
Abstract
Healthcare organizations increasingly engage in activities to identify and address social determinants of health (SDOH) among their patients to improve health outcomes and reduce costs. While several studies to date have focused on the evolving role of hospitals and physicians in these types of population health activities, much less is known about the role health insurers may play. We used data from the National Longitudinal Survey of Public Health Systems for the period 2006 to 2018 to examine trends in health insurer participation in population health activities and in the multi-sector collaborative networks that support these activities. We also used a difference-in-differences approach to examine the impact of Medicaid expansion on insurer participation in population health networks. Insurer participation increased in our study period both in the delivery of population health activities and in the integration into collaborative networks that support these activities. Insurers were most likely to participate in activities focusing on community health assessment and policy development. Results from our adjusted difference-in-differences models showed variation in association between insurer participation in population health networks and Medicaid expansion (Table 2). Population health networks in expansion states experienced significant increases insurer participation in assessment (4.48 percentage points, P < .05) and policy and planning (7.66 percentage points, P < .05) activities. Encouraging insurance coverage gains through policy mechanisms like Medicaid expansion may not only improve access to healthcare services but can also act as a driver of insurer integration into population health networks.
Keywords
Healthcare organizations increasingly engage in activities to identify and address social determinants of health among their patients to improve health outcomes and reduce costs, however, little is known about the role insurers may play.
We found that communities in states that expanded Medicaid had significant increases in insurer participation in the delivery of policy and assessment-oriented population health activities.
Encouraging insurance coverage gains through policy mechanisms like Medicaid expansion may not only improve access to healthcare services but can also act as a driver of insurer integration into population health networks, thereby increasing the population health protections available in a community.
Introduction
Addressing the social and environmental factors influencing health outcomes has emerged as a promising and increasingly popular strategy to improve outcomes in the United States (US).1,2 Individuals with unmet social needs, such as food and housing insecurity, inadequate childcare, low education/health literacy, unmet economic, mental/behavioral health, and transportation needs, are more likely to experience adverse health outcomes, accrue greater health care costs, and have decreased life expectancy.3 -6 Increasingly, insurers and clinical providers are incorporating population health activities that are designed to identify and address patient social needs alongside their clinical care. 7
Health insurers have strong incentives to invest in population health activities if these are effective in lowering healthcare utilization and costs because any savings produced will accrue primarily to insurers. In contrast, hospitals and physicians stand to financially benefit from population health activities only to the extent that these activities (1) reduce the costs of caring for uninsured patients or (2) help providers earn higher revenues under value-based payment models that reward improved outcomes and reduced costs for their insured patients. The Affordable Care Act (ACA) may have strengthened insurer incentives to engage in population health activities by increasing the number of people enrolled in health insurance coverage, particularly since newly enrolled individuals were more likely to come from low-income and minority population groups with complex medical and social needs.8,9
Medicaid and Medicare programs have emerged as early adopters of population health approaches to address their enrollees’ complex medical and social needs.7,10 -12 These approaches include programs to screen for unmet social needs, refer to community-based social service providers, support electronic communication and information exchange between medical providers and social service agencies, and build networks of community health workers, social workers, and navigators to help patients access needed services.10 -13 Recent federal programs like the Centers for Medicare and Medicaid Services State Innovation Models and Accountable Health Communities initiatives have encouraged the development and testing of these approaches.7,14,15 However, despite growing enthusiasm for population health initiatives to address social determinants of health, existing studies suggest that implementation challenges are common and clear evidence of effectiveness in improving health outcomes and reducing costs remains elusive.7,14,16 -19
Insurers may engage in population health strategies independently or through strategic cross-sector partnerships with other community organizations. Participating in collaborative networks may allow insurers to support a broader range of population health activities and share the costs of these activities with other community organizations. 20 Prior work by Mays et al found increases in insurer participation over a 16-year period in cross-sector networks that implement a comprehensive set of population health capabilities. 21 Nevertheless, insurers historically have engaged in these networks at significantly lower rates than many other sectors, including local and state health agencies, hospitals, schools, and faith-based organizations.20 -23 We build on this earlier work by examining how insurers participated in networks and what factors may be associated with changes over time, particularly after the implementation of Medicaid expansion. While several recent studies have focused on the evolving role of hospitals in population health initiatives, less is known about the role insurers play and how this has changed over time.24 -28
This study provides the first assessment focused on longitudinal trends in insurer engagement in population health activities. We leveraged data from a nationally-representative study of population health activities in 360 communities to examine changes over time in insurer participation in population health networks, focusing especially on how participation may be associated with changing health insurance coverage. We hypothesize that localized health insurance coverage gains associated with Medicaid expansion may have acted as catalysts for increased insurer engagement in cross-sector population health networks.
