
Abstract
Introduction:
Teaching is a stressful occupation due to high-stake job demands and limited resources, which were exacerbated during the initial phase of the COVID-19 pandemic. Our study assessed the prevalence of perceived stress and explored its predictors among elementary school teachers employed at schools serving predominantly low-income populations in five cities in the United States.
Method:
Our study analyzed the data among selected schools that were collected through the Brighter Bites teacher survey which comprised items measuring sociodemographic characteristics, perceived stress, perceived general health, food insecurity, and concerns regarding social determinants of health needs. The predictors of perceived stress were examined using generalized linear mixed models (GLMMs) with schools as the random variable.
Findings:
A total of 685 teachers were included in the analysis (84.9% female, 38.1% Hispanic, 57.6% <5 years of teaching experience). Most (85.4%) of the teachers stated they were stressed “sometimes”/“often.” Results from adjusted GLMM showed that teachers who were food insecure (adjusted odds ratio [AOR]: 2.33, confidence interval [CI]: [1.63, 3.35]), those who had concerns regarding financial stability (2.68 [1.91, 3.75]), food availability (1.69 [1.15, 2.48]), food affordability (2.27 [1.57, 3.28]), availability/affordability of housing (2.21 [1.33, 3.67]), access to childcare (1.76 [1.06, 2.92]), and access to a clinic/doctor (1.60 [1.10, 2.33]) were at significantly greater odds of reporting perceived stress.
Conclusion/Application for Practice:
Our study demonstrates the heightened impact of COVID-19 on the mental well-being of teachers across a wide range of social needs. Stress management and additional social service programs are suggested to support teachers to mitigate pandemic impact.
Keywords
In the United States, the COVID-19 pandemic caused by SARS COV-2 has been responsible for pervasive morbidity and mortality as seen globally (World Health Organization, 2020). The preventive measures implemented to combat the pandemic, such as quarantine and school closures, have increased concerns of insecurity and isolation, potentially causing long-lasting mental health effects in the population (Usher et al., 2020). The mental well-being of schoolteachers, in particular, may have been affected due to alterations in education delivery (Khlaif et al., 2021; Ozamiz-Etxebarria et al., 2021; Popa et al., 2020). Diliberti and colleagues (2021) found that among teachers who were surveyed in the American Teachers Panel, the primary cause of attrition was pandemic-related stress caused by insufficient pay, health risks (associated with COVID-19), childcare responsibilities, instructional challenges, and inadequate safety plans. About 75% of the teachers stated that they “often” or “always” felt stressed even before the pandemic. The pandemic exacerbated the effects by increasing working hours and decreasing sleep time. Thirty-three percent of teachers reported work hours increasing from 52 to 56 hours or more per week, and the teachers who had less sleeping time (<8 hours/day) increased from 74% to 83% (Diliberti et al., 2021). Other pandemic-related reasons such as job furlough, food insecurity, caring for family members, and balancing work and personal life compounded their stress levels (Diliberti et al., 2021; Ozamiz-Etxebarria et al., 2021). In addition, literature has consistently reported an association between perceived stress and adverse health behaviors such as increase in alcohol consumption, less efficacy to quit smoking, physical inactivity, as well as poor physical health such as stomach ulcers and high blood pressure (Ansley et al., 2016; Ng & Jeffery, 2003).
Although there is emerging literature on the impact of the COVID-19 pandemic on teachers across the United States, there is limited data on those employed in schools serving low-income minority populations (Diliberti et al., 2021; Khlaif et al., 2021; Ozamiz-Etxebarria et al., 2021; Popa et al., 2020; Usher et al., 2020). These schools have historically struggled with a lack of adequate resources and a high-need population. The pandemic further exacerbated these struggles (Christakis, 2020; Dooley et al., 2020). The purpose of our study is to address this gap in the literature by assessing the prevalence of perceived stress and examine its association with social determinants of health needs among the elementary school teachers during the initial phase of the COVID-19 pandemic. The teachers were employed at schools serving low-income children and their families implementing Brighter Bites across six regions in the United States.
