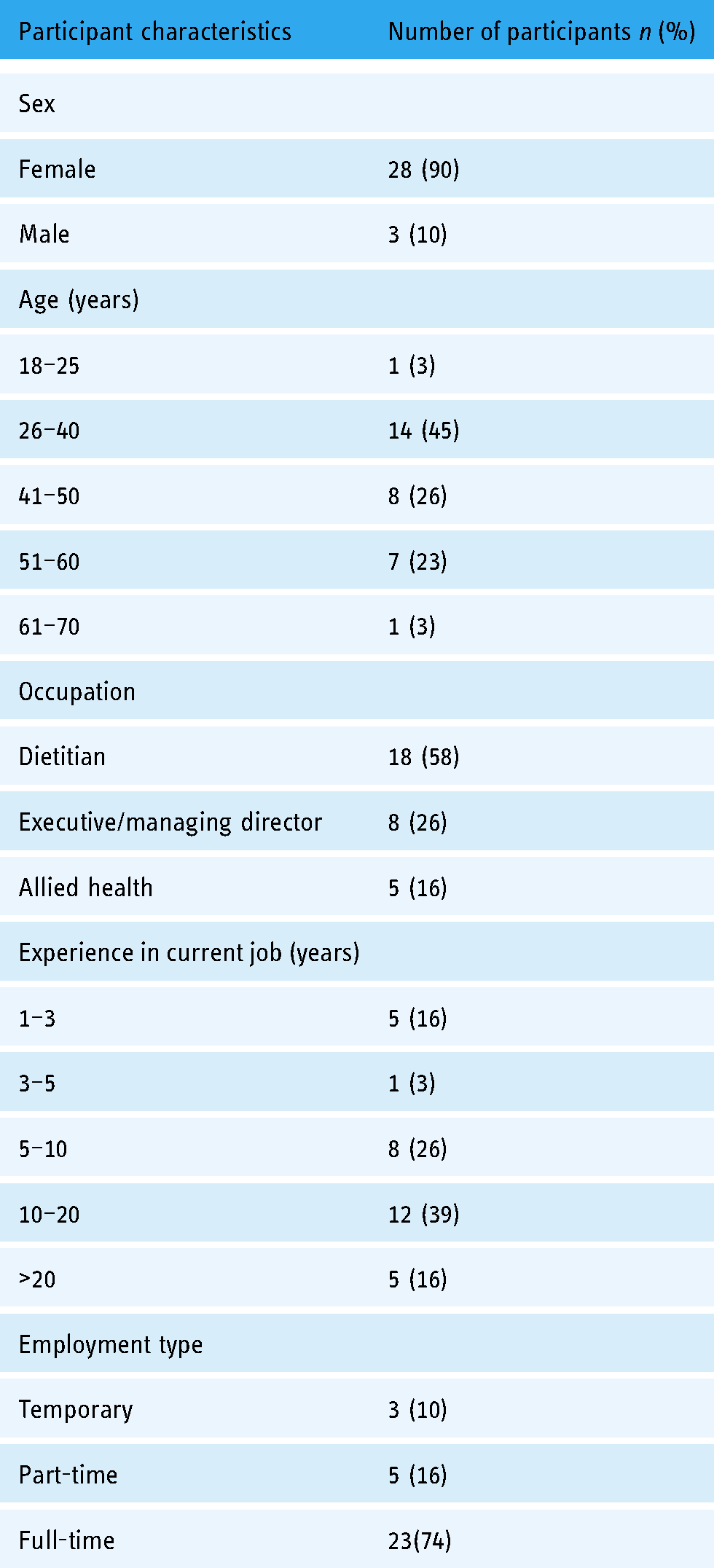
A total of 31 health service providers participated in semi structured interviews. Most participants were female (90%) and were between the ages of 26 and 40 years (45%), were dietitians (58%), followed by executive-level managers (26%), and other (non-dietetic) allied health practitioners (16%). Twenty-one interviews were conducted via video conference and 10 interviews via telephone and were approximately 29.5 min in duration. Further demographic information is provided in Table 1.
Participant demographics (N = 31).