Methods
Study Design and Data Sources
We used 2006 to 2018 data from a sample of 360 US metropolitan communities to examine trends in insurer participation in cross-sector delivery of population health activities. The National Longitudinal Survey of Public Health Systems (NALSYS) uses a validated questionnaire to collect information from local public health officials on the delivery of 20 population health activities in their communities (see Table 1 for full list).20 -23,26,29 Questions in the survey address a broad set of activities recommended by national guidelines that are considered key in promoting and improving population health.30 -34 NALSYS activities align with the 3 core functions of public health and range from community-level initiatives such as assessing health status, needs, and behavioral risk factors to ensuring individuals are linked to the appropriate health and social services.
Longitudinal Trends in Insurer Contributions to Population Health Activities, 2006 to 2018.
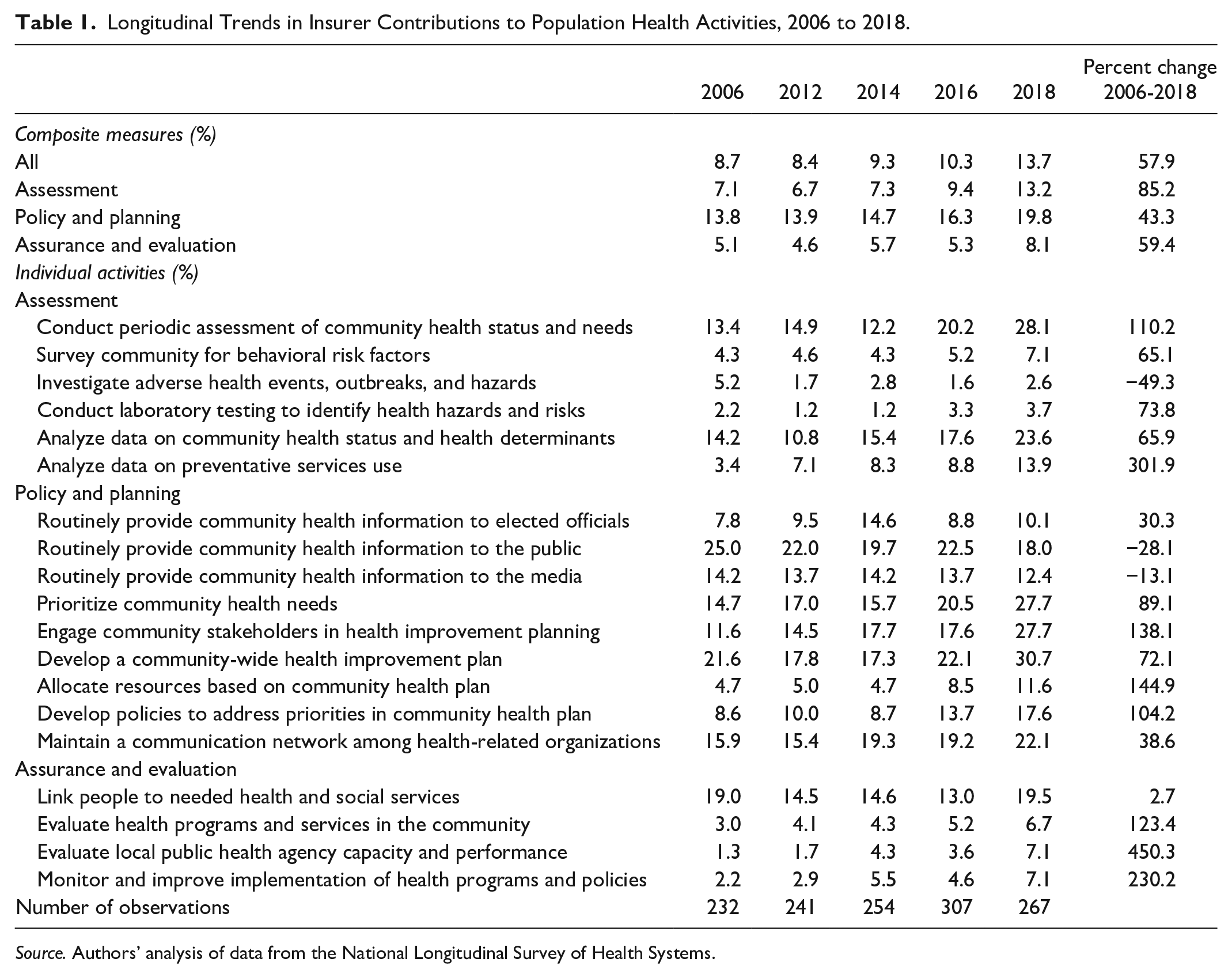
Source. Authors’ analysis of data from the National Longitudinal Survey of Health Systems.