Brighter Bites is an evidence-based, school-based nutrition program that provides a weekly distribution of fresh produce and nutrition education to schools serving low-income populations. The program is implemented for 16 weeks in the school year and 6 weeks in the summer across Houston, Austin, Dallas, New York City, Washington, D.C., and Southwest Florida, among schools where more than 75% of the children are participating in the free/reduced lunch program (Sharma et al., 2015, 2016). Due to COVID-19-related school closures, Brighter Bites programming came to a halt in March 2020 concurrently across all cities. During this time, Brighter Bites conducted surveys with participating parents and teachers to help determine subsequent programming efforts to support the families and schools (Almohamad et al., 2020; Haidar, Markham, et al., 2021; Sharma et al., 2020). The results of the teacher surveys are presented as part of our study.
Methods
Research Design and Study Participants
Brighter Bites is a 501c3 nonprofit organization that implements a coordinated school health program consisting of produce distribution and nutrition education in schools serving predominantly low-income children and their families across six regions in the United States. Due to COVID-19-related school closures, Brighter Bites programming was suspended in March 2020. A cross-sectional self-report survey was administered to all employed teachers at schools enrolled with Brighter Bites during the 2019–2020 school year. The surveys were administered to 3,068 teachers across 90 schools (percentage of teachers by region: 54.05% in Houston, 12.84% in Austin, 21.38% in Dallas, 5.15% in Washington, D.C., and 6.58% in Southwest Florida). Although the program was implemented in six regions, data were collected from five cities; NYC was excluded as we did not receive permission from the NY education board to conduct surveys with the parents. The University of Texas Health Science Center at Houston (UTHealth) administered the survey electronically, using Qualtrics (Provo, UT). UTHealth is the program evaluation partner for Brighter Bites and has a data use agreement with the nonprofit organization. Survey completion was voluntary and informed consent was obtained prior to the start of the survey. The study protocol and methodology were approved by the UTHealth Committee for Protection of Human Subjects Institutional Review Board.
Data Collection Measures
Sociodemographic measures including self-reported sex (male/female), years of teaching experience (0–5 years, 6–10 years, 11–15 years, 16–20 years, >20 years), race/ethnicity (non-Hispanic White, African American, Hispanic, Others), and area of residence (Houston, Austin, Dallas, Washington, D.C., and Southwest Florida) were collected from all the participants.
Perceived stress was measured using a self-reported single-item question, “In the last two months, due to COVID-19 and related challenges (e.g., school and childcare closures, online teaching, and other personal challenges) how often have you felt nervous and ‘stressed’?” (Thorsen et al., 2019). A 5-point response scale was used ranging from “never” to “very often” (Cohen et al., 1983). For the analysis, the response options were collapsed to three categories: never (never/rare), sometimes, and often (often/very often).
Perceived general health of the participants was measured using a pre-validated single-item measure, general self-rated health (GSRH), “In general, would you say your health is . . . ?” (DeSalvo et al., 2006). Responses were recorded on a 5-point scale ranging from “poor” to “excellent.” These response options were collapsed for analysis to poor (poor/fair), good, and excellent (very good/excellent).
Food insecurity was measured using a previously validated two-item questionnaire, the Hunger Vital Sign (Hager et al., 2010). “You worried whether your food would run out before you got money to buy more,” and “The food you bought just didn’t last and you didn’t have money to get more.” A 3-point response scale (never true, sometimes true, and often true) was used. The individuals who selected “sometimes true” or “often true” for either question were classified as food insecure.
Concerns regarding social determinants of health, including financial stability, employment status, availability of food, affordability of food, availability and affordability of housing, access to reliable transport, access to childcare, and access to a clinic/doctor were measured using a single question, “Due to COVID-19, are you concerned about any of the following in regard to you and your family? (Choose all that apply).” The responses for each item were coded as 0 (No) and 1 (Yes).
