
Abstract
The appearance of severe vulvovaginal varicosities (VVs) is challenging in pregnancy. The management of VVs may require a multidisciplinary approach, including radiologists, vascular surgeons, and obstetricians. We report a rare case of enormous VVs and pubic varicosities and summarize similar cases in the literature. A woman in her 20s with a full-term pregnancy visited our hospital for severe VVs and pubic varicosities. She had been in a spoke maternity unit where a cesarean section was scheduled. After a multidisciplinary evaluation, we offered her the chance to have a vaginal delivery (VD). The woman had an uneventful VD, and VVs disappeared after 40 days. A comprehensive literature search on this topic showed 11 cases of VVs during pregnancy (five VDs and six cesarean sections). The presence of VVs represented the indication for surgery in 70% of cases. Severe complications occurred in 20% of VDs vs. 50% of CSs. In pregnant women with VVs, the risk-benefit ratio suggests a chance of having VD.
Introduction
The vulva surrounds the vagina and external urethral meatus, including the labia minora, labia majora, clitoris, vestibule, and mons pubis. The pelvis contains numerous venous plexuses and anastomoses between the veins of the pelvis and legs, thus offering many opportunities to develop varices. During pregnancy, the rate of vulvar varicosities (VVs) increases. VVs occur in 8% of pregnancies. 1 There are anatomical (venous compression by the pregnant uterus) and hormonal changes that favor the formation of VVs during pregnancy. Ovarian and internal iliac veins with incompetent or absent valves can cause pelvic venous insufficiency. 1 Downstream VVs may develop owing to blood pooling in the pelvis. 1
The signs and symptoms of VVs usually depend on the severity of the clinical conditions. The symptoms range from mild local discomfort to difficulty in walking. The slight appearance of VVs is not an absolute contraindication to vaginal birth. VVs usually disappear within approximately 30 to 40 days after delivery. 2
The occurrence of severe VVs is a rare event in pregnant women. In these cases, the decision-making process is more demanding regarding the timing and the mode of delivery. The fear of vulvovaginal lacerations with possible severe bleeding makes management more uncertain. Several cases in the literature showed cesarean section (CS) as the delivery mode of choice in these extreme clinical conditions.2–7
A further crucial variable in VVs is represented by the setting where the birth occurs. CS rates are frequently higher in spoke maternity units than in hub hospitals because of unsuitable settings for prompt action with severe obstetric complications. 8 To date, there is no clear evidence on the best mode of delivery for these women. This report describes a rare case of huge VVs and pubic varicosities where the patient was able to have a vaginal delivery (VD). We also summarize similar cases in the literature.
Case report
Case presentation
The reporting of this study conforms to the CARE guidelines. 9 A 23-year-old woman with a full-term pregnancy visited our hospital for severe VVs and pubic varicosities, and she had difficulty in walking. She had been in a spoke maternity unit where a CS was scheduled.
The woman noticed an enlargement of the varicosities in the previous 2 weeks with worsening local discomfort and severe asthenia. Up to that point, her pregnancy had been uneventful. She had already had a vaginal birth without the appearance of VVs in her previous pregnancy. Her personal and obstetric history was unremarkable. She was not taking any medicine. All laboratory findings of blood and urine were within normal limits.
The patient’s external genitalia showed impressive pubic and VVs (Figure 1). On palpation, the varicosities appeared soft and slightly painful. The vaginal introitus was edematous and congested. We decided to perform an ultrasound with a color Doppler evaluation. An examination of the venous drainage of VVs showed bilateral reflux on the great saphenous vein. We were unable to evaluate possible drainage on the obturator circle. The superficial and deep femoral circle was bilaterally patent. These findings suggested pubic varicosities and VVs with probable drainage in the pelvic circulation. No thrombotic complications were observed.

Huge vulvar (white arrow) and pubic (red arrows) varicosities in a full-term pregnant woman.
After a multidisciplinary evaluation with vascular surgeons and radiologists, we offered the patient the opportunity to have VD. The patient's consent for treatment was obtained. Following the induction of labor with a cervical ripening balloon, the woman had an uneventful vaginal birth. The appearance of VVs and pubic varicosities changed during labor and after VD (Figure 2). These varicosities began to regress during the second stage of labor and then disappeared after 40 days. After 3 days, the patient had a regular postpartum course and was discharged with her healthy newborn.

Vulvar and pubic appearance during (a) the second stage of labor, (b) immediately after delivery, (c) at the time of discharge (3 days after delivery), and (d) 40 days after delivery.
