
Abstract
Mothers’ delivery care satisfaction is one of the indicators used to monitor the quality of health care provision. However, there is paucity of evidence on level of maternal satisfaction and its determinants, in Ethiopia, particularly in Somali regional state. Determining the maternal delivery care satisfaction level and identifying its determinants is important to understand the gap and strengthen the existing strategies. Therefore, the study aimed to determine the level of maternal satisfaction and the associated factors among post-cesarean section delivery care at selected public hospitals in the Somali regional state of Ethiopia. An institutional-based cross-sectional study was conducted on 285 mothers who gave birth in selected public hospitals in the Somali region from June 15 to August 29, 2021. The study subjects were chosen from the hospital using simple random sampling, and data was collected by interviewing newly delivered mothers. The data was entered into EPI DATA version 3, exported and analyzed using the Statistical Package for the Social Sciences (SPSS) 26 statistical package. A multivariable logistic regression was applied to identify the factors related to maternal satisfaction at a 95% confidence interval. Variables with a P-value of less than .05 in the multivariable regression were considered to be significantly related to maternal satisfaction. The overall maternal satisfaction level with cesarean section delivery care service was 61.5% (95% CI: 56.1-66.3). Current planned pregnancy [AOR = 2.793; 95% CI: (1.42, 5.51)], antenatal care follows up [AOR = 2.008; 95% CI: (1.097, 3.67)], time spent obtaining health professionals [AOR = 4.045; 95% CI: (2.12, 7.71)], and gender of healthcare provider [AOR = 7.993; 95% CI: (4.11, 15.53)] were all associated with maternal satisfaction with cesarean. The overall maternal satisfaction level with cesarean section delivery care service was found to be low as per the national standards. Maternal satisfaction with cesarean section delivery care services was significantly associated with current pregnancy planned, antenatal care follow-up, time spent waiting for health professionals, and gender of healthcare provider. Thus, hospital administrators should focus on the cesarean section delivery service quality improvement area, and the care should be client-centered.
“What is already known on this subject?” and “What does this study adds?”
Based on recent studies, the rate of cesarean section delivery is increasing in Ethiopia. Wealth index, residence, fetal presentation, parity, occupation of mothers, and educational level of mothers are factors that increased rate of cesarean section delivery in Ethiopia. However, the quality of care, women’s experience, and satisfaction is less well known.
Many studies have been conducted in the context of the client satisfaction among vaginal mode of delivery care services in Ethiopia. In addition, these studies have been done in a particular geographical area and only looked into the percentage of clients satisfied but have not explored the contributing factors. Hence, there is need to summarize and provide a clear and complete evidence of the prevalence and client’s satisfaction and its determinants in cesarean section delivery service.
Introduction
One of the markers to track the quality of healthcare delivery is how satisfied mothers are with their treatment during childbirth. 1 Interpersonal etiquette, the standard of the care provided, ease of access or convenience, the cost of care, consistency, the physical surroundings, and availability are all factors that affect satisfaction.2-4
Clients are the ultimate users of a health facility. They expect comfort, care, and cure. They may, however, be pleased or dissatisfied with the service they received. 5 Their satisfaction is a complex concept that is related to a number of factors, including lifestyle, past experiences, future expectations, and the value of both the individual and society.6-8
A cesarean section (CS) is an operative procedure whereby the fetuses after the end of 28 weeks are delivered through an incision on the abdominal and uterine walls. 9 The safety of the operation has improved with time, largely due to improved surgical and anesthetic techniques. 10 World Health Organization (WHO) suggested that the rates of the cesarean section should not exceed 15% because has no additional benefit for the newborns or the mothers. On the other hand, a rate of less than 5% would reflect the difficulty in access to adequate treatment11 Despite, the WHO recommendation SSA still has the lowest rates of cesarean birth, with many countries having national CS rates below 5%. 12 There is an inequitable distribution of cesarean birth rate, even within the poor countries; with urban resident women having better access and more CS deliveries than their rural neighbors in Ethiopia. 13
The reasons for the rise in the rate of cesarean section birth include in part an increase in the facility-based delivery and access to health care. 14 The national prevalence of cesarean birth in Ethiopia is far below the WHO optimum range, 5% to 15%. 15 The national prevalence of cesarean section birth among very low-income countries like Ethiopia requires specific attention, considering that access to cesarean birth is still insufficient. However, cesarean birth seems to rise inappropriately in private facilities and some urban settings.16-19
However, there is paucity of evidence on level of maternal satisfaction and its determinants, in Ethiopia, particularly in Somali regional state. Determining the maternal delivery care satisfaction level and identifying its determinants is important to understand the gap and strengthen the existing strategies. 20 Therefore, the study aimed to determine the level of maternal satisfaction and the associated factors among post-cesarean section delivery care at selected public hospitals in the Somali region.