Statistical Analysis
All analyses were performed using SAS Studio software, version 3.8 (SAS Institute Inc., Cary, NC). Frequency distributions and percentages were calculated for all variables. Variation of perceived stress by sex, food insecurity, and concerns regarding social determinants were examined using Cochran–Armitage trend test; years of experience and perceived general health were examined using Spearman Correlation, and race and city were examined using Rank Biserial test. Univariate and multivariate generalized linear mixed models (GLMMs) were used to determine the association between perceived stress and the social determinants of health variables. A mixed model was used to consider the two-level structure of the data, that is, the nesting effect of the teachers within the schools. Schools were modeled as a random effect in the analysis. In this model, perceived stress was measured as the outcome variable, and only those predictor variables that were significantly associated with the outcome variable were included in the analysis. City, race, and years of experience were used as covariates. The significance level (α) was set at .05.
Results
A total of 862 teachers from 76 schools responded to the survey (response rate of schools: 84.4%, response rate of teachers: 28.10%, response rate of teachers by region: 31.90% in Houston, 27.73% in Austin, 19.14% in Dallas, 10.67% in Washington, D.C., and 10.32% in Southwest Florida). The analyses included a total of 685 teachers who responded to the perceived stress question. Participants were predominantly female (84.9%), Hispanic (38.1%), with less than 5 years of teaching experience (57.6%). Approximately 85% of the teachers reported perceived stress; 37.7% of teachers stated they were stressed “sometimes” and 47.7% were stressed “often” in our sample. Less than half of the participants (43.6%) reported having good general health, and 29% of the teachers were food insecure. Most of the respondents (75%) expressed concerns regarding one or more social determinants of health.