The NALSYS survey asks local public health officials to report whether or not each population health activity is implemented in their community and, if so, the network of organizations that participate in implementing each activity. Insurers are 1 of 13 types of organizations that respondents report as participating or not participating in each activity. Prior validation work confirmed that local public health officials are reliable sources of information about the population health activities included in the survey and about the organizations that help to implement these activities. 31 One current challenge in the field is the distinction between community-oriented population health initiatives and activities and population health management strategies that target individuals. Because NALSYS focuses on activities implemented in the community at large through multi-sector partnerships as reported by local public health officials, the survey may not capture narrowly-targeted population health activities such as programs offered by single institutions for restricted panels of patients or health plan members.
NALSYS is the only nationally-representative data source with longitudinal information about population health activities implemented in US communities. These data were first collected in 1998, with subsequent waves of collection in 2006, 2012, 2014, 2016, and 2018. This study used data from 2006 to 2018. We linked NALSYS data from each year with information on community socioeconomic, demographic, and health care system supply characteristics from the Area Health Resources File (AHRF). 35 For most communities in NALSYS, the public health jurisdiction represents a single county, facilitating a one-to-one match with AHRF. A small subset of jurisdictions are multi-county. For these communities, we created a weighted average of the AHRF variables based on population size.
Study Population
Our study population included 360 communities with populations of 100 000 or more. These communities are primarily metropolitan counties and include about 70% of the population in the US. NALSYS response rates range from 68 to 92 % over the period of this study. We excluded communities where respondents did not report complete information about insurer participation (n = 89). Our final analytical sample included 410 communities and 1212 community-year observations in an unbalanced panel. Our analytical sample did not differ significantly from the full NALSYS sample on key measures included in this study (measures of insurer engagement; see Supplemental Table 1).
Outcome Measures
We used the NALSYS survey data to construct 5 summary measures of insurer participation in the population health activities referenced in the survey. First, we constructed 3 separate measures of the types of participation by grouping the 19 public health activities into 3 categories representing policy activities, assessment activities, or assurance activities and then calculating, for each category, the proportion of activities in which insurers participated. We use 19 activities instead of 20 when looking at sector engagement because the 20th activity asks about the implementation of legally mandated activities and is unrelated to collaboration
For the final 2 participation measures, we used social network analysis (SNA) methods to measure insurer participation relative to all other organizations supporting population health activities within each community. Calculation of these network participation measures followed standard SNA network definitions using previously used methods to characterize patient-sharing networks among healthcare providers.36 -38 Rather than measuring the number of patients shared between each pair (dyad) of providers in a community, we measured the number of population health activities shared between each pair (dyad) of organizations in a community. First, we measured insurer degree centrality by examining the subset of dyads that involve insurers, calculating the sum of all activities shared by these insurer-dyads, and then dividing by the sum of all activities shared by all dyads in the community. This measure indicates the relative contribution of insurers to the full network of organizations that support population health activities in the community. Next, we measured insurer betweenness centrality by examining the activities shared among all possible combinations of 3 organizations (triads) that involve insurers in the community. Within each of these insurer triads, we calculated the sum of activities that insurers share with each of the 2 other organizations in the triad. Then we determined whether this sum exceeds the sum of activities that these 2 organizations share directly with each other. If so, we designated these triads as insurer-enhanced triads because insurers contributed additional shared activities into the triad above and beyond the activities shared between the 2 other organizations. The measure of insurer betweenness centrality indicates the proportion of insurer-triads that are insurer-enhanced, which reflects the potential of insurers to broker stronger activity-sharing relationships between other organizations in the community. These measures of insurer participation in community networks characterize the health insurance sector at large and do not differentiate among market segments such as ACA marketplace plans, employer-purchased insurance plans, Medicaid plans, and Medicare Advantage plans.
Statistical Analysis
Our initial analyses focused on characterizing longitudinal trends in insurer participation in population health networks. We also examined patterns of insurer participation in the individual NALSYS activities over time to capture more granular information on engagement trends. Building on these descriptive analyses, we used a difference-in-differences approach to examine the association between changes in insurer participation in networks and Medicaid expansion. Population health networks in states that expanded Medicaid served as our control group and were compared to networks in nonexpansion states. We used 2014 as our treatment year for most states, but allowed the indictor year to vary for those states that expanded after January 1st, 2014.
