
Abstract
This study assesses the implementation and time savings associated with an innovative business-to-customer model (B2C) for the remote application of sound processor upgrades, a task related to ongoing cochlear implant maintenance. The upgrade to recipient model (U2R) involves the transfer of patient data to a cloud where the company that supplies the upgraded processor can upload it into the devices and dispatch them directly to the patient. It replaces the traditional face to face model, requiring patients to come into the clinic. Four clinics in the U.K. and one in the Netherlands were surveyed on their experiences and satisfaction levels after implementing this model. The time saved when using the U2R model was compared to the time taken for a face-to-face appointment. Upgrades were done using the U2R model in 43% of adults and children. Time savings ranged between 21 and 65 minutes per patient. Although patients were reported to be satisfied with the service, up to 50% of U2R patients requested a further in clinic follow up appointment. Four out of five clinics were satisfied with the current U2R model and would recommend it to another clinic. The other clinic required modifications to the administration of the model. Large savings in clinic and patients costs and time were reported. Streamlining the process within clinics and providing better remote support for patient reassurance and to solve equipment issues at home would ensure that time savings are maximised and the B2C model provides comparable quality to an in-clinic appointment.
What do we already know about this topic?
Cochlear implants (CI) are a treatment option for those with severe to profound hearing loss and are provided in specialist centres. CI recipients require ongoing support for their lifetime and CI centres have an ever-increasing workload with limited resources.
This study assessed the implementation and time savings associated with an innovative business-to-customer (B2C) model to support equipment upgrades for existing CI users. The upgrade is facilitated by the manufacturing company and the device sent directly to the patient.
The study confirms that the B2C model is viable in this setting. Clinical workload and patient travel time were reduced, creating value for both patients and the service providers.
Introduction
The modern approach to medicine is to streamline services to make the best use of time and resources to benefit both the patient and clinician. The use of digital tools, telemonitoring and online appointments has made some progress towards achieving this, with many innovations accelerated by the COVID pandemic.1,2 There are ever increasing pressures on health care from our ageing population and new and innovative ways of providing healthcare are needed.3,4 Technology based “eHealth” services are one way of improving productivity and a new Global strategy on digital health 2020 to 2025 has been developed to implement a long-term strategic plan. 5
The provision of remote services for patients allows health conditions to be monitored or assessed at a distance. It enhances the clinician’s ability to manage their patients and helps patients to engage with a healthcare system on their own terms.6,7 It can be implemented using a variety of different business models. 8 A business-to-customer model (B2C) differs from remote healthcare where the service is still provided by the clinician, by delegating services to an external third party provider. An example of this is the proposal of telemonitoring of chronic heart conditions where there is cooperation between the healthcare organisation and the device manufacturer. 9 A recent assessment of this type of service provision concluded that “customers benefit from the service when they need it, healthcare benefits from the reduced burden and improved effectiveness, industry benefits from the creation of innovative businesses, and governments benefit from reduced expenditure while citizens enjoy the best possible care.” 10
For remote services to be introduced successfully, staff concerns that the remote model may mean less time spent caring and more in administrating need to be addressed. 6 Having some staff with previous experience with remote health care provision can help to champion the new service. 6 It is also important that all staff are prepared for the transition and are able to ask questions before the policy is implemented, while making sure that the reasons for using the new model are well understood and the risks and benefits clearly identified. 6 Despite their advantages for increased productivity in the health service, there is currently limited research into the effects and implementation of remote services on staff, service provision and productivity, irrespective of the intervention. 6
The high prevalence of hearing loss in the global population places increased pressure on hearing services with 5% of the global population having a disabling hearing loss and nearly 30 million of these with profound or complete hearing loss in both ears. 4 This places increased pressure on hearing care services and tele-audiology has been widely used in all aspects of hearing to ameliorate this.11,12 A Cochlear Implant (CI) is a treatment option for those with a severe to profound hearing loss. The treatment is provided in specialist centres and recipients require ongoing support for their lifetime, or for as long as they continue to use the device. There are a limited number of CI centres in each country due to their specialist nature with an ever-increasing workload and limited resources. For example, there are a total of only 18 adult CI centres covering the United Kingdom and seven in the Netherlands, therefore patients often travel long distances to their CI clinics. The COVID-19 pandemic accelerated the provision of remote support for CI services and a large multisite telemedicine study evaluating a remote care pathway for all aspects of CI fitting is currently underway in the UK.13 -15
Improvements in sound processing and microphone technology, connectivity, and aesthetics can be made accessible to existing CI users via upgrades to their externally worn sound processors.16 -19 The upgrade process occurs every five to six years and usually involves the patient having to travel to the clinic for what is often a straightforward transfer of details and the programme from one sound processor into another. The clinic then provides instructions on usage, connectivity and any differences from the previous processor. This represents the standard model of face-to-face (F2F) service delivery (Figure 1). This study assessed the implementation and time savings associated with an innovative business-to-customer model where the sound processor upgrade is facilitated by the manufacturing company and the device sent directly to the patient. In this service delivery model, the clinic orders the desired sound processor and provides the company with the correct programming information. The company then sends the pre-programmed processor direct to the patient along with a user video. This allows the company to manage the administrative tasks, with the clinic still directing and responsible for the clinical aspects of the upgrade, potentially saving clinic time. The patient benefits by not having to travel to the clinic and has more ownership of their own health care.