Table 1 demonstrates the stratification of the predictor variables by perceived stress. Results of Cochran–Armitage trend test showed statistically significant gender differences (p <.0001) in perceived stress. Significant differences in perceived stress levels were noted with respect to food insecurity (p <.0001), concern regarding financial stability (p <.0001), availability of food (p = .031), affordability of food (p <.0001), availability and affordability of housing (p = .004), access to childcare (p = .007), and access to a clinic/doctor (p = .003). Spearman’s correlation demonstrated significant differences in perceived stress by years of experience (p = .009).
Characteristics of Teachers Participating in the Brighter Bites Teacher Survey by Perceived Stress (N = 685)
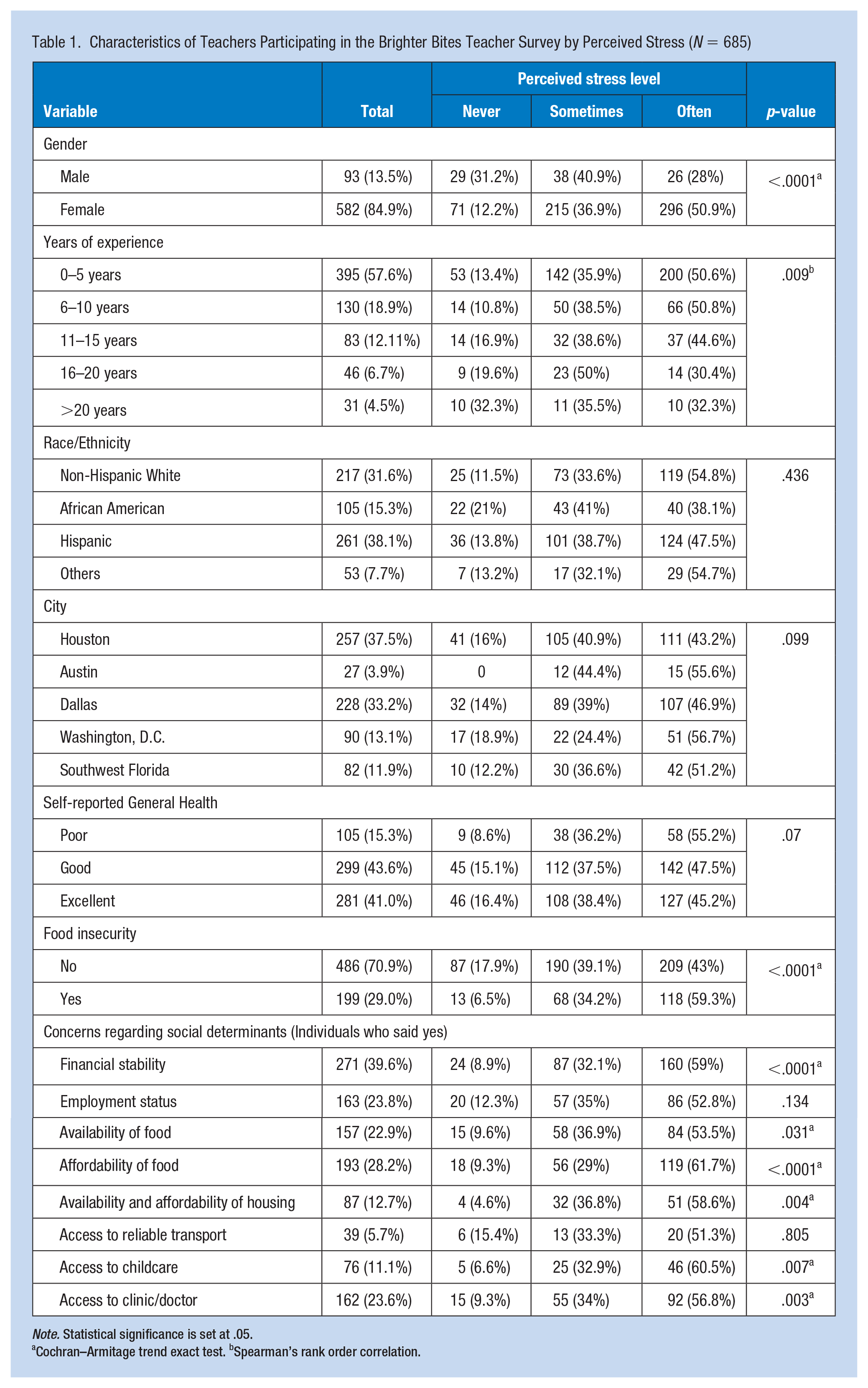
Note. Statistical significance is set at .05.
Cochran–Armitage trend exact test. bSpearman’s rank order correlation.
Table 2 summarized associations between perceived stress and social determinants of health assessed by GLMM. Results showed food insecure teachers had greater odds of reporting stress sometimes/often versus never as compared with food secure teachers (adjusted odds ratio [AOR]: 2.33, confidence interval [CI]: [1.63, 3.35], p = .0030). Similarly, teachers who were concerned about their financial stability (odds ratio [OR]: 2.68, confidence interval [CI]: [1.91, 3.75]), availability of food (AOR: 1.69, CI: [1.15, 2.48]), affordability of food (AOR: 2.27, CI: [1.59, 3.28]), availability and affordability of housing (AOR: 2.21, CI: [1.33, 3.67]), access to childcare (AOR: 1.76, CI: [1.06, 2.92]), and access to a clinic/doctor (AOR: 1.60, CI: [1.10, 2.33]) had greater odds of reporting stress sometimes/often versus never as compared with teachers who were not concerned about social needs.