Literature search and methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed to review the literature systematically. 10 A literature search was performed in the PubMed and Scopus databases (1946–2021) (accessed on 12 December 2021) (Figure 3). Retrospective observational studies (case reports, case series) including a full case description and reporting the following items were included: age, gestational weeks, signs/symptoms, lesion location, previous delivery, mode of delivery, indications for CS, and delivery outcome. Review articles and cases in a non-English language were excluded. In the search strategy, we searched for “vulvar, vaginal, vulvovaginal varicosities/varices/veins”, AND “delivery”, AND “vaginal delivery”, AND “cesarean section”, AND “pregnancy”, AND “bleeding”, AND “hemorrhage”. The only filter used was the English language. Relevant articles were obtained in full-text format and screened for additional references.
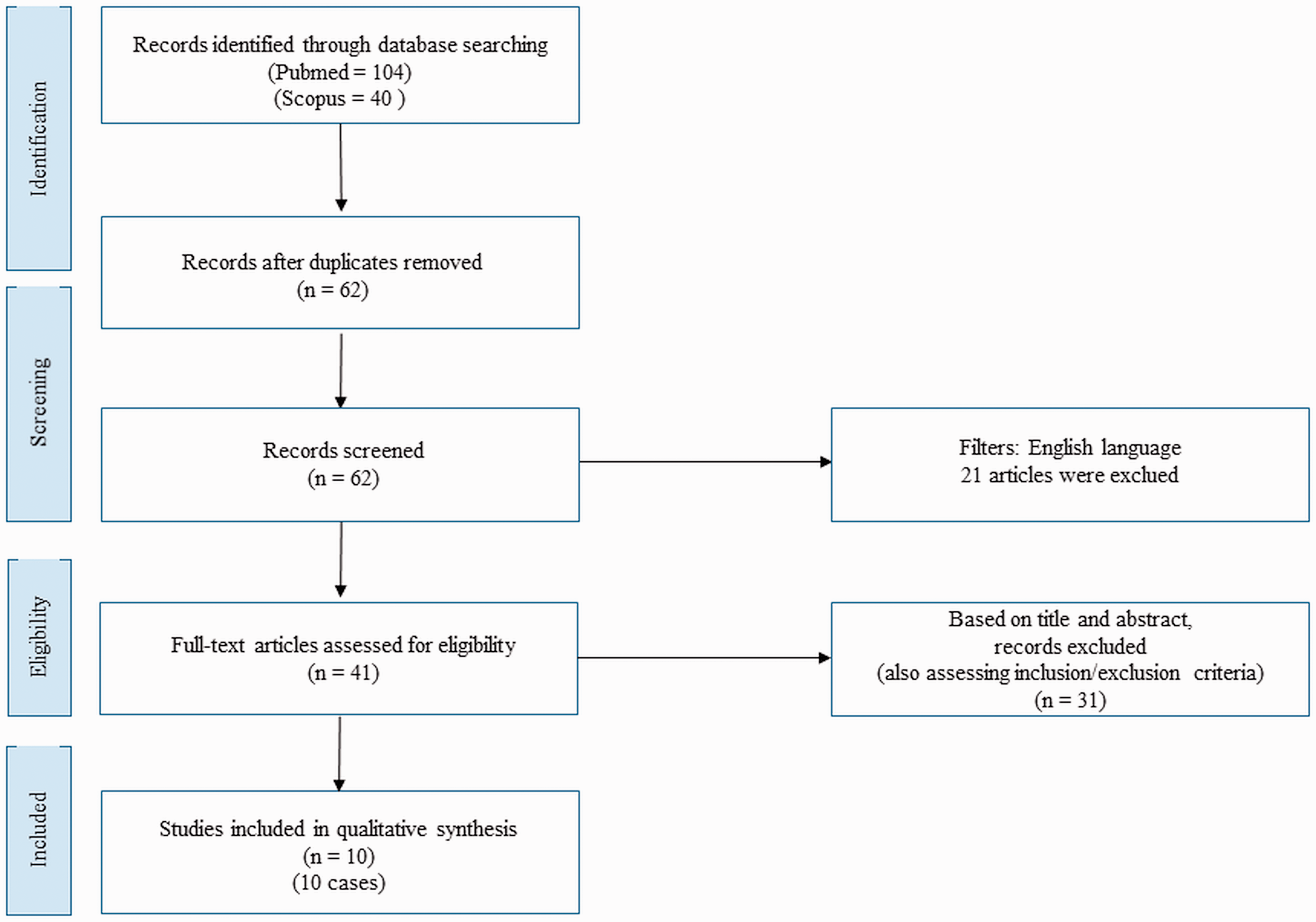
Flow chart of the literature review.