Schematic of the standard model of service delivery face to face (F2F) and the tasks done at each stage.
The aim of the study was to assess the impact of the implementation of this remote B2C service on staff, service provision and productivity from five clinics and compare it to the existing face-to-face model. A useful tool for describing the success of this type of technology innovation is proposed by Herzlinger (2006). 7 They propose six areas to be considered: (1) the structure and players involved, (2) financing and cost savings, (3) implications for public policy, (4) effective technology, (5) consumers, and (6) accountability. This approach was used by Grustam et al. (2017) 10 to measure the success of a fictitious business-to-consumer model for telemonitoring patients with chronic heart failure. The results of this study will be viewed using this model structure. To the best of our knowledge this is the first report of the suggested B2C framework being applied to a real scenario in a hospital setting where audiological services are free of charge at the point of use.
Method
Clinics were selected who had embedded U2R as part of their clinical routine and not clinics who used it for specific patients or for short time periods and where the data transfer issues could be resolved. Four clinics from the UK and one from the Netherlands agreed to participate in the initial phase and the survey.
The U2R process is outlined in Figure 2. The clinic is required to contact the patient (or patient’s guardian) to invite them for upgrade and establish what sound processor type, magnet strength and colour they would like, and the order placed. The magnet holds the processor coil on the head. If it is too weak the coil may fall off easily, if too strong it can cause skin breakdown. The clinic orders the desired sound processor and accessories from the company and converts the patient’s programme in the proprietary company software (Nucleus® Custom Sound Pro [CS Pro], Cochlear Ltd., Sydney). The sound processor programme for that patient is then automatically uploaded to the implant company’s data cloud (certified to ISO/IEC 27001) where it can be accessed by the company and provides the company with the correct patient programmes to be loaded into the processor. The company then sends the pre-programmed processor direct to the patient at home along with a user video.

Schematic of new method of service delivery upgrade-to-recipient (U2R) and the tasks done at each stage.
To use the U2R model, patients were required to be either signed up to an existing company initiative giving permission for the company access to their personal data or to sign the clinics own declaration forms giving the correct permissions required for data protection.
An unvalidated questionnaire was sent out to the five clinics to gather insights from clinicians regarding their general experiences with both F2F and U2R business models and the clinician’s view of the patient experience.
Questionnaires were completed between the 26/2/2024 and 22/4/2024. A detailed copy is attached in Supplemental Appendix A.
Data was collected from the clinicians and stored using a standard electronic survey tool and stored on a Health Insurance Portability and Accountability Act of 1996 compliant server (Qualtrics LLC, https://www.qualtrics.com). To allow responses to be tracked, each survey was linked to an individual clinic but no personal information from the respondent was collected. The data collected pertained solely to general clinic insights and experiences and did not include any identifiable patient information.
The study followed the relevant EQUATOR guideline, Standards for QUality Improvement Reporting Excellence. 20
Ethics Statement
No ethics approval was required for this study based on the tool provided by UK Health Research Authority and guidelines from the Dutch Central Committee on Research Involving Human Subjects. The study was conducted in accordance with the local ethical requirements of the participating centres. The survey and report were initiated by Cochlear, the manufacturer of the Nucleus Cochlear implant. The clinics and clinicians that participated in the study provided consent for publication.
Statistics
This is an exploratory study using descriptive methods and thus descriptive statistics have been used. No hypotheses were specified and thus sample sizes were not determined, and statistical methods not applied.
