
Abstract
This research aims to gain an in-depth understanding of precariously housed women’s experiences related to health and access to health care during the COVID-19 pandemic using a grounded theory approach. Qualitative data were obtained through interviews with 17 precariously housed women from Izmir, Turkey. Poor health among most participants was primarily attributed to unfavorable living conditions and weakened community networks. The COVID-19 pandemic exacerbated existing health issues due to barriers in accessing basic needs. Food insecurity was widespread during the pandemic and the critical role of aid and the inadequacy of social assistance in securing food were emphasized. Women’s health perceptions were significantly shaped by gender, and gendered caregiving duties have restricted women’s healthcare access. Access to healthcare was also limited by financial challenges, with health insurance being a crucial determinant. Longer waiting times, often exacerbated by the appointment system, and language were significant barriers to healthcare access. The findings propose that the participants were precarized by the blindness of COVID-19 measures to vulnerabilities, which resulted in deeper inequalities in housing, food, employment, and healthcare access. This research addresses the political, commercial, and social determinants of precariously housed women’s health. Improving precariously housed women’s health and wellbeing requires implementation of public policies targeting to improve housing quality, provide targeted assistance to food insecurity, promote gender inclusiveness, and foster gender empowerment.
Keywords
Precarious housing, particularly prevalent among women, is associated with increased exposure to infections, chronic diseases, and delayed healthcare utilization, as observed during the COVID-19 pandemic.
This research provides insights into the specific challenges faced by precariously housed women during the COVID-19 pandemic, highlighting the interlinks between factors such as housing conditions, gender roles, and other social determinants of health, thus emphasizing the urgent need for targeted policies to address these issues and improve healthcare access and outcomes for this population.
The implications include advancing a feminist perspective, underlining the importance of community resilience, addressing economic and social barriers to healthcare access, and addressing the need for policy measures tailored to the unique circumstances of precariously housed women during public health crises like COVID-19.
Introduction
Precarious housing is a comprehensive concept related to living conditions, characterized by instability, uncertainty, and insecurity in terms of tenure, housing conditions and affordability.1 -3 Precariously housed people are more likely to be exposed to infections and have chronic diseases. 4 Similarly, during the COVID-19 pandemic, a concentration of infections and deaths in places with socioeconomic disadvantages and unfavorable housing conditions was observed.5,6 The surfacing inequalities in housing during the COVID-19 pandemic required an altered approach to housing which included standard housing deprivation criteria as well as living space, technology, environment, and neighborhood, and economic stress. 7 When a specific group is subjected to increased vulnerability to injury and death due to the absence of essential economic and social support, which also includes support related to housing in this case, precariousness transforms into precarity, a condition that is inherently political in nature.8,9 The COVID19 pandemic has resulted in a global state of precarity in areas such as employment, housing, and food, where measures were not centered on equity.
Women constitute a significant proportion of the precariously housed 10 and they spend more time in an environment of health risks because of the gendered norms that also limit physical access to healthcare, employment opportunities, or other services. Several studies indicated negative health outcomes of precarious housing on both physical and mental health of women. 11 Pandemic conditions may have exacerbated the challenges for women, as the increased time spent at home, economic hardships, and elevated caregiving responsibilities could disproportionately impact them. The overburdening of healthcare services during the pandemic may have further worsened the already limited healthcare access for women in precarious housing. Access to healthcare is influenced by factors such as health needs, economic status, and availability of hours. Consequently, it can be contemplated that women find themselves under the dual burden of deteriorating health conditions and worsening access to healthcare services. It was reported that even though women had poorer conditions than men, the number of studies addressing the effect of gender on housing and health is limited. 11 The studies which examine the intersection of gender with other types of inequities in housing are also lacking. 12 Although 34.7% of the population in Turkey live in housing with at least 1 criterion for housing deprivation and 40% live in overcrowded households, there has not been an adequate number of studies evaluating gender in housing and health during the COVID-19 pandemic.13,14 However, it is important and necessary to identify the barriers faced by precariously housed women while accessing healthcare during health crises such as the COVID-19 pandemic, as well as to reveal the societal gender roles, housing, and other social determinants of health that play a role in access processes, and the interlinks between them, in order to implement more effective interventions more urgently in future crisis situations. Therefore, we aimed to explore how precariously housed women perceive their health, interpret determinants of their health status, including housing conditions and navigate different phases of accessing healthcare during the COVID-19 pandemic, contextualizing them within the broader socio-economic and political contexts through the lens of gender and social determinants of health framework. 15
Materials and Methods
This phenomenological qualitative study was conducted in Basmane neighborhood in Izmir, Turkey, where housing deprivation is common. Basmane houses several primary care facilities that provide care without any co-payments. There are also migrant health centers (MHC) and extended migrant health centers (E/MHC) that provide a linguistically and culturally appropriate primary care for Syrian refugees. E/MHCs also provide specialty care such as internal medicine, pediatrics, and obstetrics and gynecology (OBGYN). Additionally, 3 public hospitals and 1 public dental hospital were located close to the region.
