
Abstract
Introduction
To date, data about the morbidity, mortality, and risk factors for COVID-19 virus related to ethnicity and race are limited. The United States started collecting demographic data of persons affected by the disease late into the pandemic. Surveillance data on race and ethnicity are still emerging because over 300 thousand cases were reported without race and ethnicity data (Centers for Diseases Control [CDC], 2020). However, early data suggest that disadvantaged groups experience disproportionate negative outcomes from the virus (CDC, 2020).
In early April, data started appearing that identified race and ethnicity showing people of color were at high risk for COVID-19 (Goodman, 2020; Lahut, 2020; Robinson, 2020; Vickers et al., 2020). In one of the first reports from New York City, 34% of COVID-19 deaths were among Hispanics who represent 29% of the city population. Furthermore, 28% of COVID-19 deaths in New York City were among African Americans (AAs), 22% of the city population (Robinson, 2020).
In Detroit, Chicago, and New Orleans, over 70% of coronavirus-related deaths have been reported to be among AAs (Vickers et al., 2020). In Illinois, Latinos represent 17.4% of the total population and have the highest confirmed cases with 60% of Latinos testing positive. AAs represent 14.6% of the deaths total population and make up 34% of COVID-19 deaths (U.S. Census Bureau, 2018; Illinois Department of Public Health, 2020). In Wisconsin, AAs make up 28% of the population yet account for 73% of all COVID-19 deaths (Lahut, 2020). In Arizona, Native Americans from the Navajo communities make up 6% of the population but 16% of COVID-19 deaths (Goodman, 2020).
According to the CDC, social determinants of health (SDOH) are conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks (CDC, 2020). Zip code has shown to be been more predictive of health outcomes than a “genetic code.” The risks of SDOH are increased in persons from underserved and minority groups who have a higher number of risk factors like hypertension, diabetes, cancer, obesity, lung disease, and pulmonary diseases. Many of these groups have limited access to culturally congruent health care (Artiga, 2020).
The SDOH are known to drive health disparities; therefore, it is important to identify and understand both social and physical risk factors that determine health outcomes in all people (CDC, 2020; Wallace, 2019). During this pandemic, the SDOH are exacerbated as evidenced by the following (Sullivan & Connelly, 2020).
Housing instability is often seen as crowded, low-income housing where social distancing is difficult, thereby, quickly spreading in persons with SDOH risk factors.
Food insecurity may result in limited items like food essentials, infant formula, and disease specific nutrition. Farm workers who are often migrant workers or persons from low incomes also become at risk due to disruption of food supply seen in a pandemic.
Social isolation can result in loneliness and poor health habits like smoking, alcohol consumption, and drug use. Stay at home orders have been linked to an increase domestic violence and abuse.
Prejudice and discrimination has been experienced, specifically against Asian Americans who have reported harassment and physical assaults. The use of the term “Chinese Virus” puts all Asian Americans at risk for incivility resulting in mental health challenges and physical injury. Health system leaders must unequivocally denounce anti-Asian racism, dispel myths, and detail repercussions for any discriminatory treatment of patients or staff.