We ran separate multivariate linear regression models for each outcome of interest. We included year and state fixed effects in each model to control for unobserved differences across time. We also clustered standard errors at the state-level. Each model controlled for community-level hospital beds per capita, physicians per capita, number of federally-qualified health centers, population size, population density, income per capita, unemployment rate, racial composition, percent of the population over age 65, and percent living below the federal poverty line. These variables were selected based on previous work examining population health networks.
Sensitivity Tests and Analyses
We tested for parallel trends both visually by graphing descriptive data for the insurer outcome measures and analytically by estimating year-specific time trends in expansion and nonexpansion states using pre-expansion data (Figure 1 and Supplemental Table 2). We also tested additional models excluding states in the sample that had substantial early expansion (NY) and did not expand on January 1st, 2014 (IN, LA, MI, PA).

Longitudinal trends in insurer contributions to population health activities in expansion and nonexpansion states (%), 2006 to 2018.
Results
The total proportion of population health activities insurers participated in increased from 8.7% in 2006 to 13.7% in 2018 (Table 1). The most substantial gains in insurer participation were concentrated in activities in the assessment category—with insurer engagement increasing by 85%. Across all years, insurers participated in policy and planning activities at the highest rate and assurance and evaluation activities at the lowest rate. However, we found significant variation in all composite measures, with some communities reporting insurer participation in up to 85% of activities and others reporting none.
Insurer participation in the implementation of individual population health activities increased from 2006 to 2018 in almost all of the activities, with the exception of providing community health information to the public and the media and the investigation of adverse health events (Table 1). Insurers participate in activities that target assessing community needs and developing community health improvement plans at the highest rates. Almost 20% of communities reported insurer engagement in linking individuals to needed health and social services, and 22.1% indicated they maintain a communication network among health-related organizations. Insurer participation in the analysis of data on community health status and determinants and the allocation of resources based on the community health plan increased by over 300% between 2006 and 2018. Not surprisingly, insurers contributed toward the investigation of adverse health events and lab testing to identify health hazards and risks at the lowest rate.
We also found changes over time in how insurers engaged in population health networks with community partners. Both insurer degree and betweenness centrality decreased from 2006 to 2012 (Supplemental Figure 1). The centrality measures were then relatively stable or increasing slightly between 2012 and 2016, with more substantial gains from 2016 to 2018.
Results from our adjusted difference-in-differences models showed variation in association between insurer participation in population health networks and Medicaid expansion (Table 2). Population health networks in expansion states experienced significant increases insurer participation in assessment (4.48 percentage points, P < .05) and policy and planning (7.66 percentage points, P < .05) activities. Insurer degree centrality also increased by 3.36 percentage points (P < .10) in expansion states compared to nonexpansion. We did not find significant differences between expansion and nonexpansion networks in insurer participation in assurance and evaluation activities or insurer betweenness centrality.
Difference in Differences Analysis of Insurer Participation in Population Health Networks in Medicaid Expansion and Nonexpansion States, 2006 to 2018.

Source. Authors’ analysis of data from the National Longitudinal Survey of Health Systems (2006-2018) linked with the Area Health Resource File.
Note. Pre includes 2 time periods (2006, 2012), post includes 3 (2014, 2016, 2018). Model includes 1212 observations. All models include state and year fixed effects and control for community socioeconomic, demographic, and health care supply characteristics. Standard errors are clustered at the state-level. PP stands for percentage point. **P < .05, *P < .10.
Sensitivity Tests and Analyses
Results from our adjusted parallel trends analyses suggest that all outcomes measures meet the parallel trends assumption (Supplemental Table 2), despite seeing some evidence of differing pre-trends in the visual map (Figure 1). We also found our main model results to be robust against varying our inclusion and exclusion criteria (Supplemental Table 3).
Discussion
Our results indicate that insurer participation in the delivery of individual population health activities and insurer connections with other sectors increased between 2006 and 2018. Insurers were more likely to participate in activities falling into the policy and planning category, suggesting an orientation toward population health initiatives that prioritize community health needs and develop policies to address those needs. Indeed, the substantial increase in insurer participation in the assessment and analysis of community health status and determinants points to an interest in understanding population characteristics and needs. By working collaboratively with other members of the population health network, insurers stand to better understand enrollee health and social needs and where disparities might exist. Building strong connections between sectors can also facilitate linkages that ensure enrollees receive the services best suited to meet their needs, thereby improving health outcomes and reducing the cost of care.