Overview
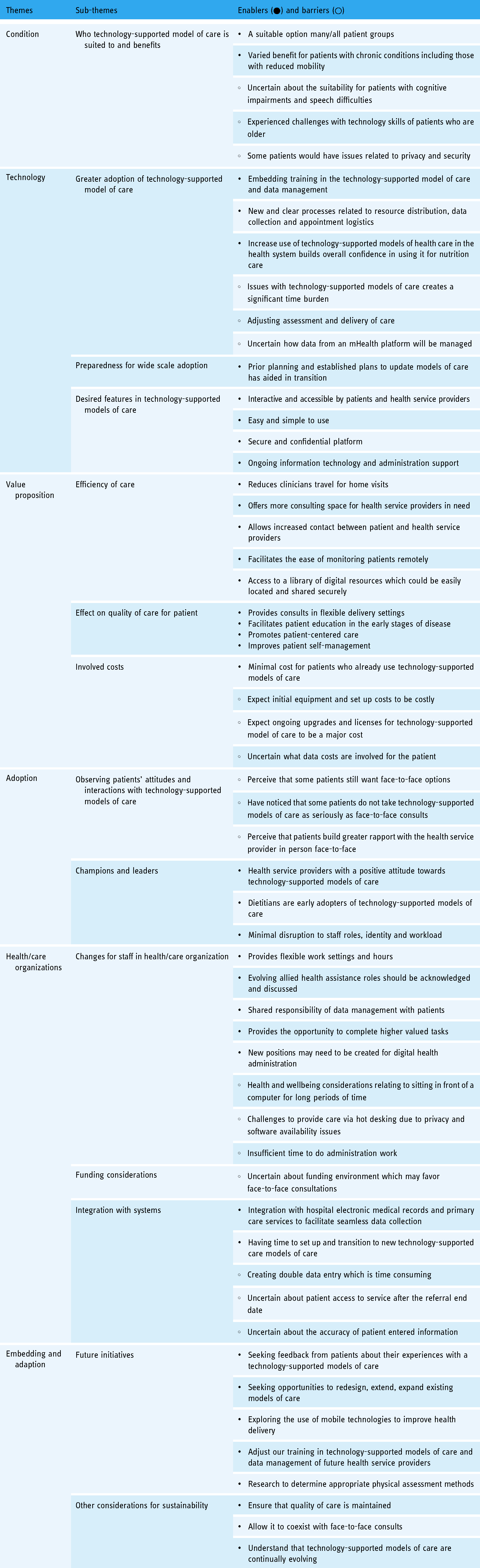
The thematic diagram for this study consists of the 14 subthemes aligned to 6 of the domains of the NASSS framework 17 (Figure 2). The arrows show the inter-relationship between the domains. Enablers and barriers (n = 38, n = 19) were identified and categorized into the various subthemes. Selection of the main enablers and barriers for each sub-theme are detailed below (Table 2).

Emergent subthemes from the interviews with health care providers and relationship between and within the subthemes identified and aligned with the six domains of the Non-adoption, Abandonment, and challenges to Scale up, Spread and Sustainability (NASSS) framework. 17 *No themes were aligned to the “wider system” domain and therefore, it is not featured in the center of the diagram.
Sub-themes aligned to NASSS framework with facilitators and barriers that emerged from interviews.
Themes aligned to NASSS framework
NASSS domain 1: Condition
Technology-supported models of nutrition care were considered suitable for many or all chronic conditions patient groups as it could allow for “ongoing regular contact” or “monitoring of progress” as re-described by some health service providers; “I think any of the chronic condition areas…I mean where there's evidence to support ongoing contact with people…you know diabetes weight management, in particular renal” (Dietitian). In addition, participants saw benefit to other outpatient groups including antenatal and pediatrics, describing them as “young and technology savvy.” They did, however, feel uncertain about using this model with certain groups of patients, including those with cognitive impairment or speech difficulties where they thought face-to-face interactions in clinic or at home would be more appropriate; “benefit in the home visit because [we could] actually see the home environment” (Occupational Therapist). They thought it would be a suitable for those who have had previous face-to-face encounters with the practitioner in which their patients had an initial assessment and some rapport had been developed.