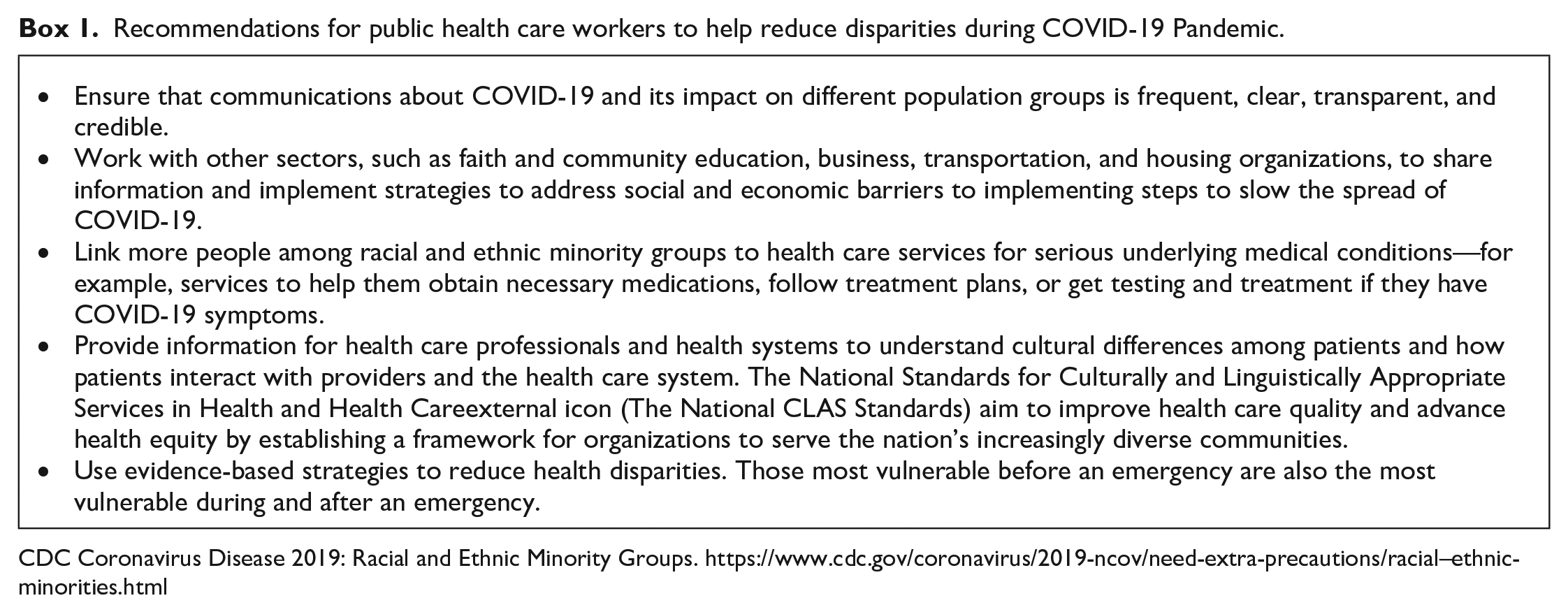
It is imperative that data are collected to determine the extent of the impact of COVID-19 in hard to access communities and develop a stronger understanding of related risk factors in the country. The CDC has provided recommendations for public health workers to help reduce disparities during COVID-19 Pandemic (Box 1). The purpose of this article is to provide an overview of the National Coalition of Ethnic Minority Nurse Associations (NCEMNA), present COVID-19 epidemiological data on five racial–ethnic groups and identify culturally congruent health care strategies for each group. Finally, directions for practice and research will be discussed.
Recommendations for public health care workers to help reduce disparities during COVID-19 Pandemic.
CDC Coronavirus Disease 2019: Racial and Ethnic Minority Groups. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/racial–ethnic-minorities.html
What Is the National Coalition of Ethnic Minority Nurse Associations?
During the May 1997 Third Invitational Minority Nursing Congress, the presidents of the Asian American Pacific/Islanders Nurses Association (AAPINA), National Association Hispanic Nurses (NAHN), National Alaska Native American Indian Nurses Association (NANAINA) and the National Black Nurse Association (NBNA) came together to discuss a collaborative organization to consider the issues, opportunities, and advantages of forming a unified entity. NCEMNA was officially incorporated in 1998 and the Philippine Nurses Association of America (PNAA) joined later in 1999.
The original focus of NCEMNA was to eliminate racial and ethnic disparities and increase the number of minority nurse researchers. NCEMNA leaders built on existing contacts they had with both private and public organizations and identified areas of mutual concern. NCEMNA became a unified force of five racial and ethnic professional organizations that advocate for equity and justice in nursing and health care to eliminate health disparities while also giving voice to 1,056,695 nurses (26.7% of the U.S. registered nurse (RN) population; Brief Summary Results from the 2018 National Sample Survey of Registered Nurses, 2019).