Significant increases in insurer participation in population health networks were associated with Medicaid expansion, suggesting that implementation of ACA policies targeting greater coverage rates to traditionally underserved populations may have triggered insurer engagement in population health activities. In alignment with our descriptive results, we found that significant increases were concentrated in policy and planning and assessment activities. While our study results suggest a relationship between Medicaid expansion and increased insurer engagement in population health, we did not explore all the components of ACA that may have contributed this change, such as private health insurance subsidies and regulations and hospital community benefit activities that may have helped patients gain and maintain insurance coverage. Future research further exploring additional ACA’s mechanisms and how they are driving population health adoption and integration would be beneficial.
Results from our study align with and reflect the growing emphasis on the importance of addressing the social determinants of health among payers. Research in this area is still emerging, but most findings to date suggest insurer engagement in this space is primarily focused on screening for unmet social needs in enrollees and referral to community-based partners to address needs.10 -12 Our study examined patterns of engagement in broader community-level population health activities, adding to the understanding of how insurers engage in population health initiatives. We also found that insurers in Medicaid expansion states are assuming more central roles in the delivery of population health activities and playing an important role in connecting other organizations into multisector population health networks. Future research using additional years of NALSYS data may capture additional trends while also measuring long-term insurer commitment to population health, especially during and following the COVID-19 pandemic.
Despite increasing engagement from 2006 to 2018, insurers remain one of the least engaged sectors in population health networks, consistent with earlier research.20 -23 These results suggest substantial room exists for greater insurer engagement in population health networks. In part, low levels of insurer engagement likely reflects the historic orientation of the sector. In the past, insurers were responsible for providing coverage but did little else in the communities they served. As mentioned above, insurers have only recently shifted their attention toward efforts to address population health outcomes. Future research should focus on identifying and evaluating the potential impact of other policy levers for increasing insurer engagement. Multisector collaboration has been identified as a mechanism for more efficient and effective delivery of population health activities.21,39 Both insurer financial resources and data on the enrollee population can potentially bring additional added value to population health networks.
Limitations
Several limitations to our study should be considered. First, our sample was restricted to primarily urban communities with a population of 100 000 or more, limiting our generalizability. Although the NALSYS sample was expanded in 2014 to include smaller communities, we focus only on those communities also in the 2006 and 2012 samples to allow us to examine changes in insurer engagement before and after Medicaid expansion. Additional years of NALSYS data to investigate trends in insurer participation in rural population health networks could offer a more robust picture of their engagement across US communities.
Second, NALSYS data does not distinguish between insurers serving different segments of the health insurance marketplace, such as the individual market, small-group and large-group employer markets, Medicare Advantage, and Medicaid Managed Care. Incorporating additional data on insurer market segments in local communities may reveal variations in how different types of insurers contribute to population health networks. Additionally, NALSYS measures the relationships between insurers and other community organizations, but it does not assess the quality of these relationships. Some insurers may have stronger relationships in the population health networks, while others may be superficial. Future studies employing mixed methods could capture more detailed information on the quality of insurer engagement in population health networks. Finally, NALSYS data are collected from the perspective of the local public health official and may not capture all population health activities in which insurers are participating, such as narrowly targeted initiatives for individual health plan members. However, as noted in the method section, previous validity assessments of NALSYS have found that local public health officials capture multisector activities with accuracy.
Third, our analysis examines insurers and networks during a time period before the onset of the COVID-19 pandemic. This allows us to examine long-term patterns of participation that are not driven by the pandemic’s unique and unprecedented disruptions, yielding findings that may be more applicable to non-emergency circumstances. In future work, it will be important to investigate the pandemic’s temporary and lasting effects on population health networks.
Conclusions
The results from this cohort study suggest that insurers are increasing their participation in population health networks and playing a greater connecting role among organizations in those networks. Additionally, we found that Medicaid expansion may help drive insurer integration into multisector population health networks. Increased insurer engagement has the potential to strengthen cross-sector population health networks and may result in downstream improvements of health outcomes and equity.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241249092 – Supplemental material for Longitudinal Trends in Insurer Participation in Multisector Population Health Activities
Supplemental material, sj-docx-1-inq-10.1177_00469580241249092 for Longitudinal Trends in Insurer Participation in Multisector Population Health Activities by Rachel Hogg-Graham, Teresa M. Waters, Emily R. Clear, Kendall Pearson, Joseph A. Benitez and Glen P. Mays in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author Contributions
All authors meet the requirements for authorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from the Robert Wood Johnson Foundation through the Systems for Action National Program Office, ID 75708.
Ethical/Consent Statement
This study was reviewed and determined exempt by the University of Kentucky Institutional Review Board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.