Research Questions
RQ1: What is the level of satisfaction of mothers delivered by cesarean section in Somali region?
RQ2: What are the factors that contribute to satisfaction of mothers delivered by cesarean section?
Methods
Study Area and Period
Somali Regional state is 1 of 10 regions of the Federal democratic Republic of Ethiopia. Situated in the eastern Ethiopian lowlands have boundaries with Djibouti, Somalia, and Kenya, locally bordering with Oromia, and Afar region. According to Ethiopian Central Statistics Agency the estimated region’s population at just above 4.5 million in 2007. 21 The region covers 271 970.91 km 2 -second in Ethiopia, 500 to 1600 m above sea level and the climate is warm, hot and arid. The region has 11 zones and 93 districts (Woreda) and 6 city administrations. A total of 11 zonal hospital, 206 health centers, and 3200 health post. The study was conducted from June 15 to August 29, 2021, in Public hospitals of Somali region. 21
Study Design
An institutional based cross-sectional study was conducted.
Study Population
All delivered mothers who underwent cesarean section in the selected public hospitals (Jigjiga Referral Hospital, Karamardha Hospital, Degahbour Hospital, and Kebridahar Hospital) of the Somali region were the study population.
Inclusion and Exclusion Criteria
All mothers who underwent CS in the selected hospitals were included in the study, and mothers who underwent CS but were seriously ill at the time of data collection were excluded.
Sample Size Determination
The sample size was calculated using the Stat-calc module of Epi-Info version 7.2 of a single population proportion formula with consideration of the following assumptions: prevalence (P) of 21% for satisfaction with CS delivery, 22 confidence level (CL) of 95%, margin of error (d) of 5%, and a non-response rate of 10%. Thus, the final sample size consisted of 285 mothers.
Sampling Method and Procedure
There are 11 zonal hospitals in the Somali region; 4 of them were selected by using a simple random sampling technique. Ultimately, proportional allocation followed by a simple random sampling technique was used to select study subjects from each hospital (Figure 1).

Diagrammatical presentation of sampling procedure on level of maternal Satisfaction with Cesarean Section and Associated Factors among delivered mothers in Somali Regional, Eastern Ethiopia, 2021.
Data Collection Tools and Procedures
The data was collected by interviewing the study participants. The questionnaire was adapted from previous research conducted on similar research topics. It was prepared in English, translated into the local language (Somali), and then back-translated into English to ensure accuracy. The questionnaire included socio-demographic information, post-CS satisfaction among delivered mothers, and factors associated with client satisfaction with cesarean section (obstetric factors, health care provider, and maternal delivery care service-related factors). Questions related to delivery service satisfaction comprised 10 items with 5 scales Likert type (1—Very Dissatisfied, 2—Dissatisfied, 3—Neutral, 4—Satisfied, and 5—Very Satisfied). Data collectors and supervisors were recruited and trained on data collection tools, consent, and ethical issues during data collection.