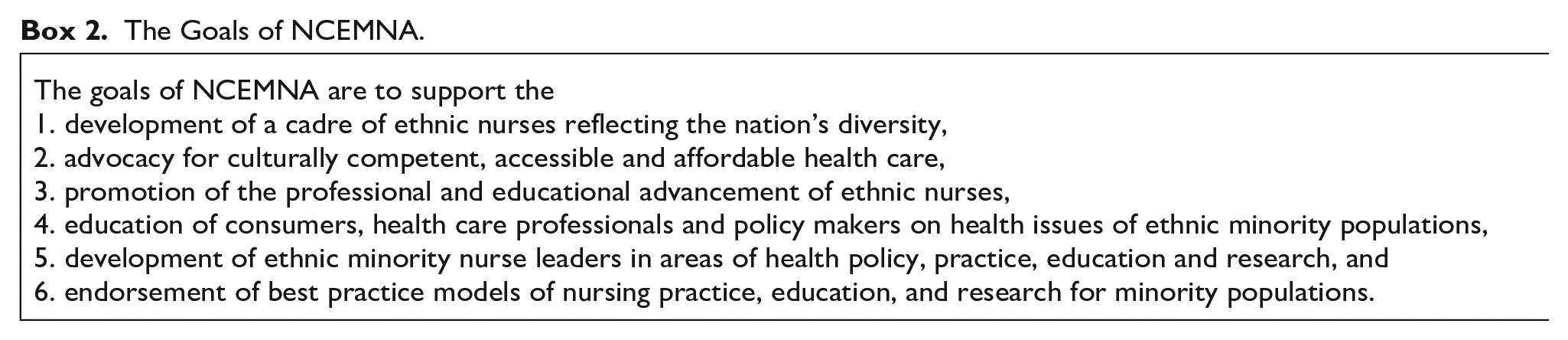
The mission of NCEMNA is to be the unified body advocating for equity and justice in health care with a vision to be a leading voice and driving force for ethnic minority populations. NCEMNA’s core values are equity, advocacy, relevance, and diversity. The goals of NCEMNA are shown in Box 2. The organizations of NCEMNA are united by a shared mission, vision, professional core values, and common goals (see Table 1). The NCEMNA Board of Directors and its officers maintain active efforts to promote ethnic minority nurse leadership in areas of health policy, practice, education and research, and to implement leadership development and mentorship programs. NCEMNA’s voice is essential in addressing racial and ethnic minority health issues and promoting the diversity of the nursing workforce.
The Goals of NCEMNA.
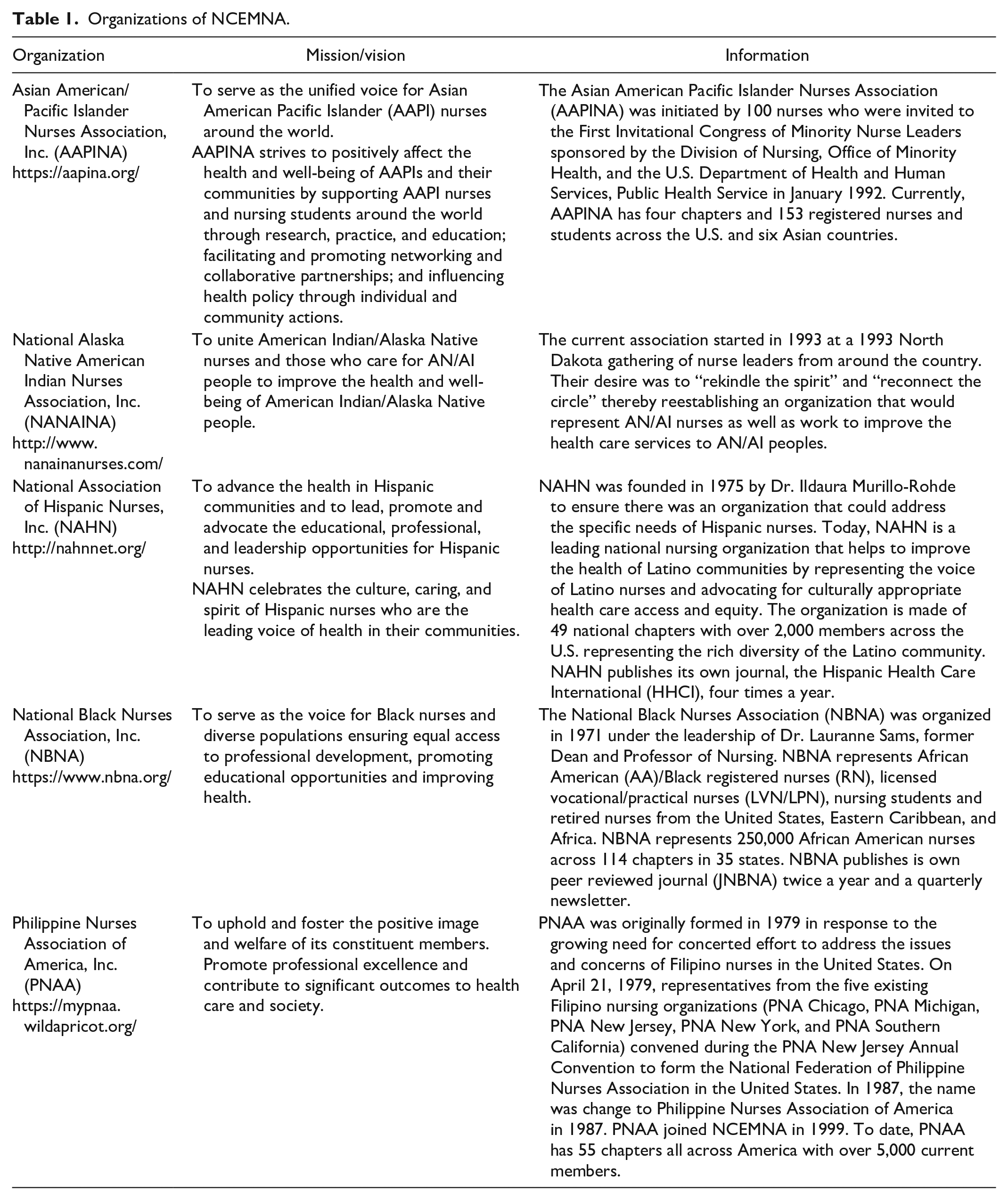
Organizations of NCEMNA.
Asian American Pacific Islander Nurses Association
The 2017 Census Bureau population estimated 18.2 million Asian Americans (5.6% of total population) and 1.6 million Native Hawaiian and Other Pacific Islanders (0.4% of total population) living in the United States (U.S. Census Bureau, 2019; U.S. Department of Health and Human Services, 2020). Most Asian Americans and Pacific Islanders reside in California followed by New York, Texas, New Jersey, and Illinois. In health care settings, Asian American nurses account for 5.2% of total RNs and Pacific Islander RNs account for 0.6% (U.S. Department of Health and Human Services, 2019).
COVID-19 in Asian American Pacific Islanders
Regarding coronavirus deaths, Asian Americans represent 6.5% overall COVID-19 deaths in the United States, which is higher than the overall American population (5.7%; CDC, 2020). Specifically, death rates of Asian Americans residing in California, New York, and Washington states are higher than those in other areas of the United States (CDC, 2020). Also, Pacific Islanders COVID-19 positive cases are 1.4% and death rates are 1.2%, which are higher than those of California population (California Department of Public Health, 2020). Higher death rates among Asian Americans and Pacific Islanders might be explained by (a) their high risk health behaviors such as smoking and alcohol drinking and a high prevalence of the respiratory diseases tuberculosis and chronic obstructive pulmonary disease; and (b) limited accessibility to health care providers due to low or no health insurance coverage and language barriers (U.S. Department of Health and Human Services, 2020).