Snowball sampling was used, and the first participant was reached through the Street Soup Makers Aid Association (SSMAA). The interviewer-researcher attended the activities of the SSMAA twice a week 1 month before the interviews started, during which she had the opportunity to introduce herself and the research. The activities took place twice a week along the same route where participants’ homes were located. Therefore, upon being informed during the initial encounter, participants could express their interest in the research to interviewer-researcher in subsequent activities. Other participants were reached through those already interviewed, a key person recommended by interviewed participants, and another organization in the same neighborhood, Konak Refugee Association. Being self-identified as a woman, experiencing housing deprivation, being 18 years or older, residing in Basmane, and agreeing to participate in the research were considered necessary for inclusion in the study. Exclusion criteria included having a communication barrier due to mental or physical health issues, refusing audio recording, or discontinuing the interview. Observatory visits to the houses of the participants were performed to assess eligibility prior to the interviews. EU-agreed indicators of housing deprivation, overcrowding, tenancy as well as affordability was assessed during these visits. The presence of 1 indicator was considered sufficient for housing deprivation. 16 Having less than 1,5 rooms per person was accepted as overcrowded housing. 17 Housing was considered affordable if the expenditure on adequate housing was less than 30% of the household income. 18 Participants were recruited until the data reached saturation and 17 women were included. No new code emerged after the twelfth participant. Data saturation was evaluated across the entire dataset, and participant recruitment process continued to reach a more heterogeneous group in terms of characteristics such as income, insurance, and education levels. As data saturation had already been achieved, and participant recruitment was continued solely to reach a more heterogeneous group, the researchers agreed to discontinue participant recruitment after the 17th participant based on the distribution of participants’ sociodemographic characteristics and previous studies in the literature. 19
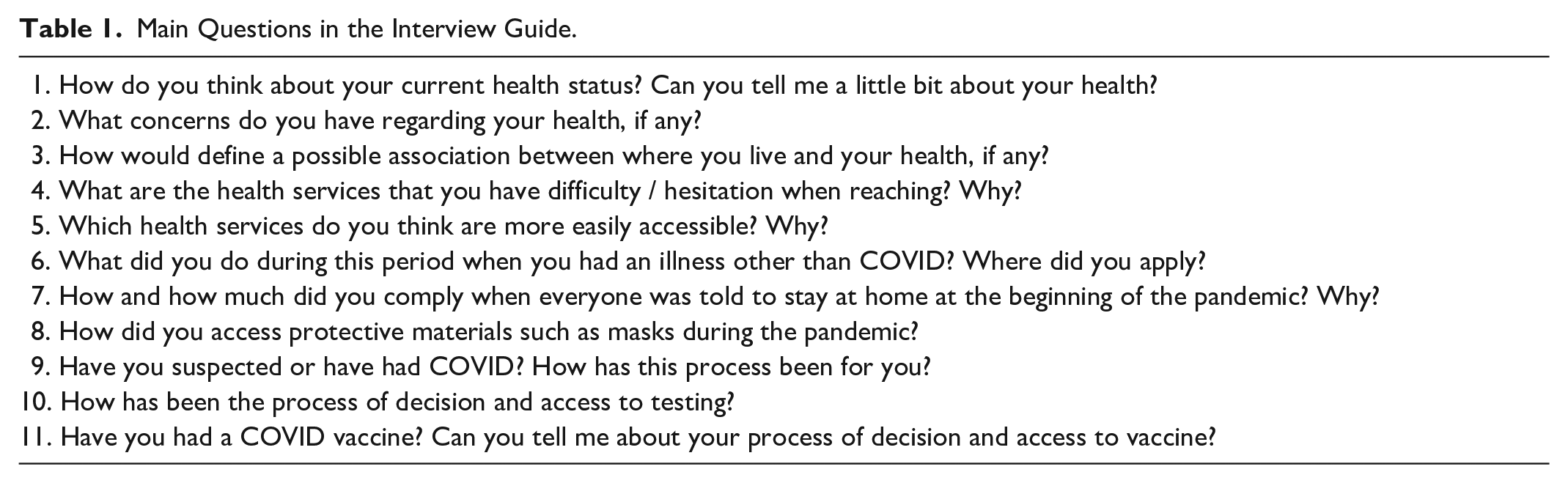
Data were obtained through semi-structured in-depth interviews held in the participants’ homes between May and August 2022 and audio-recorded. All the interviews were carried out by the same researcher who was also involved in the participant recruitment. An interview guide was formed based on a behavioral model in healthcare utilization 20 and included questions related to perceived health status and its relation to housing, health concerns, challenges, and facilitators in access to health care during the COVID-19 pandemic. (Table 1) Two pilot interviews were conducted in April to assess the clarity of the questions. The pilot interviews were not included in the analysis. The interview language was determined by the participants and interpreter support for Arabic was received when needed. The interviews lasted 30 minutes on average.