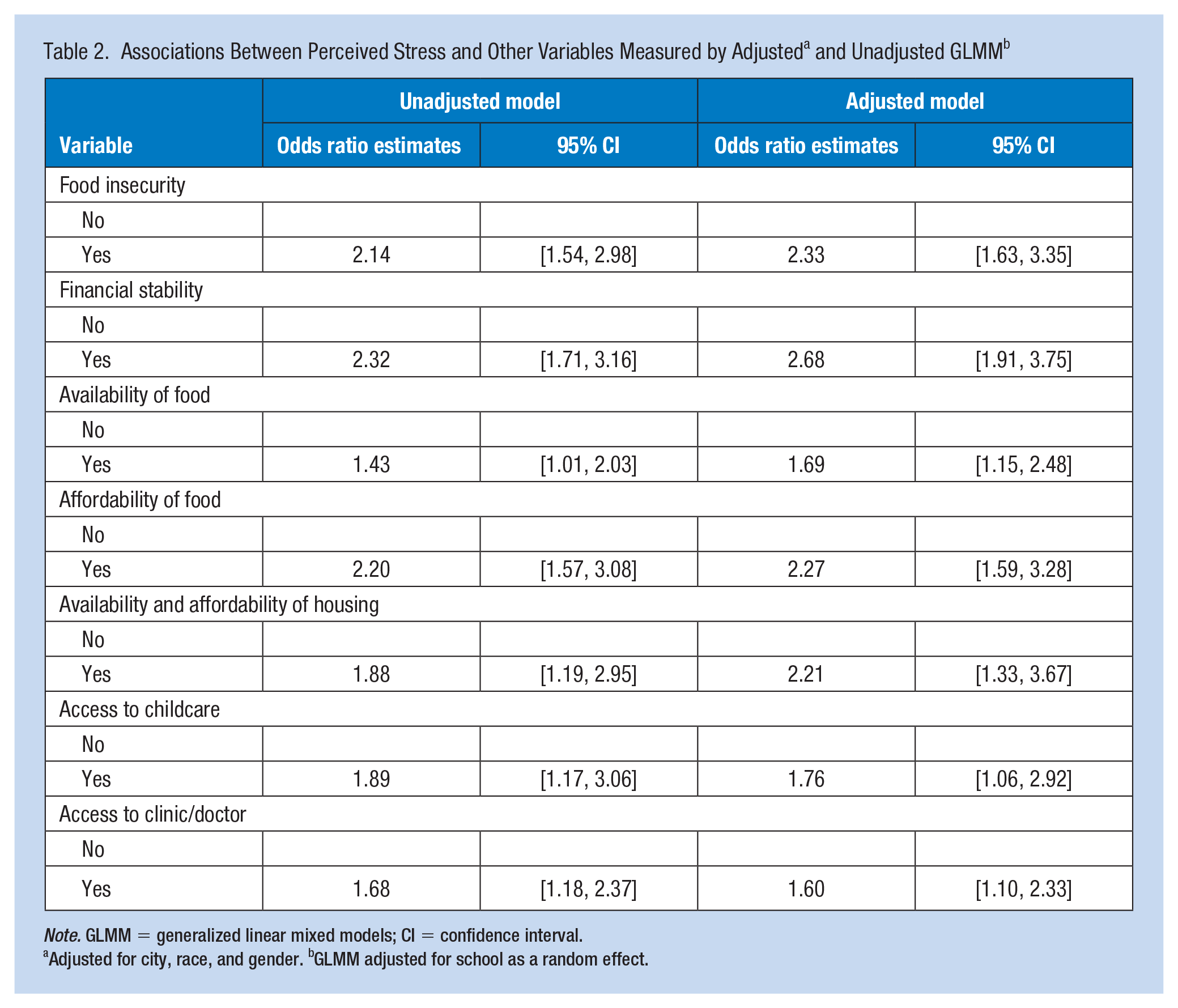
Note. GLMM = generalized linear mixed models; CI = confidence interval.
Adjusted for city, race, and gender. bGLMM adjusted for school as a random effect.
Discussion
This study adds to the limited body of literature on the mental health needs of elementary school teachers during the COVID-19 pandemic. Our study found a high prevalence of perceived stress among the responding teachers (response rate: 28.10%). These results agree with the survey conducted by the Yale Center for Emotional Intelligence in collaboration with Collaborative for Academic, Social, and Emotional Learning (CASEL) in March 2020. In this online survey, the most common feelings the pre-K-12 teachers working in the United States reported were anxious, fearful, sad, and overwhelmed due to both personal and professional pandemic-related reasons (Cipriano & Brackett, 2020; Yale Center for Emotional Intelligence, 2020). In addition, the prevalence of perceived stress in our study is higher than those presented in other similar studies (where prevalence varied from 12.6% to 50.6%) conducted during the pandemic (de Oliveira Silva et al., 2021). The higher perceived stress levels observed in our study could be because our study sample comprised teachers employed at schools serving low-income communities who may have been subject to strong financial pressures that ensued after the onset of the pandemic. Future studies could use a mixed-methods design to qualitatively assess the factors contributing to the stress among this teacher population during the pandemic.