Culturally Congruent Health Care for the Asian American Pacific Islanders
It is difficult to combine Asian/Pacific Islanders as one cultural group; there are over 70 subethnic groups within Asian Americans (Ito, 1997). Subsequently, it is also difficult to define culturally congruent health care for this group with high diversity in values, language, regions, and religions (Ito, 1997). For the convenience of discussion, we take an approach that generalizes Asian/Pacific Islanders as one group, which subsequently limits the generalizability of the discussion points that follow. General guidelines for providing culturally congruent care for Asian/Pacific Islanders during this pandemic include the following:
Health care providers need to be recognizant that this group has high respect for health care providers, especially older male physicians (Dibble, 2019; Purnell, 2014).
Health care providers need to be aware of unique cultural attitudes toward symptoms and pain. As frequently reported in the literature, this group tends to be stoic and rarely seeks help until symptoms and pain become intolerable, frequently resulting in suffering from symptoms and pain that could be easily relieved using existing regimens (Purnell, 2014).
Health care providers need to be aware that recent immigrants from Asian countries may come from a country with universal health insurance mandated by the government, but many of them may not have a health insurance in the United States (Purnell, 2014). Furthermore, language barriers, modesty, cultural attitudes toward the disease, and communication problems could cause impediments for access to health care (Dibble, 2019; Purnell, 2014).
Among Asian/Pacific Islanders, self-medication with herbal remedies is frequently practiced (Dibble, 2019; Purnell, 2014). For instance, among East Asians, ginseng (a root used for anything from a remedy for the common cold to an aphrodisiac) is frequently used. Chinese traditional herbs or other herbal medications are also used to control the degree of “wind” that may be in the body.
Most families consider that they must care for family members at home. Thus, involving family members in discharge education would be essential. Also, involving family members in education for preventive measures is essential to prevent the transmission of the disease.
National Alaska Native American Indian Nurses Association
There are 1.9 million American Indians and Alaska Natives (AIAN) or Native Americans according to the Bureau of Indian Affairs (2020), an agency of the Department of Interior. AIAN as a single race make up 1.3% of the U.S. population (U.S. Census Bureau, 2019). There are 574 federally recognized tribes (Bureau of Indian Affairs, 2020) and some state-recognized tribes. Tribes are considered sovereign nations, have a government-to-government status with states and the federal government; and lands or reservations are held in trust by the federal government. Up to 71% of AIAN live in urban areas (Urban Indian Health Institute, 2020); however, many are quite mobile as they move back and forth between reservations and urban communities for educational or employment purposes. As with other ethnic populations, there is diversity within the AIAN populations that vary by tribal status, language, geography, culture, and in other ways (National Congress of American Indians, 2018; 2020).
COVID-19 in American Indians and Alaska Natives
As of April 30, 2020, the Indian Health Service (IHS) estimated that the overall percentage of COVID-19 infections was 10%; however, due to the scarcity in testing, this is assumed to be an underestimate (IHS, 2020). On the same day, the Navajo Nation (2020) reported 1,977 or 24% positive results among those tested on their reservation. Tribes have received some federal assistance for COVID-19; however, many have expressed concerns in the delayed federal response. Several tribes including the Navajo Nation took legal action to request their fair share of federal funds for dire situations on their reservations (The New York Times, 2020). As sovereign nations, AIAN tribes have declared public health emergencies among their people as well as ordered stay-at-home mandates, curfews, limited mass gatherings, and fines if curfews are violated (Navajo Nation, 2020).
There are 12 Tribal Epidemiology Centers throughout the country which have been instrumental in data collection, reporting, and analyses. The most active has been the Navajo Epidemiology Center working in coordination with the Navajo Nation Department of Health, Navajo Health Command Operations Center, the Navajo Nation Office of the President and other tribal agencies (Navajo Nation, 2020). Communication with tribal members is extremely important due to lack of understanding of this new corona virus, unlike any other respiratory illness experienced in recent times. Health guidelines and educational material from the National Indian Health Board (NIHB), IHS, and CDC are available. NIHB serves as a national communication conduit between tribal nations and government agencies.