Results
One set of responses was provided per site representing the views of the whole clinic. The questions asked for each section are provided for ease of reference.
Clinic Information (Q1-Q7 and Q9-Q15)
Question 1. How many Cochlear™ implant users are currently followed at your clinic?
Question 3. How many new Cochlear™ implant users have been implanted in your clinic in the last calendar year?
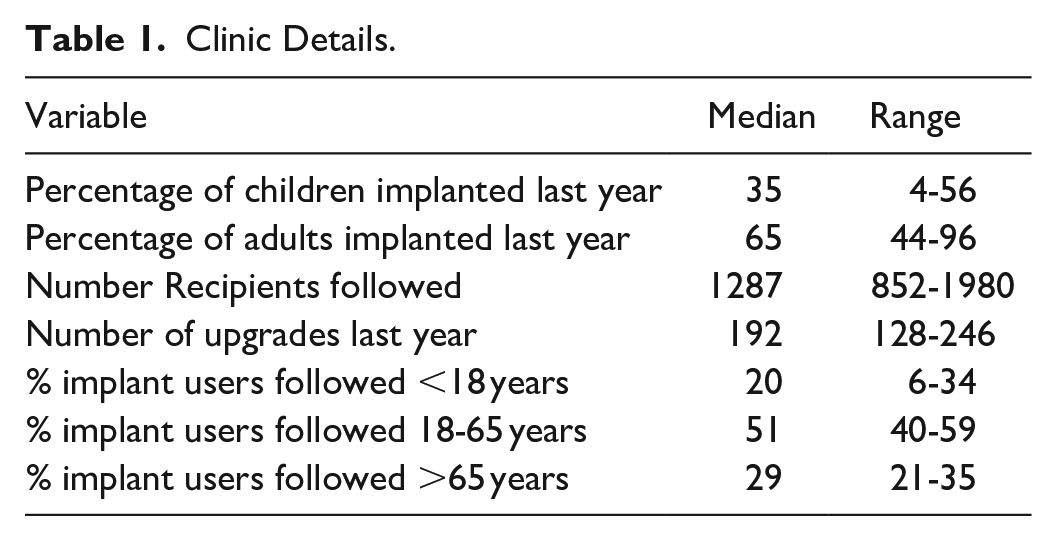
Clinics followed between 852 and 1980 implant users each, and most were adults (Table 1). New implantations per year were also predominantly adults, with only 1 clinic implanting mainly children (Table 1). A median of 15% of the total users followed received an upgrade in the previous year.
Clinic Details.
Question 2. What is the maximum distance a patient would need to travel to attend clinic?
An exact figure could not be given, but all participating clinics reported having patients nationwide who travelled to the clinic from distances of up to several hundreds of miles.
Question 9. For how long has your clinic been using the U2R model?
Question 10. What prompted your clinic to start using U2R initially?
Four out of five clinics were prompted to try the U2R model due to the COVID-19 pandemic, and for the fifth, there was pressure on clinic space and capacity. All had used the U2R model for at least two years with a maximum of three years.
Question 4. How many Cochlear™ implant users have had a Sound Processor upgrade in the last calendar year?
Question 7. For those CI users that got a Sound Processor upgrade in the last calendar year, how many received their upgrade in the clinic face-to-face?
Question 15. In the last calendar year, how many CI users that got a Sound Processor upgrade did it via U2R?
Over the year prior to this survey, the five clinics included had done 969 upgrades in total. 553 (57%) of these were face to face (F2F) and 416 (43%) were done using the upgrade to recipient (U2R) model (Figure 3). The predominant age of patients using the U2R model in all clinics was the 18 to 64 years old group, reflecting the main age group of most CI recipients (Figure 4). Clinic 4 sees very few children, and this is reflected in the low percentage of children using U2R. Clinic 2 has not used U2R for children to date and does not routinely offer U2R to patients over 70 years of age, based on earlier experience with this age group.

Percentage of total upgrades done with U2R by clinic.

Age distribution of patients using the U2R model by clinic.
Question 5. How often do CI users receive a Sound Processor upgrade?
Question 6. Are there any specific requirements a CI user needs to fulfil to receive a Sound Processor upgrade besides the time passed since their last upgrade?
Upgrades were offered to recipients every five to six years but could be delayed or withheld if the recipient had previously lost or damaged a device beyond repair or was a partial or non-user and for patients with dementia who may be confused by the change in device.