Our results also demonstrated that food insecurity prevalence was high, with close to one third of the responding teachers stating they were experiencing food insecurity. Being food insecure was significantly associated with perceived stress. It is important to note that these food insecurity rates are higher than the national average (U.S. Department of Agriculture, 2015). A systematic review conducted prior to the pandemic to explore the relationship between food insecurity and emotional health (including stress, anxiety, depression, and anger) reported an association between food insecurity and negative emotional health (Bruening et al., 2017). Our study adds to the current literature indicating the importance of conducting further research to better understand the long-term impacts of the pandemic on teachers’ food insecurity and the need to implement evidence-based strategies to improve overall health in this population (Lauren et al., 2021; Thomas et al., 2019).
Our study also showed that concerns regarding financial stability, availability and affordability of food, availability and affordability of housing, and access to childcare and a clinic/doctor were high among the teachers, and these factors were significantly positively associated with perceived stress. It has been well established in the literature that individuals in teaching professions experience insufficient pay and budget cuts (Fay et al., 2020). This, coupled with the financial crisis and school closures and furloughs subsequent to the pandemic, may have resulted in acute concerns regarding financial stability, job stability, and other social determinants of health needs which, in turn, plausibly increased perceived stress (Fay et al., 2020; Wilhem et al., 2000). These findings concur with the study conducted by Diliberti et al. where the teachers reported insufficient pay and childcare as a primary reason for stress and teacher attrition during the pandemic (Diliberti et al., 2021). Given that the COVID-19 pandemic continues to persist in the United States, it is likely these impacts are going to be further exacerbated and warrant the need for immediate intervention strategies, including financial assistance and counseling to manage stress, to be made available to teachers.
The study’s results provide an insight into the prevalence and determinants of pandemic-related perceived stress among teachers. However, the study is subject to certain limitations. First, the participants of this study belonged to the schools enrolled with Brighter Bites from selected cities. Therefore, the results may not be generalizable to teachers across other metropolitan cities and suburban areas. Furthermore, the response rate was 28.1%. Thus, the low response rate may result in potential selection bias. Second, the self-reported questionnaires are subject to social desirability bias. In addition, perceived stress was subjectively measured in our study. In future studies, an objective measurement of this variable needs to be considered. Third, the cross-sectional nature of the data limits any temporality and causal associations which need to be considered in future studies.
Implications for Occupational Health Practice
Professionals in educational settings have been subjected to psychological discomfort and turbulence in work schedules since the onset of the COVID-19 pandemic (Hager et al., 2010). The current study demonstrates a higher prevalence of perceived stress among teachers who are largely female, with less experience, food insecure, and with high concerns regarding various social determinants of health. Given the persistence of the pandemic in the United States, the results of our study underscore the need for further investigation into the long-term impacts of the pandemic on teachers’ health and well-being, and to develop, implement, and evaluate intervention strategies to mitigate these issues. First, mixed-method studies can be conducted to understand specific job stressors of teachers from different backgrounds to build targeted interventions. Second, to address social determinants of health needs, as in our study sample, school districts could collaborate with nonprofit organizations and grocery retail companies to design innovative solutions such as voucher programs to address food insecurity and financial hardships during times of crises (Haider et al., 2021; Mukigi, 2018; Walker et al., 2021). Third, forming teacher coalitions with adequate administrative support can help the teachers in bolstering peer support by building strong social networks (Jones & Ali, 2021). This can also help in creating a positive school climate. Finally, it would be beneficial for school districts to implement evidence-based stress management programs coupled with social services to meet these teachers’ needs (Ansley et al., 2016; Harris et al., 2016; Walker et al., 2021).