Main Questions in the Interview Guide.
Audio recordings were transcribed verbatim. Data analysis was conducted based on grounded theory, and open, axial, and selective codes were used in line with the model of Strauss and Corbin. 21 Initially, 62 open codes were identified. The consistency of the coding was verified by a continuous comparison of the later codes with the existing codes. Subsequently, axial and selective codes were identified. The second author who has years of experience in qualitative research methods re-read all the codes and related citations and proposed changes that were later discussed in detail by the researchers until an agreement based on re-evaluation of the literature was reached. In situations where two researchers cannot reach a consensus, they strove to select the most suitable codes for research questions by considering the study’s aim and objectives, literature, and the perspective of social determinants of health. 15 The researchers chose to either merge the codes that they could not reach an agreement on, ensuring the preservation of meanings or defer to the decision of the more experienced researcher in unresolved cases, which was rare. All data were reprocessed using the agreed codes. This involved identifying both selective codes, which encapsulate broader themes, and axial codes, which categorize specific aspects within those themes. Ultimately, 3 overarching selective codes were pinpointed: Living Conditions and Health, Social Characteristics and Health, and Barriers to Healthcare Access and Utilization. Within each of these selective codes, 9 axial codes emerged, representing distinct categories such as Inadequate Housing, Food Insecurity, and Lack of community perception in the neighborhood under Living Conditions and Health. Similarly, Gendered priorities and Religion as a coping strategy surfaced as axial codes under Social Characteristics and Health. Additionally, axial codes such as Financial challenges, Less available appointments and longer waiting times, Service provider characteristics as a determinant in service utilization, and Language barrier were identified under Barriers to Healthcare Access and Utilization. In prioritizing these themes, the frequency of code recurrence was considered, along with the alignment of themes with the steps and factors in The Aday-Andersen Behavioral Model of Health Services Utilization. 20 Therefore, the categories that formed the themes, were consistent with the theoretical framework of the study and semantic integrity of the data.
Ethical approval for this study was obtained from the Ege University Medical Research Ethics Committee. (Reference Number: 22 - 4T/25) The participants were informed about the research process and their written informed consent was obtained.
Results
Sociodemographic characteristics of the participants are presented in Table 2. Three themes and 9 categories were identified. Age and initials of education status (N: Non-literate, P: Primary School, S: Secondary School, H: High school, and U: University) were used to address the citated participants.The quotes for each category are presented below their respective paragraphs.
Sociodemographic Characteristics of the Participants.
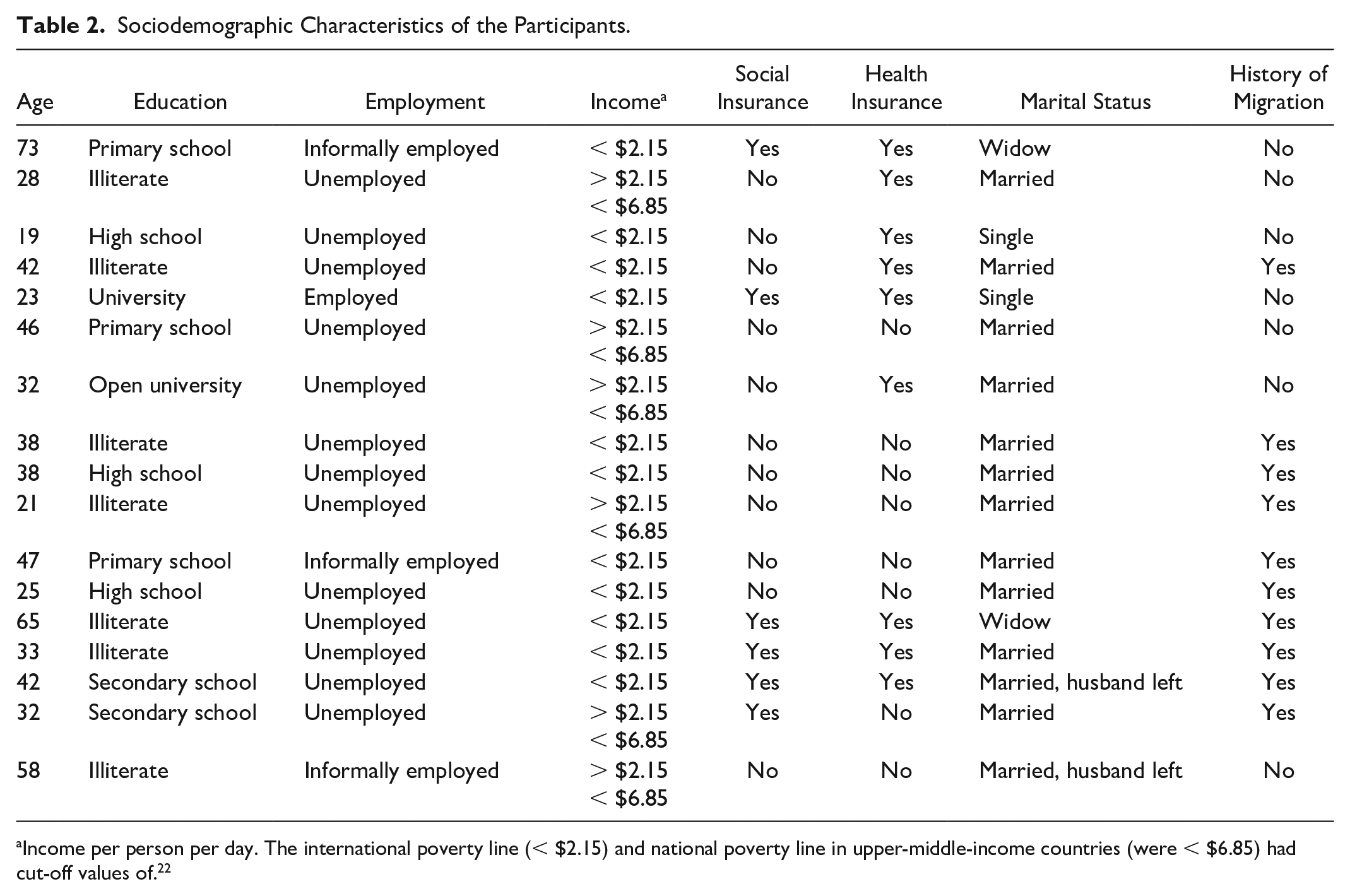
Income per person per day. The international poverty line (< $2.15) and national poverty line in upper-middle-income countries (were < $6.85) had cut-off values of. 22
Living Conditions and Health