NASSS domain 2: Technology
With increased adoption of technology-supported models of care, some dietitians said they had to adjust the way they provided care over the phone or video conferencing including anthropometric assessments; “adapt to not having scales and trying to get other things … like clothes feeling looser, all those other things to try and make your assessment…” (Dietitian). They recognized that many new processes occur with increased adoption of technology and that these processes should be clear for all of those involved. Moreover, participants who recently started using video conferencing in their health facility, acknowledged the importance, yet challenges of training staff in this model of care “…it was up-skilling our clinicians and that was a big issue in itself…we do have an older workforce in our service, getting the confidence and competence of our staff to use the different platforms we were using” (Exercise Physiologist).
The COVID-19 health pandemic resulted in escalated use of technology support models of care. Some health service providers discussed that their organization or departments had established plans to update models of care prior to the pandemic; “it had been something that had been discussed for probably a couple of years that we needed to move that way” (Physiotherapist). Participants who reported these types of pre-established plans, found it to be a more agile transition to virtual care compared to others.
Most dietitians indicated the ease of use as an important consideration in the design of a technology support model of nutrition care, describing a simple link that the patient could easily have “clicked on” to access the service would be desired. Furthermore, many thought ongoing troubleshooting support for technology-supported models of care for both health practitioners as well as patients would need to be considered in the design of a new mobile health (mHealth) platform; “…having some sort of troubleshoot or a support network where people would be able to phone…like a helpline” (Dietitian). In addition, ensuring there is adequate administration support to facilitate the appointment bookings process was raised as an important feature of this model of care; “…sending out the appropriate link, making sure that it's, I guess privacy protected as well…” (Dietitian). Many participants who reported these desired features found it to be the components that were missing in their current technology set up at their health site.
NASSS domain 3: Value proposition
Some health service providers generally perceived that technology-supported models of care, particularly mHealth applications could be used in the future to monitor patients remotely with greater efficiency; “blood sugar levels or food diaries [records could capture] real information as opposed to in a clinic when you’re asking people to recall” (Dietitian). This was particularly relevant to dietitians who indicated the importance of such measures for their nutritional assessments. In addition, some health service providers indicated that technology-supported models could “free up” consulting room space for practitioners who require face-to-face interactions with their patients; “…our hospital, is bursting at the seams, so we’ve been able to free up outpatient rooms for other areas that have needed that need like physio for example” (Executive/ managing Director). They acknowledged that this could be a potential cost-saving to the health service with less of a reliance on certain infrastructure and or resources.
Many health service providers identified that technology-supported models of care provides consults in flexible delivery settings, with access to resources and care on demand; “…they’ve got access to the education resources all the time…” (Physiotherapist). They described it as opportunity for patients to take “ownership” of their organized care and self-management. With increased self-management, some health service providers thought it could positively impact the acute care environment; “hopefully reduction of say ED [Emergency Department] presentations or reduction of exacerbations of their conditions.” They perceive this to reduce demands on the health service. Participants also thought that offering technology-supported models of care could overcome some of the barriers for patients to attend their appointments and in turn, reduce non-attendance rates at health services.
Health service providers identified that not only would there need to be investment in the initial set up of technological equipment and infrastructure, but there would also be ongoing costs for training, licenses, and maintenance of the equipment. The ongoing costs were thought to be a major expense and cost consideration for managing directors; “it's actually the maintenance…that cost us more than the initial infrastructure” (Executive/ managing Director). These costs were viewed as an important investment and not necessarily a barrier. In addition, most of the health service providers identified that access to the devices and data would be costs considerations for the patient. Understanding the involved costs for the patient was particularly important for dietitians and other allied health, reassuring their patients that it is an affordable service. They did acknowledge that costs for both health service and the patient would depend on the design of the model; “costs are variable and dependent on what model would looks like” (Dietitian).
NASSS domain 4: Adopters
Health service providers perceived that some patients have a preference to receive face-to-face consultations over video conferencing. They perceived that patient want face-to-face consultations for several different reasons including “not [feeling] comfortable” to use technology, or they “don't have access to technology.” Additionally, they also thought patients don't establish rapport with the health service provider over video conferencing or phone appointments as well as face-to-face consultations; “…over the phone, they [patients] are not sort of building rapport…” (Dietitian). Some health service providers also noticed that patients do not always take technology-supported models as seriously as face-to-face consultations, particularly phone consultations; “they are not committing to those appointment times, not treating them as the same” (Dietitian). As a result of these observations, dietitians and other allied health were hesitant to use technology-supported models of care at times.