Question 11. What were the initial clinical staff opinions on U2R?
Question 12. Did these opinions change with time/experience?
Question 13. Did you develop any staff training and/or protocols/pathways?
Question 14. Were there staff specifically dedicated to implement U2R? (eg, For training, administration, etc.)
Staff were initially sceptical with concerns that time and resources would not be saved, and that data breaches and errors would occur. With experience, most staff became more confident in the U2R model. Protocols and pathways evolved over time. Information gathered about the feelings and views about the U2R model from the staff specifically dedicated to implementing the U2R model were given in an open format and are included in Supplemental Appendix B.
Staff specifically allocated to U2R varied across clinics within the UK and between the two countries:
The Patient Experience (Q16-Q18 and Q25)
Question 16. What factors do you consider at your clinic when identifying/selecting CI users for U2R?
The factors considered by clinicians when selecting patients for U2R included: Age, education level, geographic location, patient preference, access and ability to work with a computer.
Exclusions reported for not offering U2R to a patient were:
No follow up in the previous six years or a long time passed since their last appointment.
Historic issues with upgrades or battery-life issues.
Additional needs.
Patients with limited English or Dutch (depending on location).
Older generation CI device user (eg, Nucleus CI22).
Complex needs or complex programming sound processor parameters.
Patient is recorded as a non-user or potential non-user.
Sign-language or interpreting services needed and all parties prefer face to face interactions.
Those requiring F2F due to combined hearing-aid and CI pairing.
Question 17. In your opinion, what would be the optimal way to identify and contact patients for U2R?
Patients were contacted either by letter or email to offer them an upgrade. For some clinics, all patients meeting the clinics U2R inclusion criteria were informed that this is how they would receive their upgrade. Other clinics allowed patients to choose whether to have U2R or F2F. One comment was that those patients who chose to not email about spares were not interested in U2R. One clinic offered users a check-up visit after receiving the U2R processor as standard.
Question 18. From the patients you select for U2R, what is the uptake proportion?
The percentage uptake rate across the clinics varied from 80% to 100%. Clinic 2 and Clinic 3 reported 100% accepted. Clinic 3 reported that 25% of the children who received U2Rs attended the clinic afterwards without having a scheduled appointment. Clinic 4 reported 11% declined U2R, 5% of these gave a reason including: Convenience (works at the hospital), experiencing pain around implant site so wanted a visual check, ear infection present so wanted advice and guidance, having trouble with existing programmes so wanted this explored as part of the upgrade process, patient lost previous processor so needed to attend department for further action, patient was having problem with other Cochlear services (ie, Remote Check self-evaluation smartphone application), patient declined because they did not have access to email. Clinic 5 reported all eligible paediatric patients had remote upgrades and 80% of their adult upgrades were U2R after removing the bimodal patients.
Question 25. What information do you share with patients when you introduce them to U2R?
The upgrade letter introduced the concept, explained potential benefit to the patient and signposted them to the Cochlear website for further information. For example, one clinic letter explained that a “pre-programmed sound processor (based on the settings of your current processor) will be sent out and you can start using it immediately.” The unboxing video was shared. One clinic also offered a video links sheet with YouTube videos, the UPS shipping service smartphone application, what is included in the kit, and specifics about making sure they have been sent the right magnet strength and the consequences of that been wrong. Alternatives were also offered for F2F if the patient was not happy.
Question 26. What were the initial patient opinions on U2R?
Patient opinions were not gathered directly as part of this study. However, clinics reported that users were mostly positive, perhaps some were more receptive during COVID-19 pandemic and were now pushing back and requesting F2F. One clinic reported that 90% of U2R recipients were satisfied with their U2R upgrade. However, one comment states that: “Patients are not confident to accept care via remote means. Patients are nervous to lose the interactions they are used to with the clinic. Patients are worried that things will sound different with their upgrade but with no option for remap when U2R. Some anxieties about the safe delivery of their processor.”
Clinic Costs and Time Savings (Q8 and Q19-Q21)
Question 8. Considering the Face-to-Face upgrade appointments in your clinic, please indicate in the table below the average duration, staff involved/banding and facilities used for each of the identified activities, from a clinical perspective.
Question 19. Considering Upgrade to Recipient model in your clinic, please indicate in the table below the average duration, staff involved, and facilities used for each of the identified activities, from a clinical perspective.