Data Processing and Analysis
The collected data was checked for its completeness and consistency manually. Data was sorted, coded, and entered into a computer using Epi-data version 3.2, then it was exported to SPSS version 21 software for analysis. Data was cleaned by simple frequency before analysis. The mean with standard deviation, continuous variables, and frequencies with percentage for categorical variables were used to describe the study subject’s characteristics.
Multicollinearity was checked by using variance inflation factor (VIF < 10) indicating the non-existence of multicollinearity. A logistic regression model was used to identify the association between explanatory and outcome variables. An odds ratio (OR) with a 95% CI was used to measure the strength of association between explanatory variables and the outcome variable.
The model fitness was checked using Hosmer and Lemeshow goodness of fit (P > 0.05). A P-value less than .25 on bivariable analysis was considered for variables to be candidates for multivariable logistic regression analysis. Variables with a P-value of less than .05 at multivariable logistic regression analysis were considered as statistically significant predictors of mothers’ satisfaction.
Operational Definitions
Satisfied—We took the Likert scale to measure the satisfaction status of mothers on delivery care services. Each satisfaction assessing question rated from 1 up to 5. Then, we sum up these 10 variables altogether. Then, we computed the 75th percentile for the 10 variables. Finally, those mothers who scored the value of 75th percentile or more of the satisfaction assessing questions were considered as “satisfied” of the delivery care services. However, mothers who scored less than the value of 75th percentile were considered as “dissatisfied” on the delivery care service. 20