In the most remote regions of the U.S., communication about COVID-19 has been challenging in areas where people may not have electricity or poor connection to Wi-Fi hotspots or other means. For people without transportation, hitchhiking is the best means to access health care, making social distancing impossible. Where there is one vehicle, an extended family might crowd into one available car to seek care (Clahchischiligi, 2020; Kovich, 2020).
Culturally Congruent Health Care for the American Indians and Alaska Natives
AIAN nurses make up 0.3% of the total U.S. nursing workforce (HRSA, 2019). In working with tribal communities, nurses must be knowledgeable about tribal laws and guidelines in taking care of patients, including local emergency declarations, communication with patient and communities, and providing accurate and understandable messages.
Nurses working in these communities must be objective and understand that CDC guidelines of frequent hand washing and physical distancing may not be possible due to scarcity of indoor plumbing and multigenerational housing. Nurses must provide masks for family members to wear and assist with procuring hand sanitizer as needed, clearly explaining reasons for physical separation and no visitation policies in hospitals.
After being in contact with COVID-19 patients, people might return home for traditional smudging or cleansing supplies (sage, cedar, sweet grass, corn pollen, traditional tobacco) for their self-care needs. It is important to support patients in individual ceremonial use of smudging or cleansing. Traditional health care practices are a valued part of the communities.
All health care providers must be cognizant to assess total health needs for this population. Mental health screenings for depression, suicide ideation, child abuse, and domestic violence. These needs are already in abundance for the population and are increased during the pandemic.
The role of public health nurses in AIAN communities is vital in order to conduct the important traditional public health work of education and prevention, disease control including testing and contact tracing, effective communication about COVID-19 and policy development. Nurses, as trusted and most respected health care professionals, must advocate for vulnerable populations and point out inequities in the health care and public health systems and be actively engaged in policy development for these populations (Asiodu et al., 2020; Edmonds et al., 2020).
National Association of Hispanic Nurses
The Latino population is the largest racial–ethnic minority group living in the United States. There are approximately 59.8 million Latino individuals living in the United States, making up 18.3% of the total U.S. population (U.S. Census Bureau, 2018). Latino RNs currently represent 10.2% of the nearly 4 million licensed RNs in the United States (HRSA, 2019). The mismatch between the U.S. Latino population and Latino RN workforce means there are fewer health care providers who can provide culturally sensitive care to Spanish-speaking patients, fewer providers who understand the cultural nuances that influence health beliefs and practices, and fewer providers who can help advocate on behalf of Latino communities who are experiencing health disparities and health inequities.
COVID-19 in Latinos
Many factors influence the health outcomes of COVID-19 in Latinos including the prevalence of higher comorbidities, SDOH, and limited access to health care. Risk factors for COVID-19 (e.g., including hypertension, diabetes, and obesity) are prevalent in the Latino population and they are thereby at higher risk of complications and mortality (Richardson et al., 2020; U.S. Department of Health and Human Service, 2020).
As of April 21, 2020, the CDC reported the distribution of Hispanic/Latino COVID-19-related deaths in the United States was 16.7%. States with the largest COVID-19 related deaths include Arizona, Florida, and Texas (CDC, 2020). In most states, the weighted percentage of COVID-19 deaths among Latinos is larger than the states’ total Latino population.
Culturally Congruent Health Care for the Latino Population
Like other ethnic-minority groups, the Hispanic or Latino population is not homogeneous; it contains over 30 subgroups (U.S. Census Bureau, 2020). A few of the Latino subgroups include Mexicans, Puerto Ricans, Cubans, Salvadorians, Dominicans, Guatemalans, Columbians, Hondurans, Ecuadorians, and Peruvians. Health disparities exist among the subgroups. For example, Mexican Americans have higher rates of diabetes compared with other Latino subgroups (U.S. Department of Health and Human Service, 2020). Therefore, providing a culturally congruent approach to the Latino population must carefully consider the unique risk factors, health beliefs, and SDOH based on differences in subgroups.