The time taken per task for the U2R and F2F models were compared and the time savings calculated (Table 2). No change was reported for the grades of staff allocated to each task. Room allocation was freed up as no device counselling or programming session was required (soundproof booth, clinic room and consultation room) and there were four reports of tasks now done by clinic staff during home-working (programme conversion in software, device counselling and update notes). Staff allocated to the tasks where most time was saved were audiologists, clinical scientists, and speech therapists, although these staff were still used to convert the programme for the upgraded processor in the U2R model.
Average Time Saving in Minutes for the U2R Models Compared to the F2F Model in Minutes by Task and by Clinic.

Note. Negative numbers indicate increased time for the task when using U2R.
Device counselling and convert map included in same 60 minutes clinic appointment. In consultation with the clinic, a gain of 15 minutes was calculated.
Other tasks are supporting patients remotely who have difficulties with their new kit and checking name and address details.
Additional tasks for the U2R that weren’t needed in the F2F model were reported by clinic 2, (Supporting some patients remotely who have difficulties with their new kit, 5-60 minutes) and clinic 3 (check name and address details and send order confirmation, 8-18 minutes).
Question 20. Do you usually perform any of the activities described on the table above for more than one patient at a time?
Clinics 1 and 5 upgraded groups of patients using U2R once per month.
Question 21. Did any of the CI users that used U2R have a face-to-face appointment related to the upgrade soon after and what were the top five triggers for requesting and in person appointment?
Some patients did request a clinic visit following the U2R upgrade and the percentage varied widely (Figure 5). One clinic reported that an additional 10% to 20% needed either some phone contact or had some questions over email.

Percentage of patients requesting clinic visit following a U2R upgrade.
The top five triggers for returning to clinic were different for each clinic (Table 3). Clinic 5 did not reply to this question. Remote consultation could have resolved some of the connectivity issues as well as the Remote Check smartphone-based check-up facility to reassure recipients. The option for remote mapping would also help.
Top five Triggers for Returning to the Clinic for a Face-to-face Appointment.

Patients Costs and Time Savings (Q23-Q24 and Q26-Q27)
Question 23. What are common challenges the patients face when attending in-clinic visits?
Common challenges for patients during F2F upgrades were associated with coming into the clinic:
Need to take time off work
Travel long distances
Cost of travelling for example, parking, fuel, or train tickets
Older patients need someone to bring them but also often can’t manage a U2R
Childcare
Challenges of travelling into central London for elderly or disabled patients
Takes more time before they will be invited in clinic due to capacity limitations
Traffic hold ups around the hospital site
Train strikes (we encourage patients to use the hospital train station)
Inflexibility of appointment times/day (no weekend/evening clinics)
Hospital transport is difficult to access and inflexible with timings. Patients often face long waiting times
Hospital waiting area is not comfortable for those with disabilities or additional needs
Question 24. Considering the Face-to-Face upgrade appointments in your clinic, please indicate in the table below the average duration and costs associated to each activity from the patients’ perspective.
Patient costs for F2F upgrades and U2R could not be reliably estimated as the distance to the clinic varies greatly by patient, but included parking at the hospital, time off work, and travel to hospital. Travel time for F2F appointments could also not be estimated accurately as again this varied considerably by patient. The average estimated time in clinic for patients with a F2F appointment was around 95 minutes, excluding travel time.
Question 27. Considering Upgrade to Recipient model in your clinic, please indicate in the table below the average duration, staff involved and facilities used for each of the identified tasks from a patient perspective.
Based on responses from 2 clinics the U2R tasks took 15 to 40 minutes for the patient to download the app and unpack the kit and another 10 minutes to watch the video. One clinic additionally offered a 40-to-60-minute telephone consultation with a speech and language therapist.
Overall Experience (Q22 and Q28-Q31)
Question 22. Comparing the U2R model vs. face-to-face upgrade appointments at your clinic, how would you rate the following statements?
When comparing the models, positive responses were generally given for the U2R being more convenient, more sustainable, saves time and costs for patient travel, reduces staff resources and storage space. Less positive responses were given for comparable quality of service to clinic appointments and as a substitute for clinic appointments (Figure 6). Additional comments made in open text are provided in Supplemental Appendix B.