Waiting time—The time between arrivals and the time seen by the health professional.
Labor and delivery period—The end of pregnancy by one or more babies leaving a woman’s uterus by CS.
Cesarean delivery or cesarean birth: An operation for delivering a baby by cutting through the mother’s abdomen and uterus.
Nulliparous: parturient without previous delivery.
Multiparous: parturient with previous 2 or more deliveries.
Grand multiparous: Parturient with 5 or more deliveries.
Results
Characteristics of Study Subject’s
Two hundred eighty-five mothers were included in this study, resulting in a 98.3% response rate. Of those, 171 (60%) of the mothers were aged between 20 and 30 years. The overall mean age of the respondents was 26.4 (± 6.1) years. Nearly three-fourths (81.1%) of the participants were urban dwellers. 240 (84.2%) respondents were from the Somali ethnic group, and about 248 (87.0%) were Muslim followers. The majority, 254 (89.4%), were married, and more than half, 172 (60.4%), were house wives. Almost half (49.8%) of the respondents were unable to read and write as shown in (Table 1).
Socio-demographic Characteristics of Mothers Delivering in Selected Public Hospitals of Somali Region, Eastern Ethiopia, 2021 (n = 285).

Note. SD = standard deviation.
Obstetric and Gynecological Characteristics of the Study Participants
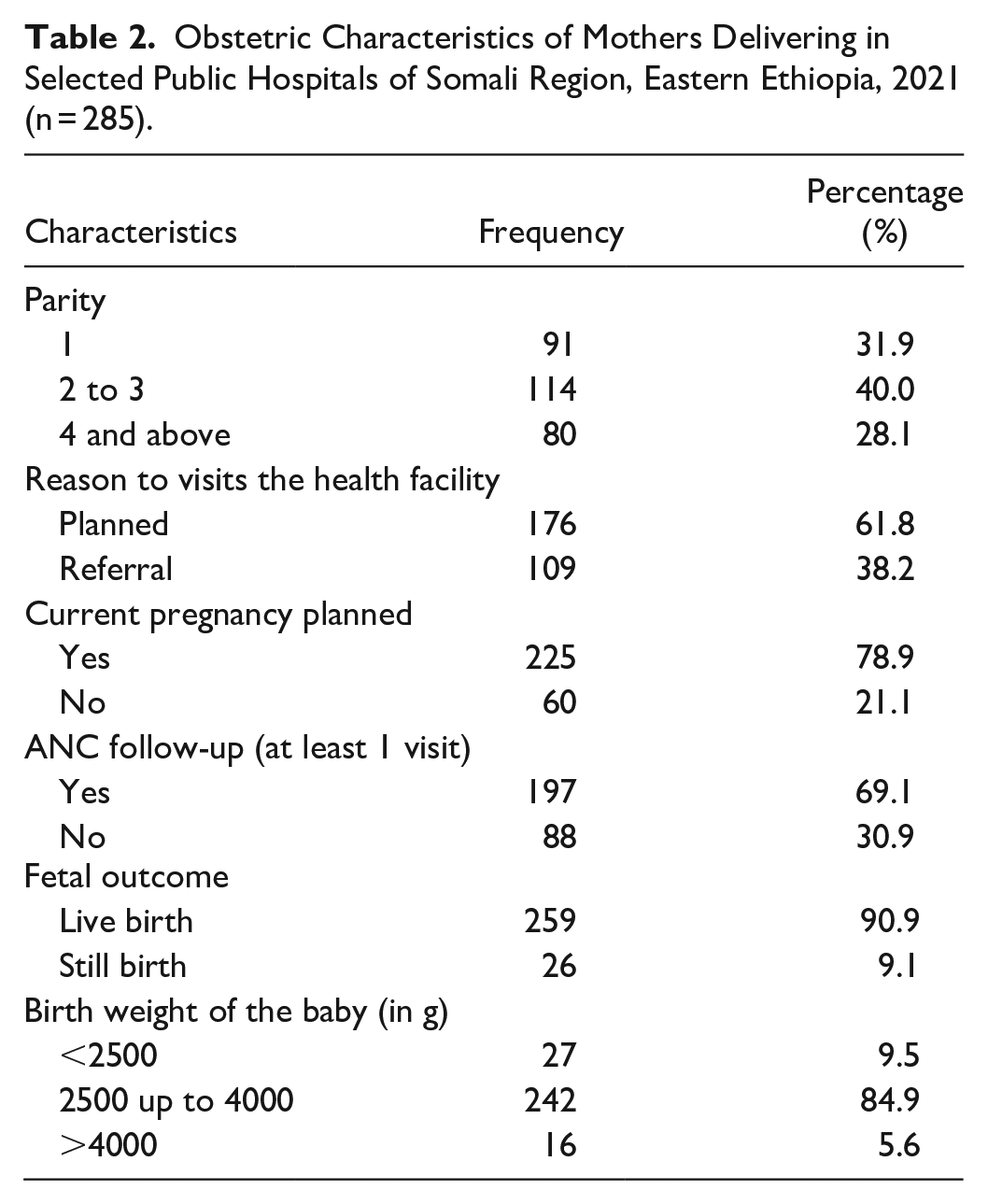
As indicated in Table 2, 114 (40.0%) of mothers gave birth to 2 to 3 deliveries. The majority of the women 225 (78.9%) had planned pregnancy. The majority of mothers 197 (69.1%) had at least 1 ANC visit. However, 26 (9.1%) of the respondents had still births. While 27 (9.5%) of mothers gave birth to babies weighing less than 2500 g.
Obstetric Characteristics of Mothers Delivering in Selected Public Hospitals of Somali Region, Eastern Ethiopia, 2021 (n = 285).