Some health service providers particularly executive/ managing directors and other allied health professionals, described dietitians as “notoriously early adopters” and “change advocates” for technology-supported models of care. They perceived that the dietetic profession lends itself particularly well to using virtual care modalities; “the nature of [dietetic] interventions as opposed to say, occupational therapy….[where] you really need to be in at home environment” (Occupational Therapist) and “We are pretty fortunate, dietetics within [our health service] are actually one the strongest allied health professions in terms of virtual care and have been since COVID struck” (Executive/ Managing Director). However, all participant groups perceived that adoption of this model of care is greatly dependent on the attitude of whole team of health service providers; “it comes down to everyone in the team… the leadership…the involvement, the ‘willing[ness] to take on new challenges’” (Executive/ Managing Director).
NASSS domain 5: Health/care organization
Many executive managing/ directors perceived that with increased adoption and scale-up of technology-supported models of care there would likely be new and evolving staff roles. Some thought allied health assistants could be used “more effectively” where they are delegated tasks to review mHealth data for the allied health practitioner “[They could] look through data and identify red flags” (Executive Managing Director). Others thought that there would be creation of new virtual job roles, with the responsibility of setting up equipment, ensuring the technology was working and managing the data. As a result of these new or evolving staff roles, some participants thought allied health practitioners would be able to focus on completing higher valued tasks; “almost potential to enable professionals to have an increased focus on their full scope” (Executive/ Managing Director). Furthermore, health service providers perceived that a challenging aspect to providing technology-supported care is the “shared spaces” in hospitals which could result in privacy or software availability issues; “it comes down [to] finding the room that has got the right technology” (Executive/ Managing Director). Health service providers felt that the organization of technology-supported models of care would be a particular consideration for executive/ managing directors.
Several health service providers acknowledged that there are differences in funding for various service models and it currently favors face-to face consultations; “a significant difference in the amount of funding and WAU [Waited Activity Units] attracted for a telehealth assessment versus a phone assessment” (Dietitian). They indicated uncertainty with how much funding would be allocated to models such as mHealth; “if we are interacting with people, you know through an app, how is that funded?” (Dietitian). They did acknowledge that funding determines the time allocated to occasions of service and influences a practitioner's workload and schedule.
All groups perceived that in order to support the use of technology-supported models, all hospitals within a metropolitan area would need to be upgraded to electronic medical record (EMR) keeping. They would like that technology-supported care systems integrated with hospital EMRs to “streamline” the data collection processes, by saving allied health service providers valuable time with recording data; “integrate into electronic medical record…to prevent duplication” (Dietitian). They also saw it as an opportunity to work more efficiently with General Practice (GP) clinics; “…we are not integrated well with GPs, there's a lot of faxing backwards and forwards of results and emailing” (Dietitian).
NASSS domain 7: Embedding and adapting over time
As indicated in theme 4, participants revealed some of the “desired features” of a technology-supported model of care. However, this theme also highlighted that Health service providers realize the importance of engaging with consumers to understand their perspectives on the future design and implementation of technology-supported models of care; “I think you know engaging the consumers around elements they would like…” (Dietitian). In theme 8, Health service providers shared “observations of patients’ attitudes and interactions with technology,” however, within this theme, the importance of further exploring the usability of mHealth technologies; “[Finding out] why do people stop using apps or why people never get to using an app” (Psychologist). In addition, in theme 2, some dietitian participants reported adjustments to their anthropometric assessments as result of increased adoption of technology. They highlighted that they felt this was challenging at times and further research to determine appropriate physical assessment methods for practitioners was indicated; “…even physical assessments like subjective global assessments (SGA's), patient-generated subjective global assessments (PGSGA), that's quite difficult and whether or not there needs to be some kind of development in that space” (Dietitian).
Health service providers indicated that in order for technology-supported models of care to be sustained long-term, quality of care needs to be maintained by the allied health practitioner; “no reduction in service and quality… [that you] will be giving the client” (Executive/ Managing Director). In addition, health service providers felt that technology-supported models of care should be “complementing” or “supplementing” traditional care but to not act on its own, for a “hybrid” model to exist. This concept strongly links back to theme 6 “Effect on quality of care for the patient,” which emphasized the importance of flexible delivery of health service options for patients.