Most participants (12/17) complained of poor health, which they defined as a state of illness brought in by unfavorable living conditions and weakened community networks, instead of having a disease. Health was perceived more as a social concept by the participants, and the determinants of health proposed by Dahlgren and Whitehead 15 were also addressed. Inadequate housing, food insecurity and lack of community perception in the neighborhood were mostly referred to. The COVID-19 pandemic was expressed as an exacerbator of an already poor health status due to the barriers in accessing basic needs and mental challenges related to uncertainty.
Inadequate Housing
Inadequate housing is considered a strong predictor of respiratory disorders. Dampness and mold, heating, and inadequate personal space were the 3 aspects of inadequate housing where the relationship between housing and health was perceived by the participants, with specific emphasis on economic conditions.
“In winter, my children had to stay in bed for a month due to the flu. There was no stove, and the electric stove is expensive. They were always in bed in the cold times.”
Dampness and mold were perceived as threats to respiratory health and an exacerbators of respiratory symptoms. Protecting oneself from COVID-19, an essentially respiratory disease, ironically meant being obliged to spend a longer time in a housing which was perceived risky for respiratory health by the participants.
Sustaining access to heating was difficult and primarily dependent on charity and aid. When no aid was received, using blankets, couch-surfing for heating, and improvising combustible items such as paper and clothes were solutions resorted to.
“We burnt our clothes because the state did not provide coal during the COVID-19 pandemic.”
Inadequate space is a major concern due to the risk of SARS-CoV2 transmission. The presumption that self-isolation could not be properly implemented if the test showed positive results was cited as the reason for some participants’ reluctance to be tested. One participant reported inadequate space and dampness as reasons for non-compliance with the lockdown regulations.
“We are living with 10 people in a two-room house; it has been very challenging.”
“I had a severe flu,. . ..but when they wanted to test me at the hospital, I ran away (. . .) My home is as much as you see; where will I stay, where will I isolate, so I didn’t take the test.”
Food Insecurity
Participants reported widespread food insecurity, which they attributed to both their deteriorating economic status and rising food prices during the pandemic. Thus, food insecurity became a category in which social and commercial determinants of health were articulated and aid became a crucial means of obtaining food.
“We were starving. My husband could not go to work. No jobs were available during the COVID-19 pandemic. We did not receive any food; it was like death.”
Lack of Community Perception in the Neighbourhood
The majority of the participants indicated that many people in the neighborhood have had COVID-19. While there is a significant consensus on this, there are primarily 2 different interpretations regarding the role of the neighborhood in experiencing COVID-19. According to the first interpretation, the risk was universal, and nothing distinguished the neighborhood from other areas.
“The disease was worldwide, not just here. The whole world was affected. I think everywhere was risky.”
In the second interpretation, the reason why many people in the neighborhood had COVID-19 was attributed to the individual behaviors of the residents, such as disregarding personal protective equipment (PPE) and social distancing measures. The participants described the residents as irresponsible yet separated themselves from other residents. The neighborhood was usually perceived as an already polluted area in this interpretation.