Applying Research to Occupational Health Practice
The current study illustrates a high prevalence of perceived stress among school teachers during the initial phase of the COVID-19 pandemic and significant positive associations of the perceived stress with various concerns regarding social needs related to food, financial stability, and access to childcare and health care. It is paramount that school districts address the mental well-being and social needs of the teachers by providing a wraparound approach of stress management coupled with social services’ supports to meet their needs. Access to occupational health specialty services in addition to social services is warranted to ensure the root causes of the perceived stress are addressed.
Footnotes
Acknowledgements
The authors acknowledge the Michael & Susan Dell Center for Healthy Living, the Brighter Bites staff, and the participating schools and the teachers for their support on the project.
Author Contributions
N.P. contributed to conception, data analysis, interpretation, drafting, and revising the article. F.L. contributed to conception, data analysis, and interpretation. F.Z. contributed to data analysis and interpretation. R.-J.C. contributed to conception, interpretation, and critical revision of the article. M.M. contributed to interpretation and critical revision of the article. M.P. contributed to data acquisition and critical revision of the article. J.N. contributed to data acquisition and critical revision of the article. C.M.M. contributed to conception, drafting, and revising the article. S.V.S. contributed to conception, data acquisition, analysis, interpretation, and critical revision of the article.
Conflict of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Shreela Sharma serves on the board of directors of Brighter Bites 501c3 nonprofit organization. This is an unpaid board position. No other conflicts of interest exist.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the study was provided by Brighter Bites through Feeding Texas and the Texas Health and Human Services Commission. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethical Considerations and Disclosure(s)
This project was approved by the University of Texas Health Science Center, Committee for Protection of Human Subjects. Informed consent was obtained from the teachers prior to completing the survey.
Human Subjects Review Details
This project was approved by the University of Texas Health Science Center, Committee for Protection of Human Subjects Institutional Review Board (HSC-SPH-15-0752).
Author Biographies
Nivedhitha Parthasarathy, MPH - is a PhD student in Health Promotion and Behavioral Sciences at the University of Texas Health Science Center at Houston, School of Public Health. Her research interests include dietary behavior and obesity prevention among children and adolescents, and school health.
Fangyu Li, MS - is a PhD student in Epidemiology, Human Genetics and Environmental Sciences at the University of Texas Health Science Center at Houston, School of Public Health. She is also a predoctoral fellow with National Cancer Institute with a focus on Nutrition Epidemiology, gut health, and cancer.
Feng Zhang, MS - is a PhD student in the department of Biostatistics and Data Science at the University of Texas Health Science Center at Houston, School of Public Health. He is trained in statistics, machine learning, and epidemiology.
Ru-Jye Chuang, DrPH - is a faculty associate at the University of Texas Health Science Center at Houston, School of Public Health in the Department of Epidemiology, Human Genetics and Environmental Sciences. Her research interests include designing and implementing health promotion programs for obesity prevention and oral health,
Mallika Mathur, MPH - is a PhD student in Epidemiology, Human Genetics and Environmental Sciences department at the University of Texas Health Science Center at Houston, School of Public Health. She has a vested interest in maternal and child health.
Mike Pomeroy, MPH - vice president of operations of Brighter Bites, overseeing and directing programmatic aspects of Brighter Bites.
Jacqueline Noyola, BS - is the Brighter Bites program manager for nutrition education. She also works on Brighter Bites school action plans, accountability tools, and data collection metrics for the Coordinated Approach to Child Health (CATCH) and other child-focused school programs.
Christine M. Markham, PhD - is a professor and interim department chair of Health Promotion and Behavioral Sciences department at the University of Texas Health Science Center at Houston, School of Public Health. She works on the development and evaluation of child and adolescent health promotion interventions, including school-, clinic-, and family-based interventions.
Shreela V. Sharma, PhD, RDN - is a professor in the department of Epidemiology, Human Genetics and Environmental Sciences at the University of Texas Health Science Center at Houston, School of Public Health. She also serves on the board of directors of Brighter Bites nonprofit organization. She has worked on various nutrition and physical activity-based interventions to address obesity via school-, family-, and community-based approaches.