Discussion
Principal findings
This study explored health service providers’ perspectives to the adoption, scale-up, and sustainability of using technology-supported models of nutrition care, in hospital and ambulatory settings, guided by the NASSS framework. 17 Our findings revealed that health service providers perceived value of technology-supported models of nutrition care providing effective and high-quality care to many patient groups. Dietitians were the most prepared and efficient in providing this care and were seen by the health services as well suited to adopt virtual models. However, there were notable challenges that still exist for transitioning and overcoming current organizational barriers.
Clinicians perceived that patients with chronic conditions are well suited to technology-supported models of nutrition care due to the ongoing support required in this group. A key value proposition identified was the ability to monitor patients remotely, reducing patients’ barriers to attend their appointments and thus potentially improving non-attendance rates. In various chronic disease groups, technology-support models of care have demonstrated improvements in diet and other health-related outcomes. 23 Moreover, our participants thought it would be particularly suitable for those who have had previous face-to-face encounters with a previous initial nutrition assessment and established rapport. This supports similar findings of a health service provider who chose to use a mHealth application with their patients because they were familiar with their medical condition and their needs. 24 In addition to our study, suitability was thought to be dependent on the individual's past experiences and abilities. Older adults, who often experience cognitive issues, have indicated that using tablets and similar devices can be challenging. 25 Along with usability, other technology adoption challenges for older adults have been related to affordability, accessibility, and confidence. 26 This complements our findings that health service providers perceived that patients still want the option of face-to-face appointments because of accessibility issues or not feeling comfortable to use technology-supported models. Thus, technology-supported models of care were envisioned to be complementary to usual care, not fully replace it, hence the importance of maintaining face-to-face consultations to allow for individualized care. Furthermore, as identified by participants, capturing the perspectives of consumers themselves as a result of greater exposure to technology-supported models of care in more recent times, is needed.
Like health services around the world, the COVID-19 health pandemic has been a catalyst to providing alternatives to in person care. 27 The rapid update to integrate technology into healthcare delivery resulted in an agile transition to technology-supported models of care, however, dietitians reported feeling a lack of confidence about certain aspects of nutrition care including conducting anthropometric assessments virtually. This lack of confidence can also extend to subjective measures of health which are also prudent to quality nutrition assessments. For example, a qualitative study found that health care providers were concerned about the difficulty with capturing emotions when using mHealth technology. 13 Our participants acknowledged the importance of training in technology-supported models of care and that adjustments to training processes may be required to become more competent and literate with digital health technologies, and to ultimately improve digital health adoption, scale up, and sustainability. Training could assist dietitians to become more familiar with the emerging research that is guiding clinicians with virtual assessments, including anthropometry. 28 With many clinicians struggling to transition and having limited experience to such models of care, 13 training is considered imperative to the success of technology implementation. 29 This highlights the need for adequate support and resources to coordinate training including university training for future dietitians to have the foundation knowledge to deliver these methods.
Embedding new and clear processes related to resource distribution, data collection and appointment logistics was recognized as a critical facilitator of effective care delivery via technology-supported models. However, participants indicated they were concerned that administrative tasks would continue to be a significant time barrier with increased adoption and scale up. This supports existing research that administrative tasks involved with technology-supported models of care is a common barrier to adoption among clinicians.30,31 In our study, ongoing administrative support, the creation digital health administration jobs, and utilizing health assistants, were all considered potential solutions to overcoming these organizational concerns. Such changes were thought to provide dietitians the opportunity to complete higher valued tasks. Dietitians have previously indicated insufficient time within consultations to effectively use communication skills, and behavior change techniques. 32 Moreover, patients have indicated that effective communication with the dietitian is appreciated and supports a positive experience. 33 Therefore, there would be great value in the creation of new digital support roles for improving efficiencies within the health organization and to ensure quality of care for the patient is upheld. There is also some recent commentary that this might be a natural evolution of the dietetic profession, as nutrition care continues to be disrupted by digital technologies. 34
Health service providers acknowledged that the current funding environment has favored face-to-face consultations. They were uncertain of the funding allocated to occasions of service that involved mHealth as a result of limited exposure to this model of care. The intention to secure funding for digital health technologies is evident in strategic documents. 35 However, at the present time there appears to be no specified funding model for technology-supported models of care within hospital and ambulatory care settings. There is evidence in a dietetic position statement that mHealth is a growing area and is effective at improving and monitoring dietary behavior. 23 This position statement has indicated that technology supported models could be funded more broadly when it is complemented by existing care services and/or emerging technology supported models of care like mHealth.