“Nobody wears a mask here, but I wear. They did not wear a mask when the pandemic was severe and were never concerned. That’s why most of them became sick.”
Social characteristics and health
Gendered priorities
Gender had a significant impact on how the participants perceived health, which was highly apparent by the prioritization of the health of the husband. Most participants were unemployed (14/17) (Table 2) and their husbands were the sole income earners in the household. Health and continued employment of the husband were considered as essential for the family to sustain itself.
“ I have an illness, and when COVID-19 emerged, my doctor stressed the importance of staying at home for my health. However, my immediate concern at that time was, 'Oh no, my husband won’t be able to work. What will we do?”
Economic empowerment through training in skills to increase family income is commonly required. However, the demand for economic empowerment was not free of gender stereotypes, as it was restricted by the home and the neighborhood, essentially due to the gendered caregiving duties. Training is also expected to increase social interactions within the neighborhood to create a social capital. The immigrant participants requested Turkish lectures.
“The women here, we need something like this (trainings). We are always at home, available to come, for a different organization.”
Caregiving responsibilities have increased health concerns and limited access to healthcare. “Nowhere to leave the child” was notably limiting the health service utilization, especially by the participants with younger children. Having no one to take care of the children in the case of illness was expressed as a health-related concern.
“Sometimes my left side hurts, from my fingertips down to my foot, and that’s why I’m scared. I want to see a doctor for this pain, but I don’t have anyone to leave my child with.”
Religion as a coping strategy
Older participants perceived religion as a means of self-healing and a coping strategy against health-related anxieties and also considered faith as a preventive measure against COVID-19.
“When I think about whether I will become bedridden in the future, I immediately start praying to God to protect me from losing my feet; and from becoming helpless.”
Barriers to healthcare access and utilisation
Financial challenges
Health insurance is a crucial determinant of access to healthcare, intersecting citizenship. Many participants depended on their husbands’ employment for their health insurance. Less comprehensive insurance coverage and out-of-pocket payments were obstacles to accessing treatment and were a reason for financial hardship.
“There was never enough money. (referring to the treatment of pulmonary embolism) We accumulated a lot of debt. My husband said that he could not pay it in the end.”
One participant explained why she had to pay out-of-pocket for the limited treatment she could access due to lack of insurance, despite the ever-increasing drug prices, addressing the commercial determinants of health:
“It is hard for those without insurance. I can only take painkillers because I cannot visit a doctor and I do not know any other drugs. They increase the drug prices a lot, even if it is sold for 30 liras, we will still buy them, it relieves the pain. We have no option, we will buy it even for 40 liras.”
Concerns regarding insurance have resulted in limited access to the testing. Even though the test was offered free, the participants without insurance felt anxiety caused by hypothetical extra spending due to hospitalization or prescriptions in case of being positive for COVID-19.
Many participants faced challenges accessing PPEs for economic reasons. Social assistance was an essential way of getting PPEs, but it was neither sufficient nor continuous. In addition to economic challenges, PPEs have become difficult to find and expensive because of the rapid and high demand during the first wave of the COVID-19 pandemic.
“Masks and disinfectants were unavailable for a while, there weren’t any in the markets. Just like we cannot easily get sugar or flour right now. It was like famine.”
The financial challenges in accessing masks and hygiene materials necessitate management with limited resources, resulting in the inappropriate use of materials.
“There was one cologne. We had to put water in it because it was very expensive. Disinfectants were very expensive and getting one was hard because no one was working. I bought a mask once, but I did not get it for free. I was washing the masks every day (Single-use masks).”
Less available appointments and longer waiting times
According to many participants, the appointment system poses a challenge to accessing health services. Long waiting times were the most frequent criticism of the appointment system by participants. The appointments were managed either by phone or online, rendering the process more challenging for some participants. The appointment system in hospitals has been cited as a reason for the increased utilization of emergency and primary care services.
“For example, if one is sick, and cannot have an appointment, does one have to die? Most of the time, I could not get an appointment for an examination. Therefore, we cannot reach health too.”
Service provider characteristics as a determinant in service utilization
Previous experiences with the health workers were found to affect adherence to treatment and the utilization of health services. Trust seemed to facilitate adherence to treatment and the utilization of services, such as vaccination, during the pandemic. Phone-call follow-ups by family physicians during the pandemic also had a positive impact.
Immigrant participants experienced challenges accessing secondary and tertiary healthcare institutions; therefore, they applied to E/MHCs. E/MHCs, which the participants preferred because of their proximity, did not have OBGYN specialists. Consequently, the participants had to go to more distant E/MHCs and wait for a longer time.
“I would like to have a gynaecologist in the health centre. There are (gynaecologists) in Karabaglar, but it is too far, and one has to go at 4 o’clock and wait for a long time.”