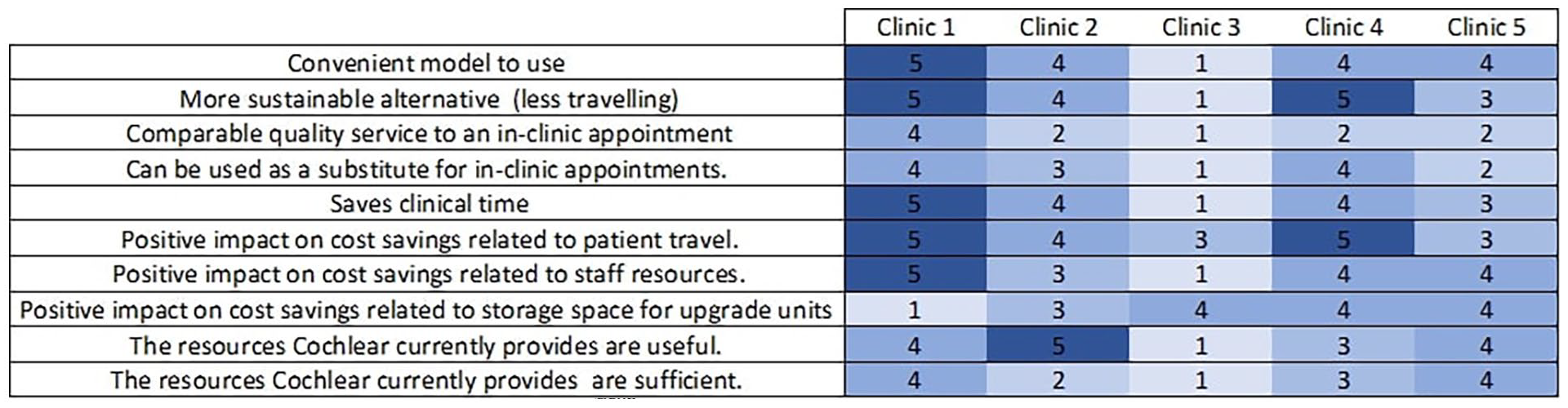
Answers to question 22: Comparing the U2R model versus face-to-face upgrade appointments at your clinic, how would you rate the following statements? Satisfaction ratings are given for each clinic from 1 to 5, where 1 is strongly disagree and 5 strongly agree. A score of 3 is neither agree nor disagree. A score of 1 is shaded light blue and 5 dark blue.
Question 28. What have been your key learnings and best practices using U2R? (on items like implementation, information governance, protocols development, change management)
Question 29. Where do you feel the U2R service can be further improved, if at all?
Open comments from each clinic are reported in Supplemental Appendix B for suggested improvements and any key learnings. Overall, more administration was required than expected and procedures must be optimised for the model to succeed. For some patients U2R works well, but for others it is very challenging, and participants must be chosen carefully. One comment was that “despite the time and cost savings, I still feel that the patients who attend F2F get a better deal, although the U2R patients probably don’t realise this.”
More resources to troubleshoot problems remotely and better quality-control of processor programming by the company were requested by the clinics. Better labelling of items within the kits sent to patients might reduce the feeling of being overwhelmed when it arrives.
Question 30. How satisfied are you with U2R?
Question 31. How likely are you to recommend U2R to other hospitals/colleagues?
Figure 7 gives score for how satisfied clinics were with the U2R model overall and how likely they would be to recommend it to another clinic (both ratings were the same for all clinics). The Four clinics were generally satisfied but Clinic 3 was not and would not have recommend it to another clinic in the form trialled within this study. This clinic has worked with Cochlear to improve the workflow and responsibilities and continues to use U2R in their daily practice.

Overall satisfaction ratings for the U2R model and the question “how likely are you to recommend to another clinic” ratings were given on a scale of 1 to 10 where 10 is satisfied and 1 not satisfied.
Discussion
The study shows how a medical device manufacturer can be used to provide remote care, interacting directly with patients in a B2C model to reduce clinical workload. The implementation of the B2C model required device manufacturers, health care providers, regulators and payers to work together as described by Grustam et al. (2018). 9 The results and success of the model are discussed using the six areas proposed by Herzlinger (2006) 7 and explored by Grustam et al. (2017) 10
The Structure and Players Involved
The structure of the model implementation varied hugely between clinics. The staff involved ranged from ATOs in some clinics to senior audiologists in others and there was no reported difference in the categories of staff between the F2F and U2R models for the tasks they had in common. This was true even for clinics within the same country. All the clinics reported that their protocols for implementation changed over time as they became more experienced. Although initially some staff were sceptical, experience and familiarity with the process positively influenced their opinions. Further streamlining of the U2R process and an improved allocation of staff resources would be beneficial to consider, with greater consensus across clinics of the minimum skill sets required for each task. The company are a key player in the structure of the model and provided its services free of charge, with the expectation that a greater number of upgrades could be purchased overall by the participating clinics.