Health-Facility, Health Care Provider, and Maternal Delivery Care Service-Related Characteristics
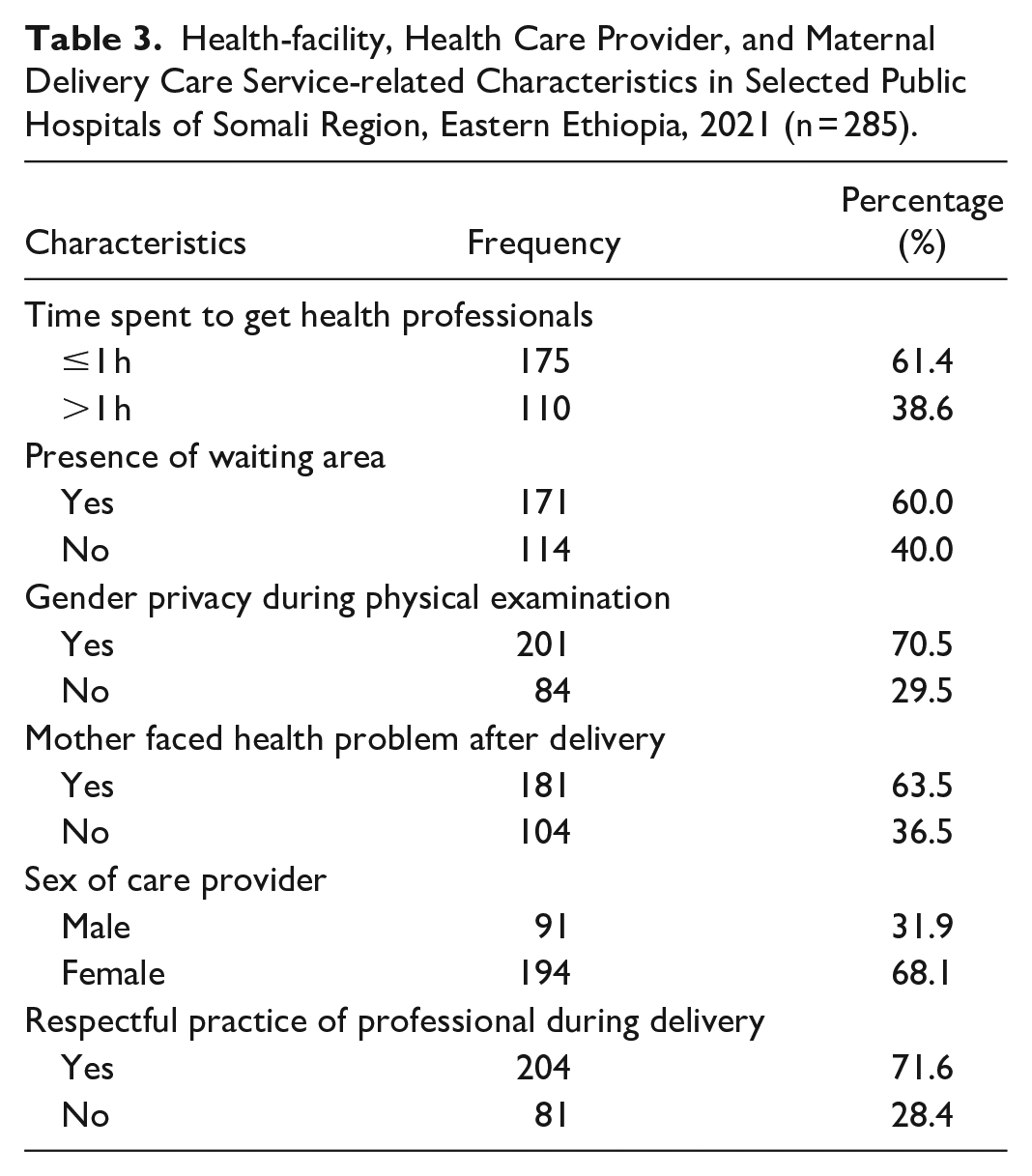
As indicated in Table 3, there was a delay in getting health professionals for service. About 110 (38.6%) of the delivered mothers spent more than an hour getting to the health care worker. Nearly three-fourths (70.5%) of delivering mothers had been examined with their privacy kept. More than half 183 (63.5%) of delivering mothers faced a health problem after delivery. The majority, 194 (68.1%) of the healthcare providers were female.
Health-facility, Health Care Provider, and Maternal Delivery Care Service-related Characteristics in Selected Public Hospitals of Somali Region, Eastern Ethiopia, 2021 (n = 285).