The current study found that integration of technology-supported models of care, particularly mHealth, with EMRs and primary care services was thought to support data collection processes. Other studies have maintained that technology models of care lack integration with EMR and this increases clinician's workload which is one of greatest barriers to digital health buy-in from clinicians.24,31 Our analysis complements findings that physicians have a high interest to use mHealth integrated with EMR without previous experience using the systems. 36 However, like other components of technology supported models care this was perceived to be a high investment for the set up and maintenance.
These study findings have indicated that adoption, scale up, and sustainability of technology-supported models of care is currently impacted by patient engagement, adequate training and support, secure funding, and systems to improve interoperability with other health system technologies. Thus, we hypothesize that there is a lack of incentive for health service providers to adopt technology-supported models of care at present. In order to adequately embed and adapt technology-supported models of care, more evaluations of digital interventions within hospital and ambulatory setting are needed.
Limitations
It is important to highlight the limitations of this study. We purposively sampled to primarily include dietitians, with some representation across other allied health clinicians and executive-level management of allied health practitioners. Doctors and nurses were not recruited into this study but we appreciate that they have a very important role in the delivery of nutrition care as indicated in the literature. 37 Nonetheless, the shift to virtual nutrition care due to COVID-19 was an opportunity to examine nutrition service delivery more specifically from health professionals who are delivering nutrition care or allied health professionals who face similar enablers and barriers to using virtual care in a tertiary setting. Another limitation of the study is that results reflect the experience within a large Australian public health service and therefore, may not reflect other countries and in the private sector. Further to this, the number of participants and male representation within each occupation was limited. Reports on the Australian dietetic workforce indicate that a high percentage of females represent the dietetic profession (88–96%), with the majority aged 35 years or under (54–55%).38–40 Our study sample of dietitians is a close representation of the dietetic workforce in Australia, with a slightly higher percentage of females (100%) and two thirds aged 40 years or under (67%). Participants were involved on voluntary basis, thus the health service providers involved were willing to discuss their perspectives and experiences with using technology-supported models of care and it is unclear what bias this may introduce to the findings.
Conclusion
This study investigated the perspectives of health service providers readiness to embrace technology-supported models of care. The main perceived barriers include suitability dependent on patients’ past experiences and abilities, health service providers lack of confidence with some aspects of conducting the assessment, additional administrative tasks for health service providers, and no funding mechanism to adequately support technology-supported models of care. Enabling factors to support adoption, scale up, and sustainability is allowing it to co-exist with face-to-face care, adjusting training, creating new or evolve support roles and greater exposure to mHealth and robust clinical trials within a range of practice settings. These findings provide greater knowledge and insights to inform future pragmatic trials and health service evaluations of technology-supported models of care for embedding and sustaining clinical nutrition practice.
Footnotes
Acknowledgements
This study was funded by the Griffith University New Researcher Grant Scheme. The authors would like to acknowledge and thank all the health service providers from the various Metro North and Hospital Health services that volunteered to participate; The Prince Charles Hospital; Royal Brisbane and Women's Hospital; Caboolture Hospital; Redcliffe Hospital; Community and Oral Health Services. Many thanks to the clinical working group representatives for their contribution to the study.
Contributorship
AB led the write up of the article. AB, CW, and JK contributed to study design, interviews, analysis, interpretation of the results, and approved the final article. KC contributed to the study design, interpretation of the results, and approved the final article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Royal Brisbane and Women's Hospital Human Research Ethics Committee (63049) and Griffith University Human Research Ethics Committee (2020/432) approved this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Griffith University New Research Grant Scheme (grant number 52716).
Guarantor
AB.