It is important to identify how Latinos want to communicate, whether in Spanish or English. Researchers have found that racial/ethnic concordance influences communication, satisfaction, and decision making (Alegría et al., 2013). Therefore, providers with the same racial/ethnic background, who speak the same language as their client and understand specific cultural beliefs, can contribute better health outcomes among these persons.
Health promotion and disease prevention education and interventions must carefully consider Latino culture-specific health beliefs and the impact of SDOH. Awareness and assessment of traditional cultural beliefs of familism, personalism, religion, machismo, fatalism, folk illnesses, and remedies can help health care providers better understand how such factors affect the health beliefs of their client determine to provide best evidence-based care practices.
Stay-at-home orders may be difficult for Latinos because they are in jobs that are considered essential workers. Employers must offer the proper personal protective equipment (PPE) and protections needed to keep all essential workers safe and decrease exposure to COVID-19.
Bilingual COVID-19 education must include targeted public service announcements shared on radio, television, social media platforms, and advertisements where Latino communities can receive the most updated guidelines and recommendations. COVID-19 testing, treatment, and preventative care should be a free service to all. Latino communities need to be provided culturally sensitive information about COVID-19.
Immigration status may limit access to resources and increased experiences of health care discrimination (López-Cevallos & Harvey, 2016). Enforcement of immigration laws like the Public Charge punish noncitizens for receiving public federally funded benefit programs for health, food, and housing (U.S. Citizenship and Immigration Services, 2020).
National Black Nurses Association
According to the July 2017 census data, 41.4 million people in the United States identified as single-race AA/Black. At 12.7% of the total U.S. population, AAs are the second largest minority population. In 2018, the U.S. Census Bureau estimated the AA/Black population at 13.4%. Fifty-eight percent of AA/Blacks live in 10 states, many of which are epicenters for COVID-19: Texas, Georgia, Florida, New York, North Carolina, California, Illinois, New Jersey, Virginia, and Louisiana (U.S. Department of Health and Human Services, 2017. The AA/Black RN population makes up 7.8% of the 3.9 million RNs (Brief Summary Results from the 2018 National Sample Survey of Registered Nurses, 2019).
COVID-19 in AA/Blacks
On April 23, 2020, the CDC reported that 25.5% of deaths per 100,000 were AA/Black. Home zip code, where you work and play, income, financial resources, and education all matter in COVID-19 disease and morbidity just as much as having comorbidities. In the United States, there is a large percentage of AAs who are underinsured, uninsured, have poor access to health services and live with comorbidities that place them at a disadvantage when dealing with major health threats. Early COVID-19 surveillance data clearly reflect that race and ethnicity matter in the Black and Brown communities.
Culturally Congruent Health Care for AA/Blacks
Since its inception, the focus of the NBNA has been on improving the health of AAs/Blacks through the provision of culturally appropriate and competent health care services. The Association is proud of its Collaborative Community Health Model developed by Dr. Linda Burnes Bolton and Dr. C. Alicia Georges, NBNA past presidents. This model is the basis for collaborative partnerships and inclusive health programs that focus collectively on the entire community to improve health, achieve better outcomes, and use data to drive change.
The evidence supports that having caregivers, providers, researchers, educators, and leaders from within the population and communities being served is important. Harrison et al. (2019) reported that ethnic minority populations experience obstacles when engaging with health care systems. In addition, it is of the upmost importance to embed cultural competence strategies into health systems and services to ensure professionals have knowledge and skills to engage individuals from a culture standpoint. Over the past five decades health care, medical advances, and technology have improved yet health care disparities and social determinants continue to negatively influence health of persons of color, and access to care in AA communities (Thornton et. al., 2016). The United States and health care providers, systems, and payors must address the underlying social determinants that exist where people live, work, worship, play, learn, and obtain essential services such as food, water, housing and the air inhaled (Thornton et al., 2016; Wesson et al., 2019).