Language barrier
Language is a barrier to accessing health services, leading to the increased utilization of E/MHCs as the first point of contact with the health system. Other reason cited for the increased use of E/MHC were long waiting times due to insufficient number of interpreters in secondary healthcare facilities. Thus, although E/MHCs seem to have an advantage with their staff providing services in Arabic, challenges in other institutions remain unresolved.
“I prefer the health center (E/MHC); because it is closer and not crowded. Also Arabic is spoken there.”
“When we go to the hospital, they tell us there’s no interpreter, and they can’t proceed with the examination.”
Discussion
The findings of this study, which aimed to gain an in-depth understanding of precariously housed women’s experiences related to health and access to health care during the COVID-19 pandemic, suggest that precariously housed women perceive poor health and have limited access to health care.
“Living Conditions and Health” describes experiences of precariousness in terms of housing, food, neighborhood and identifies COVID-19 pandemic as an exacerbator for precariousness. Precariousness dominated the health-related narratives of the participants instead of disease complaints, despite the interviewer’s physician identity, indicating the priority and severity of the issues raised. Through this theme, it is observed that participants’ perception of health is significantly shaped by the precariousness they experience. Biomedical and economic definitions of health with an individual focus, shaped under Western capitalism, are profoundly inadequate in this context, as they lack neither a social nor political perspective.23,24
Food insecurity was widespread among the participants, in line with the observed increase in food insecurity globally during the COVID-19 pandemic due to deteriorating economies and supply chain disruptions.25,26 Our findings are also consistent with the findings of a study conducted in 103 households living in deep poverty in Istanbul during the pandemic, in terms of prevalence of food insecurity. 27 In the same study, similar to our findings, it was observed that households working in daily jobs, who were already living in poverty before the pandemic, began to experience food insecurity due to sudden job loss. 27 Both studies demonstrate how economic conditions determine access to food for at-risk groups. Access to food is highly dependent on aid, which varies in terms of quality, content, amount, and frequency; thus, equity cannot be ensured. Unstandardized delivery of the aids for heating and hygiene was also observed.
In neoliberal countries, response strategies to food insecurity are largely centered on food aid and charity. 28 Aids relieve some of the severe needs; however, they also have significant disadvantages. Aid-based relief causes depoliticization of the food and diminishes the government’s responsibility to ensure access to adequate food as stipulated under international human rights law. 29 Another disadvantage is the inability to control the food aid content, which may worsen the feeling of a lack of control caused by the precarious living conditions. In addition, spatial differences in the availability of food aid further deepen inequalities.30,31 Considering the high inflation rate of food and energy prices in Turkey, 32 aid-based strategies may no longer be sustainable.
Epidemics have rendered the relationship between housing and health more prominent throughout history. 33 Housing, a means of prevention, has also frequently posed a threat to those living in inadequate or overcrowded housing, as also expressed by the participants of this study. 34 The emphasis on the individuals in COVID-19 measures did not recognize the structural barriers to complying with these measures.35,36 Many participants assumed that their housing characteristics increased respiratory illnesses and were concerned about the risk of transmission due to overcrowding; however, they had to comply with the stay-at-home regulations. Thus, it can be argued that the blindness of the measures to vulnerabilities resulted in a form of precarity and increased social and socio-spatial inequalities. 37 Despite evidence regarding the association between precarious housing and higher COVID-19 mortality and morbidity, precariously housed people were not prioritized in any European country in terms of testing, treatment, or vaccination. 38 Ayala et al 7 argued that the concept of housing precariousness, which had already tended to expand before the COVID-19 pandemic, should be further expanded in light of what we have learned from the COVID-19 pandemic. The unmet needs identified in this study also support the need for a broader concept.
The reasons cited for the perceived high COVID-19 density in the neighborhood were evaluated in the 2 groups. While the first group did not identify any prominent neighborhood characteristic as a reason, the second group cited the irresponsible behavior of the residents as the reason and marginalized them as “others” while separating and defending themselves. Both groups can be considered as everyday representations of responses to spatial stigma related to COVID-19. Following the internalization of spatial stigma, 2 separate defense mechanisms were developed in line with Wacquant et al’s work39,40 on severe marginalization. Whereas the first group resisted stigmatization with indifference, the second group submitted to it through coping strategies, such as retreating into private space, distancing, and defensive othering, thus reproducing the stigma in everyday life. 41 Therefore, in this study, neighborhood stigma constituted a major challenge to community cohesion, which is a keystone in building social resilience against precariousness.