Financing and Cost Savings
The U2R model saved substantial time per patient per clinic ranging from 21 to 65 minutes. This saved time was from device counselling and programming new sound processors, which was allocated to audiologists, speech therapists, and clinical scientists. These tasks also used rooms which are often in high demand such as soundproof booths and consulting rooms. Therefore, this saved time potentially represents a large cost saving to the clinic for the U2R model compared to a F2F appointment. However, the time spent on patients returning for follow up appointments or trouble shooting reduced this time and cost saving. There was also a large saving in the patient’s time and costs as they no longer needed to travel to the clinic. In non-paying health care systems, as was the case here, the use of cost saving models does not have a negative effect on clinics’ finances. However, there may be impacts on funding structures that should be considered and addressed in other settings before the model is implemented.
Effective Technology
The Custom Sound Pro software provided by the company used to transfer the data was an established piece of software. Nonetheless, clinics did report that errors in programme transfer to the new sound processor and the correct equipment being included in the kits were made. These were most likely due to human error, but it still may be possible to avoid them with technology innovation. Confidence in the accuracy of data represent one of the barriers to the acceptance of telehealth in general. In addition, better instructional videos, guidance, and support for the patient once the sound processor kit is received would facilitate the process and reduce the need for patients to return to the clinic.
Implications for Public Policy
This limited model had no impact on public policy, but more research and peer reviewed publications in this area will help to provide an evidence base for moving towards innovative healthcare solutions.
Consumers
The consumers in this case are the patients, parents, guardians, and/or carers themselves and the high uptake rates of 80% to 100% across clinics would indicate that the U2R model was successful. However, in some clinics patients were not given the choice between F2F or U2R appointments. Clinics made a careful selection of patients for the U2R service and for some this resulted in it being offered to less than 40% of patients. Clinicians reported that the patients who had accepted to use the U2R system were generally satisfied and positive. However, patient satisfaction with the U2R service was not directly measured and this would be required to give confidence that consumers were entirely happy with the change of service delivery. Other studies looking at tele-audiology have reported good levels of patient satisfaction and largely positive experiences. 12 The high return rate of patients to the clinics would indicate that patient confidence in the quality of the U2R service was low and this must be addressed before it is implemented in the wider population.
Accountability
Finally, the clinics were still accountable for the interaction with the patient. Each had their own system for ensuring that the right data protection safeguards were in place and that the right permissions for personal data sharing had been obtained from the patient. Successful management of the patient confidentiality and data privacy issues was key to the model’s implementation. 1
To our knowledge this is the first example of the proposed framework being applied to a real scenario in a hospital setting. The results go some way towards confirming that the B2C model is viable and creates value for both patients and the service providers. Although the U2R model was acceptable across the six factors identified by Herzlinger, a relatively low percentage of U2R upgrades took place compared to the number of upgrades still done face to face. A high proportion of patients were not offered the service initially and this varied across clinics with some not offering U2R to older adults or children and others using it for all their paediatric upgrades. Some of the barriers to be addressed were concerns over loss of face-to-face patient interaction and worries about the patients’ abilities to handle the technology. These challenges are common across many eHealth solutions and similar concerns were also expressed about the loss of patient interaction when considering remote audiology.6,21,22 However, self-fit hearing aids, where patients acquire their hearing aids directly from a business, and not through a clinician, and then fit them themselves at home, are already in use across many countries with acceptable outcomes for most. 23
The reduction in the need for face-to-face interactions with the clinic is a key aim of these models and technologies. Confidence in their effectiveness both for clinicians and patients must be built if they are to be used more widely. Key staff were trained in the implementation of the U2R model, and the process was reviewed, discussed, and adjusted with staff and the company. 6 This contributed to ensuring that the system was implemented smoothly, but some concerns were still expressed that the quality of the service provided with the U2R was not the same as the F2F and that the time spent in administering the U2R may be better spent caring for the patient face to face. 6 Ensuring that any remote interactions and support are high quality can assist in clinician’s addressing these concerns. Successful implementation of remote health care requires considerable training and a specific set of digital health care competencies. 21 The greater use of remote programming could solve some of the connectivity, device pairing and equipment issues specified as the main reasons for patients returning to clinic. The Cochlear Remote Assist enables clinicians to make certain limited adjustments to patient’s sound processor programmes remotely by connecting the fitting software to the recipient’s sound processor via a smartphone app over the Internet. 24 This has been proven to be successful as an alternative to face-to-face visits for 80% of routine CI programming sessions and in combination with the U2R model may solve some of the problems encountered. 24 The continued building of clinicians’ confidence in these new models of service provision is key to their wider acceptance. It would be beneficial to seek further information from the patients in the future about how they found the process and what their suggestions are for improvement. Also, consideration should be given of how long a patient should go without any face-to-face appointment where a physical assessment of the device placement and surgical site can be made.