Philippine Nurses Association of America
The most recent American Community Survey data show that there are an estimated 4,037,564 (1.3% of U.S. population) Filipinos in the United States. This group makes up the second largest populations of Asian Americans after the Chinese. The five states with the largest Filipino population include the following: California, Hawaii, Texas, Washington, and Nevada (Asian Journal Press, 2018). It is estimated that around 4% (150,000) of practicing nurses in the United States are Filipinos (Quadra-Balibay, 2019).
COVID-19 in Filipinos in the United States
There is limited information on the overall prevalence of COVID-19 among Filipinos. Filipino enclaves exist in New York, New Jersey, Massachusetts, Illinois, and California. The Filipino Community Health Resources and Needs Assessment reported the top three health concerns among Filipinos as hypertension, diabetes, and cancer followed by respiratory problems such as asthma, all risk factors for severity of illness in COVID-19 (NYU Center for the Study of Asian American Health, 2016).
Many Filipinos are caregivers for their elderly parents. When living in dense cities like Queens, Manhattan, and Jersey City, Filipinos may be living in one- or two-bedroom apartments creating a challenge for those who have COVID-19 symptoms requiring quarantine. Living in close shelters with limited space puts other family members at higher risk for contracting the virus. There are anecdotal reports where micro aggressions related to COVID-19 and racial profiling are being experienced by Filipinos, especially among those who have Chinese descent.
Culturally Congruent Health Care for Filipinos
By nature, Filipinos are collectivist; the interest of the group often overrides the interest of the individual. This Filipino trait influences patterns of communication and connection with other members of the community. The Migration Policy Institute data in 2016 showed that 30% of Filipinos older than age 25 have limited English proficiency (Zong & Batalova, 2018). With an archipelago with over 7,107 islands and approximately 175 ethnolinguistic groups, Filipinos’ understanding about health is influenced by cultural and religious beliefs. Older adults would most likely ask for medical help from their family first and would prefer a provider that speaks their language. Some would use traditional or alternative treatment like herbs, tea, or oil for minor ailments.
The Philippine Consulate has reached out to local community-based organizations (CBO) in determining next-of-kin as some hospitals are not able to determine relatives of Filipino patients who passed away. Prior to COVID-19, the New York City Department of Health through the Mayor’s Office contacted Filipino CBO in order to leverage this network to aid in understanding concerns, improve services, and disseminate resources to the Filipino community.
Through this network, the City was able to leverage its communication when the outbreak started. CBO like Kalusugan Coalition received daily COVID-19 updates on basic prevention translated into the Tagalog language. Grassroots Filipino organizations together with the PNA-New York chapter partnered with the Philippine Consulate in New York City in providing a series of webinars that included a wide range of helpful topics on epidemiology, immigration and the employment impact of COVID, and addressed racism in the community.
Summary
The 2020 COVID-19 pandemic has clearly exposed the negative effects and outcomes of SDOH in the U.S. health system. Health care leaders, health systems, federal, state and local representatives must acknowledge that the U.S. health care system is failing racial–ethnic minority populations. Despite the fact that health care, medical advances, and technology have improved, the COVID-19 pandemic is heightening the awareness of health care disparities and the impact of SDOH on patient outcomes in the United States. To resolve health disparities in the United States, there must be a common focus on the systemic causes and cultural influences among racial–ethnic minorities. NCEMNA can serve as a vital partner to ensure culturally sensitive measures are taken to address the needs and reduce the risks of COVID-19 in communities of color. Addressing these issues could increase accessibility to health services and improve health outcomes during the COVID-19 pandemic and beyond.
Different approaches for providing health care services must be identified to effectively work with the culturally diverse population in the United States. Basic essentials must be present to promote health, including access to healthy food, clean water, housing, and clean air.
Data that measure cultural differences must be an embedded process to capture epidemiological data on race and ethnicity to develop culturally sensitive interventions and improve health outcomes. Organizations such as NCEMNA, with a cultural footprint that invests in diverse communities, has a deep understanding of cultural beliefs that affect health. NCEMNA directly serves and conducts research within diverse communities and can be a strong partner to decrease health inequities that persist.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.