Women’s roles in social reproduction had negative consequences for their health, both by affecting other determinants of health and restricting access to health services. In a study conducted using data from the Turkish Statistical Institute in 2018, it was found that women residing in areas with higher levels of unemployment, urbanization, and a higher percentage of ethnic minorities feel less empowered, hence the demands for empowerment among women in our study can be interpreted in this context. 42 Training on skills that can be conducted at home or in the neighborhood to increase family income was requested in many studies; however, the reason behind the request differed.43 -45 Women in the lowest socioeconomic group demanded a place where they could participate in production and marketing processes together as a strategy to cope with financial challenges, and at the same time maintain their daily reproduction roles, which is consistent with the findings of this study. 44 Demand is limited to the home and neighborhood as the influence of patriarchal stereotypes and social reproduction roles continues. However, there are also studies indicating that women continue to primarily identify themselves as mothers and spouses even if they work. 46 Again, it is observed that women prioritize their children, 46 while, in our study, besides children, the spouse’s health is also prioritized. At this point, the fact that the majority of participants in our study do not work may have been influential. The relevance of the socialization of housework and childcare for women’s empowerment and health has once again emerged. Economically empowered women are better able to make their health-related decisions and have better healthcare access47 -49,and women who take part in women’s cooperatives, which is a similar form of empowerment suggested by this study’s participants, feel economically, psychologically, and socially more empowered, even facing political and societal challenges. 50
Participants mostly utilized primary care services and had challenges in accessing secondary care institutions due to income, coverage, and appointment systems, as the literature suggests.51 -54 Therefore, primary healthcare plays a health equity-producing role. Although primary healthcare is crucial in eliminating inequalities, as referral care is a component of health, challenges at this stage also remain crucial. 55 Unavailability of the required specialist care can cause other challenges in accessing healthcare such as distance and long waiting times, as expressed by the participants.
Insurance is a significant financial barrier to access to healthcare. Turkey has been implementing the general health insurance system since 2006, through which the health insurance of most of the population covers. 56 According to the Turkish Demographic Health Survey (TDHS), 9% of women do not have any health insurance coverage, and women living in the most deprived households are less likely to have any kind of health insurance. 57 This may explain the high number of participants without health insurance in this study. Even though Atun et al 56 propose a significant expansion of coverage for the most deprived, concerning the findings of this study and TDHS, 57 more effort is needed to provide insurance to women in the most deprived communities.
Refugees have the right to social security at the same level as citizens of the country of asylum, according to the Convention Relating to the Status of Refugees, 58 in which Turkey is a signatory. The Turkish government has taken steps to provide healthcare to registered refugees with similar coverage to Turkish citizens through MHCs and E/MHCs, which are organized under the Turkish Ministry of Health and aim to provide free, linguistically, and culturally appropriate primary care to refugees under temporary protection. 59 TDHS conducted in a Syrian refugee sample, 60 reports that 93% of Syrian women in Turkey has health insurance but does not include any segregation by deprivation. Although Turkey has made significant progress in the healthcare provision for refugees, some regulations that came into force in the later period, such as limiting the social insurance coverage to the city of residence determined by the Ministry of the Interior, and practical challenges could have resulted in limited access. 52 A regulation published in 2019, 61 requires Syrian refugees who have been in Turkey for more than a year to pay their social insurance. The short period between the publication of the regulation and its enactment before the COVID-19 pandemic also had negative consequences on access to healthcare. 52 Concerning undocumented immigrants, even though universal access to primary and emergency care is guaranteed, many practical challenges exist, such as the healthcare registry system and limited information related to services. 59 This exemplifies why immigrants who are not integrated into the social, health, and economic systems of countries are considered an important precarity group experiencing inaccessibility, less protective networks, and continuous insecurity.
In MHCs, the removal of the language barrier facilitated refugee women’s access to healthcare; however, the challenges in other healthcare institutions remain unresolved, rendering MHCs a parallel organization rather than an integrated 1, which can also result in further disintegration and exclusion of Syrian refugees. The benefits of the service provision in Arabic and a culturally appropriate environment were appreciated by the participants, but alternative ways to support adequate and appropriate services in existing institutions should be encouraged toward a more socially integrated healthcare delivery.
Long waiting times are indicators of the functioning of the health systems. The rate of unmet medical needs in Turkey is reported to decline, and only 1.9% of the population has to forego a medical examination due to cost, distance, or waiting times. 59 Although it is acknowledged that the people in the poorest income quintile experience more unmet medical needs compared with the richest quintile in international reports, the findings of this study suggest that the scope of the challenges concerning waiting times can be more frequently experienced. 62 A more demand-oriented primary care system without an appropriate referral chain may have resulted in an increased demand for hospital care, resulting in unavailability of appointments and long waiting times. A study described the Central Physician Appointment System as unsustainable if a mandatory referral chain or reorganization based on demand is not taken into effort, consistent with our findings. 63
The commercial determinants of health have been referred to repeatedly, noting how commercial interests and the market have a decisive influence on health, even in a humanitarian crisis setting. Commercial determinants also include the gradual abandonment of needs-based service allocation with health reforms to pave the way for the privatization of health and the prominence of profit and demand-based service allocation. 64 Thus, they are in close relationship with financial barriers in access to healthcare and longer waiting times.