Two independent reviewers (L.G. and M.M.) selected the studies using a two-step screening method. At first, the screening of titles and abstracts was performed to assess eligibility and inclusion criteria and exclude irrelevant studies. The two reviewers then evaluated full texts of included articles to (1) assess study eligibility and inclusion criteria and to (2) avoid duplications of the included cases. Two other authors (J.D.G. and G.D.C) performed a manual search of reference lists to search for additional relevant publications. A.C. checked the extracted data. The objective of this systematic review was to provide and summarize the literature regarding a rare event for which there are limited data, such as the mode of delivery and outcome, in pregnant women with VVs.
The data collection was study-related (authors and year of study publication) and case-related (age, gestational weeks at delivery, signs/symptoms, varicosity location, previous delivery, mode of delivery, indication for cesarean section, and outcome). The collected data are reported as continuous or categorical variables. Continuous variables were tested for a normal or non-normal distribution using the Kolmogorov–Smirnov test. According to the distribution, the data are expressed as mean ± standard deviation or median and interquartile range. Categorical variables are expressed as the frequency and percentage. MedCalc® Statistical Software version 20 (MedCalc Software Ltd., Ostend, Belgium; https://www.medcalc.org; 2021) was used for the analysis.
Discussion
We report a successful VD in a woman with enormous VVs and pubic varices. Such huge VVs are a rare occurrence in pregnancy. Our patient had recently been in a spoke maternity unit where a CS had already been scheduled.
In primary maternity units, the resources readily available for obstetric emergencies are more limited compared with those in hub hospitals. 8 In this case, the fear of facing severe bleeding in an unsuitable setting may have led to choosing to have a CS performed. Our hospital is the only regional obstetric hub hospital. Our hospital manages all high-risk pregnancies (preterm fetuses, severe pregnancy pathologies), while low-risk and full-term pregnant women can also give birth in primary maternity units (spoke centers).
We carried out a multidisciplinary consultation to decide on the mode of delivery. We offered the patient the chance to have VD because of the absence of mandatory indications for surgery and a suitable setting for dealing with any complications. This situation emphasizes that, in a hub and spoke obstetric network, these women should be referred to a high-volume obstetric unit to avoid unnecessary CS.
The literature on VVs is limited. Few cases of VVs with severe varicosity have been reported. Furthermore, there are no indications for obstetric management of this condition. Therefore, more in-depth research on this topic needs to be performed to provide more detailed information for daily obstetric practice. To date, a summary including all cases of VVs in pregnancy reported in the literature is missing. In our literature review, 11 cases of VVs in pregnancy were identified at the final analysis, including the present case (Table 1).2–7,11–14 The median age was 29 years. All of the women were pregnant at full term. Almost all patients reported a vulvar and/or vaginal localization. Our case is the only one that showed a pubic location. The signs and symptoms appeared nonspecific. Most women reported mild local vulvar discomfort. Approximately 55% of the women were nulliparous. Interestingly, three women had Klippel–Trenaunay syndrome. Klippel–Trenaunay syndrome is a rare malformation that includes the presence of capillary malformation, hypertrophy of soft tissues and bones, and atypical lateral varicosity. Pregnancy in these women can exacerbate the signs/symptoms of the disease. Five (45%) women had a vaginal birth, while six (65%) underwent a CS. Approximately 70% (4/6) of women who underwent CS did not have a mandatory indication for surgery; therefore, the reason for CS was the presence of VVs. Severe complications occurred in 20% (1/5) of VDs vs. 50% (3/6) of CSs.
Summary of cases with lower genital tract varicosities in pregnancy.

The descriptive analysis of these cases provides further information on VVs in pregnancy. In the presence of severe VVs, a CS was preferred more often than VD. These women had a non-negligible complication rate. The only case of severe complication in a VD was reported in 1951 after using “prophylactic” forceps and episiotomy. 13 Although the small sample size cannot provide mandatory indications for daily obstetric practice, the risk-benefit ratio should allow offering the chance of having VD for these women.
In conclusion, our patient reported satisfaction with her successful VD and avoiding surgery. Our findings suggest the following two main points: 1) the mode of delivery in women with huge VVs should be managed by hub obstetric centers with a multidisciplinary consultation including vascular surgeons and radiologists; and 2) on the basis of only a few reported cases, the risk-benefit ratio suggests a chance of having VD for these women.
Footnotes
Author contributions
L.G.: conceptualization, methodology, formal analysis, data curation, patient management, and writing—original draft preparation; M.M, J.D.G., and G.D.C: methodology, data curation, and writing—original draft preparation; A.C.: methodology, data curation, patient management, supervision, writing—review, and editing. All authors have read and agreed to the published version of the manuscript.
Ethics statement
Review board approval was not required because of the nature of this study (case report). The patient provided written informed consent for publication of this case report.
Data availability statement
The data supporting the findings of this study are available within the article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.