Limitations
The study was descriptive in nature and only represents the view of the small number of clinics who are already using U2R in their practice. Different results might be found with clinics from other countries or patient age profiles. Only one clinician from each clinic completed a questionnaire representing the whole clinic’s views rather than results being collected and collated from multiple clinicians. All clinics applied selection criteria to the types of patients invited to participate in the U2R model, excluding those who may have found the process harder. The time saved does not account for the time required to set up the system or any of the transaction costs involved in negotiating and implementing the new system.
Conclusions
The study shows how a manufacturing company can be used to provide remote care in a business to customer model, interacting directly with patients to reduce clinical workload.
Large savings in clinic and patient costs and time were achieved. The implementation of the model varied hugely from clinic to clinic, with staff involved ranging from assistant technical officers in some clinics to senior audiologists in others. Future improvements would be to further streamline the process within clinics and provide better remote support for patients to solve equipment issues and provide reassurance without the need to return to the clinic. This would ensure that time savings are maximised and the B2C model provides comparable quality to an in-clinic appointment.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251332569 – Supplemental material for Clinical Time Savings and Experiences Using a Business-to-Customer Model for Cochlear Implant Sound Processor Upgrades
Supplemental material, sj-docx-1-inq-10.1177_00469580251332569 for Clinical Time Savings and Experiences Using a Business-to-Customer Model for Cochlear Implant Sound Processor Upgrades by Jane Bradley, Wendy J. Huinck, Angella Fuller, Martin O’Driscoll, Lorna Whitehouse, Andrew Soulby and Paula Greenham in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to acknowledge the invaluable contributions of the dedicated teams at each clinic for their efforts in implementing the U2R model and facilitating data collection. Special thanks go to Ana Bordonhos and Chris James from Cochlear for their support throughout this project.
Ethical Considerations
No ethics approval was required as no patient data was accessed, collected, or reported for this study. Guidelines were followed as laid out by the UK Health Research Authority (![]() ) and guidelines from the Dutch Central Committee on Research Involving Human Subjects (https:/english.ccmo.nl/investigators/legal-framework-for-medical-scientific-research/your-research-is-it-subject-to-the-wmo-or-not). All authors except PG had access to patient data as part of their clinical roles. The study was conducted in accordance with the local requirements.
) and guidelines from the Dutch Central Committee on Research Involving Human Subjects (https:/english.ccmo.nl/investigators/legal-framework-for-medical-scientific-research/your-research-is-it-subject-to-the-wmo-or-not). All authors except PG had access to patient data as part of their clinical roles. The study was conducted in accordance with the local requirements.
Consent for Publication
The clinics and clinicians that participated in the study provided consent for publication.
Author Contributions
Conceptualisation, JB, WH, AF, MOD, LW, AS, PG; methodology, JB, WH, AF, MOD, LW, AS; formal analysis, PG; investigation, JB, WH, AF, MOD, LW, AS; data curation, PG; writing—original draft preparation, PG; writing—review and editing, JB, WH, AF, MOD, LW, AS, PG; visualisation, PG. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by Cochlear Ltd. The funder participated in the research design, analysis, interpretation, and reporting of the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PG holds consultancies with Cochlear Ltd, Advanced Bionics Ltd. and Med El Ltd. WH has received travel support from Cochlear Limited for workshop attendance.
Data Availability Statement
Data is available on request by email from cjames@cochlear.com at Cochlear Ltd.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.