All participants encounter obstacles at various stages of healthcare access; however, the complexity of these barriers intensifies for certain individuals who concurrently experience multiple forms of disadvantage. For instance, while most participants expressed a demand for courses aimed at economic empowerment, refugee participants concurrently requested language courses. Challenges such as prolonged waiting times are ubiquitous among most participants, with uninsured individuals additionally grappling with the escalating costs of medications. The unique insurance coverage practices and language barriers pertinent to refugees added further layers of complexity. In this milieu, the depth of inequalities experienced by participants in their access to healthcare is shaped by the housing, immigration, and insurance statuses.
Limitations
This study attempted to address unequal health outcomes of housing precariousness, thus including participants from different age groups with various educational, employment and citizenship statuses. The use of interpreter support in interviews with 8 participants in the study constitutes a limitation. While the interpreter support contributes to the inclusion of participants with diverse cultural backgrounds, potential losses in meaning may have occurred due to the absence of exact Turkish equivalents for certain words. Additionally, non-verbal communication elements might not have been adequately represented in the translation. Interpreters may not always be fully familiar with the cultural context of the participants, which can affect the accuracy and sensitivity of translation. Certain cultural nuances or references may be lost or misunderstood, impacting the depth and accuracy of the data collected. In order to mitigate these challenges, we provided a detailed briefing to the interpreters prior to the interviews.
This study’s findings are based on a small specific sample from Basmane, which also poses a limitation regarding the generalizability of the findings. Further studies in other neighborhoods where housing precariousness is common could improve our understanding of different aspects of health-related experiences.
Snowball sampling method was preferred due to the challenges in reaching the target population and inherent vulnerabilities within the target population. Snowball sampling can introduce a selection bias as a non-probabilistic method of sampling, leading to a homogenous sample. Therefore, our mitigation strategy was to diversify our recruitment sources by later incorporating a local key person and involving a different NGO in the participant recruitment process. Additionally, we tried to ensure diversity among participants by including individuals with varying ages, educational backgrounds, and citizenship statuses, aiming to prevent the findings from solely reflecting the characteristics of a very limited group.
The interviewer-researcher’s regular attendance at activities of the SSMAA may have led to rapport bias, where participants may feel pressured to respond in a certain way due to their familiarity with the interviewer. However, the interviewer-researcher had a training in qualitative research methods, including techniques for maintaining neutrality and minimizing the influence of personal biases during interviews. Professional boundaries were maintained during the interviews and confidentiality was ensured.
Conclusions
The precariousness experienced by participants worsened during the COVID-19 pandemic, leading to poorer perceived health and restricted access to healthcare.
This study provides insights into how gender roles shape the health conditions and healthcare access of women in precarious housing. Women’s access to healthcare is adversely affected by factors such as constraints to private space, childcare responsibilities, and the inability to achieve economic independence. Lower educational attainment, immigration status, or the combination of both exacerbated the challenges, demonstrating intersecting influences on access. The study, adopting a feminist perspective, identifies areas where intersectionality is observed as urgent intervention domains.
To improve precariously housed women’s health and wellbeing, public policies addressing inadequate housing should be implemented and gender sensitive support programs to improve housing quality should be developed. Targeted social assistance programs to address food insecurity which prioritize collaboration with local communities could help securing food. The starting point for such policies may be a rapid needs assessment. Therefore, it is imperative to promptly identify houses that meet the definition of precarious housing in the area, engage in interviews with women living in these houses to conduct a needs analysis, and based on this analysis, tailored strategic action plans should be prepared. Transparent and accountable geographically distributed service hubs can be established, financially supported, and supervised by local governments, incorporating the connections, experience, and trust built by civil society organizations, to respond to the various precarious situations of these women. To achieve universal healthcare access, measures to promote gender-inclusive and culturally sensitive care should be taken. Training programs for healthcare professionals should include modules aimed at enhancing their cultural competency, with a specific focus on providing patient-centered and women-centered care. Cultural mediators should be integrated into the services offered across all healthcare facilities, and efforts should be made to increase the employment of interpreters while ensuring equitable distribution among institutions. Political, social, and economic factors shaping health are interconnected and by tailoring interventions to the needs of the women, policymakers can contribute to fostering healthier and more resilient communities. Still, there is a need for more studies involving women from diverse regions and cultural backgrounds to prepare crisis action plans that are more responsive and have a capacity for rapid response to needs, with greater inclusivity and involvement of researchers from various academic disciplines.
Footnotes
Acknowledgements
We are thankful to Safak Taner, Zeliha Ocek and the Street Soup Makers Aid Association for their contributions to this study. We are also grateful to the Ege University Planning and Monitoring Coordination of Organizational Development and Directorate of Library and Documentation for their support in editing and proofreading services of this study.
Data Availability
The qualitative data used to support the findings of this study were restricted in order to protect patient privacy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Ethical approval for this study was obtained from the Ege University Medical Research Ethics Committee. (Decree No. 22-4T/25)
Informed Consent
The participants were informed about the research process and their written informed consent was obtained.