Maternal Satisfaction Level of Cesarean Section Delivery Care Services
Of the total of 285 clients, the majority (71.9%) of them were satisfied by the advice and counseling after delivered, and 70.5% were satisfied by the privacy maintained by health staff. In addition, 64.6%, 68.8%, 66.0%, 66.3%, 60.0%, and 58.2% were satisfied regarding waiting time to see a health worker, encouragement and support at delivery by health staff, courtesy and respect, availability of medical facilities in the ward, overall cleanliness of the facility, and waiting area cleanliness, and comfort, respectively. 50.2% of respondents were dissatisfied with toilet access and cleanliness, and 60.4% were dissatisfied with the availability of beds in the ward (Table 4).
Maternal Response on Satisfaction Level of Cesarean Section Delivery Care Services in Selected Public Hospitals of Somali Region, Eastern Ethiopia, 2021 (n = 285).

Factors Associated With Maternal Satisfaction With Cesarean Section Delivery Care Services
In crude analysis, current pregnancy planned, ANC follow-up (at least 1 visit), sex of care provider, residence, reason for visiting the health facility, time spent waiting to get health professionals, age of mothers, and educational level of mothers were significantly associated with maternal satisfaction with cesarean section delivery care services at P < .25.
In a multivariable logistic regression model, at a P-value of .05, current pregnancy planned, antenatal care follow-up, time spent getting health professionals, and gender of healthcare provider were significantly and positively associated with maternal satisfaction. When comparing mothers who planned (wanted) their current pregnancy to those who unplanned (unwanted), the odds ratio of cesarean section delivery service satisfaction was 2.79 times higher [AOR = 2.793; 95% CI: (1.42, 5.51)].
Among those mothers who attended antenatal care, the odds ratio of cesarean section delivery service satisfaction was 2 times higher [AOR = 2.008; 95% CI: (1.097, 3.67)] when compared to those mothers who did not attend antenatal care. Those mothers who waited 1 hour or less to be seen by the healthcare provider, the odds ratio of cesarean section delivery service satisfaction was 4 times higher [AOR = 4.045; 95% CI: (2.12, 7.71)] compared to mothers who waited more than 1 hour. The sex of the health care provider strongly affected the level of mothers’ satisfaction during delivery care services. Those mothers who got delivery care services by a female physician had an odds ratio of 7.99 times higher [AOR = 7.993; 95% CI: (4.11, 15.53)] than mothers who got the service by male physicians (Table 5).
Bivariable and Multivariable Logistic Regression of Factors Associated With Maternal Satisfaction With Cesarean Section Delivery Care Services in Selected Public Hospitals of Somali Region, Eastern Ethiopia, 2021 (n = 285).

Note. COR = Crude odds Ratio; AOR = adjusted odds ratio; CI = 95% Confidence interval; N = number.
Significant at *P < .05. **P < .01.***P < .001.
Discussion
This study determined the level of maternal satisfaction with cesarean section delivery care services and identified the associated factors at the health institutions. In this study, the overall maternal satisfaction with cesarean section delivery care service was found to be 61.5%. Maternal satisfaction with cesarean section delivery care services was significantly associated with current pregnancy planned, antenatal care follow-up, time spent getting health professionals, and gender of healthcare provider.
Sixty-five percent of mothers reported being overall satisfied with the care they received during their cesarean deliveries. This result agrees with research carried out in Bahir Dar, Ethiopia, which was 61.4%, 20 and also with findings from Wolaita Sodo University Teaching and Referral Hospital, which was 67.3%, 23 a study carried out in the Jimma regions, which was 65.2%, 24 and a study carried out in referral hospitals in the Amhara Region, which was 61.9%. 25
This finding is higher than the studies conducted in Siri Lanka (30.4%), 26 Adea Berga district found in West Shewa Zone, Oromia regional, Ethiopia (36.6%), 27 and Addis Ababa, Ethiopia (19%). 28 The possible reasons for this discrepancy might be women’s perception towards satisfaction, the management approach of the health managers of the health institutions, or the staffing of the health institutions.
Additionally, this result is lower than those of studies conducted in the Northwest Ethiopian towns of Debre Markos (81.7%), 29 Gamo-Gofa (79.1%), 30 and Nekemte Specialized Hospital (82%). 31 This discrepancy might be the result of a genuine differential in the quality of services rendered, mothers’ expectations, or the kind of healthcare facilities. Additionally, it could be brought on by differences in respondents’ literacy levels, cultural variety, the criteria used to gauge happiness, and the methods used to calculate total mother satisfaction.
In addition to determining the magnitude of maternal delivery care service satisfaction, the current study also identified various maternal delivery care service satisfaction predictors. Wanted current status of pregnancy was found to be a significant predictor of satisfaction. Mothers who wanted their pregnancy to be almost 3 times more satisfied with the cesarean section delivery care service than those who did not. This may be due to perceived confidence in socioeconomic and cultural readiness towards welcoming the expected baby. On the other hand, having a planned pregnancy may be associated with better knowledge and awareness of health services as well as familiarity with health facilities before delivery. This finding is consistent with findings from Ethiopia.23, 32, 33
According to the study finding, mothers who received ANC follow-up had a twofold higher likelihood of being satisfied with their cesarean birth services than mothers who didn’t. This concurs with research done in Ethiopia.20,23 This could be the result of mothers’ receiving more information on the value of a successful birth throughout the follow-up phase.
In comparison to mothers who waited more than an hour to be seen by a healthcare professional, those who waited an hour or less were 4 times more likely to be happy with the services they received during their cesarean birth. This is consistent with research conducted in western Ethiopia’s Nekemte. 31 This may be related to the fact that brief wait periods led to high levels of pleasure and little exposure to the uncomfortability and unkemptness of the waiting area.
The gender of the delivery care provider was the other important factor in determining satisfaction with maternal delivery care services. According to the study, mothers who received care for a cesarean section from a female healthcare professional were eight times more satisfied with that service than mothers who received care from a male healthcare provider. Studies done in Ethiopia confirm this finding.20,34 This could be the case because female delivery care providers may support deliveries in the mother’s best interests and may respect her cultural norms, giving her a great chance to feel more content.
Strength and Limitation of the Study
The magnitude of maternal satisfaction with cesarean birth care services and potential contributing variables have both been greatly enhanced by this study. However, because research participants can find it challenging to express their unhappiness in front of data collectors, social desirability bias may have had an impact on the quality of the data obtained. Additionally, the lack of a common quantitative cut-point for satisfaction with mother-delivery care presented another difficulty.
Conclusions and Recommendations
The overall maternal satisfaction level with cesarean section delivery care service was found to be low as per the national standards. Maternal satisfaction with cesarean section delivery care services was significantly associated with current pregnancy planned, antenatal care follow-up, time spent waiting for health professionals, and gender of healthcare provider. By enabling more predictable planning for ANC and more time to complete obligations outside of ANC, a scheduling intervention that decreases waiting time enhances the client satisfaction.
Footnotes
Acknowledgements
The authors are pleased to acknowledge the study participants who participated in this work and Jigjiga University and its staff for their support throughout this study by providing all necessary materials and technical support.
Author Contributions
KKA conceived the idea, collected the data, and played a major role in this research. The authors (KKA, AW, and GD) contributed to data analysis, writing, and editing the document. KKA, AW, and GD gave valuable ideas for the manuscript and revised it. Finally, all the authors (KKA, AW, and GD) read and approved the final version to be published and agreed on all aspects of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Jigjiga University.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the School of Graduate Studies, College of Medicine and Health Science, Jigjiga University Research and Ethical Committee (REC). An official letter was written from the school of Graduate Studies to hospitals (Jigjiga Referral Hospital, Kara Mara General Hospital, Degahbour Hospital, and Kebridahar Hospital) to get permission, and written consent was sought from every participant. The purpose of the study was explained to the study participants, and written consent was taken from participants to confirm whether they were willing to participate. Confidentiality of responses were also be ensured throughout the research process.
Data Availability
Almost all data are included in this study. However, additional data will be available from the corresponding author upon reasonable request.