
Abstract
To clarify the functional orientation of community health nurses in the continuous care of patients with chronic diseases and to encourage community nurses to play their expected roles in extended nursing work. In this study, conducted from May to July 2020, the staff of Shanghai Community Health Service Center were sampled, and representative medical staff were selected for in-depth interviews and focus group discussions. Eighteen community medical staff members participated. The functions of community nurses in the continuous care of patients with chronic diseases are mainly as follows: ① undertaking individualized projects for patients’ continuous treatment, nursing and rehabilitation; ② creating “peer education” conditions for patients; ③ providing supportive care to family caregivers; and ④ participating in the whole process of family doctor team health management. The results provide a reminder for nurse managers that under the new mission, community nurses need “one specialty and multiple abilities,” appropriate nursing technology and good health management skills. The training of community nurses should better meet the practical needs of patients with chronic diseases.
In the medical context of European and American countries, continuous nursing is essentially a joint service of hospitals and communities. The continuation of information, relationships and management can foster an organic connection for patients upon discharge to different care stages in the community or with their families to make continuous nursing a seamless and continuous process, which plays an important role in chronic disease management. However, in China, it refers to the transfer stage of patients from the hospital to the family, and service providers are often hospital nurses rather than community health care personnel.
This study uses qualitative and phenomenological research methods to explore the functional orientation of community nurses in the continuous nursing of patients with chronic diseases in the community and encourages community nurses to play their expected role in the continuous nursing of patients with chronic diseases.
This study looks forward to continuously innovating the localized continuing nursing model and the model of post service education and continuing education to improve the health service level and ability of community nurses. It is expected to provide a research basis for the development of this work and collaborative work to optimize continuous nursing service for the integrity and consistency of patient care service.
Introduction
Continuity of care, also known as transitional care or long-term care, usually refers to the continuation of care after a patient is discharged from the hospital to his or her family. 1 It is a new nursing model for noncommunicable diseases (hereafter referred to as “chronic diseases”). In addition, it is a response to the health problems and health needs of patients during the transfer period between different medical institutions.2,3 In the medical context of European and American countries, continuous care is essentially a joint service of hospitals and communities. The continuation of information, relationships and management can foster an organic connection for patients upon discharge to different care stages in the community or with their families to make continuous care a seamless and continuous process, which plays an important role in chronic disease management. However, in China, Ying et al 4 pointed out that the domestic concept mostly refers to the transfer stage of patients from the hospital to the family, and service providers are often hospital nurses rather than community health care personnel. Some experts have suggested that the connotation and extension of continuous care services in China should be further defined. Compared with nursing in general hospitals and specialized hospitals, community nursing has its own functions and unique characteristics. The outline of nursing development in the 13th Five-year Plan of China is clear: community nursing has an important task in continuous care.5,6 The concept of continuous care has been proposed for several years; however, due to the lack of unified service content, service standards and implementation plans in China, the role of community nurses in the continuous care of patients with chronic diseases has not been fully elucidated. Many community nurses’ work philosophies lag behind, and they still aim to simply complete medical orders. The service content is limited, the service ability is incomplete, the continuity is poor, and the function is not fully realized, which affects the development of continuous care.7,8 This study uses qualitative and thematic analysis methods to explore the functional orientation of community nurses in the continuous care of patients with chronic diseases in the community and encourages community nurses to play their expected role in the continuous care of patients with chronic diseases.
Materials and Methods
Design/Participant
The objective was to select representative medical staff for in-depth interviews and a focus group discussion at the Shanghai Community Health Service Center from May to July 2020. The sample size was saturated with no emergence of new themes. The inclusion criteria were as follows: ① be a director of a national top 100 community health service center in Shanghai with the goal of “one specialty and multiple abilities” or a nursing director of a community health service center and ② have participated in community basic medical treatment or basic public health work for more than 5 years, with an intermediate professional title or more. A total of 18 medical and nursing staff members participated in the interviews, including 4 who participated in in-depth interviews and 14 who participated in the focus group (Table 1). Prior to the start of the study, potential participants were contacted through the Community Nursing Committee of Shanghai Community Health Association and informed of the interview plan, purpose, content and time. Informed consent and contact information was obtained. Participants knew one another.
Basic Information of the In-Depth Interview Respondents.

Preparation of the Interview Outline
The interview outline was created based on a literature review and group discussion, and 2 respondents were selected for preinterviews. The adjusted interview outline was as follows: ① What do you think community nurses should do to effectively carry out continuous care for patients with chronic diseases? ② Positioning and role of continuous care staff for chronic diseases on the family doctor team; ③ Talk about the practice and prospects of community nursing in the continuous care of patients with chronic diseases.
Data Collection Methods
Interviews were conducted in individuals’ work units, and the focus group was held in the familiar small conference room of the hospital in 2 sessions. The interviews were face-to-face interviews, and the interview content was recorded with built-in mobile phone software. Liu Weiqun was the interview host, and Jinjin Ge assisted with recording. Both authors have rich experience in qualitative research. Jinjin Ge has published 3 papers related to qualitative research during his postgraduate years. Weiqun Liu, as the postgraduate supervisor, supervised 5 graduate students engaged in qualitative research. The other researchers were also trained in qualitative research. The purpose of the interviews was to explore the role of community nurses in the continuation of chronic disease care. To better position the functional responsibilities of community nurses and facilitate the development of the work of community nurses, the interviewer stated his personal thoughts, actions and understandings about the practice according to the interview outline. To better understand the practical experience of the interviewees, the moderator of the focus group guided the discussion in a timely manner and encouraged each participant to speak. The interviews were always conducted in a relaxed and lively atmosphere. All the researchers fully expressed their views, and no interviewees withdrew from the study or were interviewed a second time. The personal in-depth interviews lasted approximately 30 to 60 min, and the focus group discussion lasted 120 min. Two researchers, Yongfang Zhang and Liping Chu, cooperated with Jinjin Ge to transcribe the recordings and sent the transcript to the interviewees for confirmation. After confirmation, the data were analyzed.
Data Analysis
The thematic analysis method was adopted to analyze and research the interview data. 9 Data saturation was achieved in this study. Two research team members, Yongfang Zhang and Jinjin Ge, performed the coding(Figure 1).
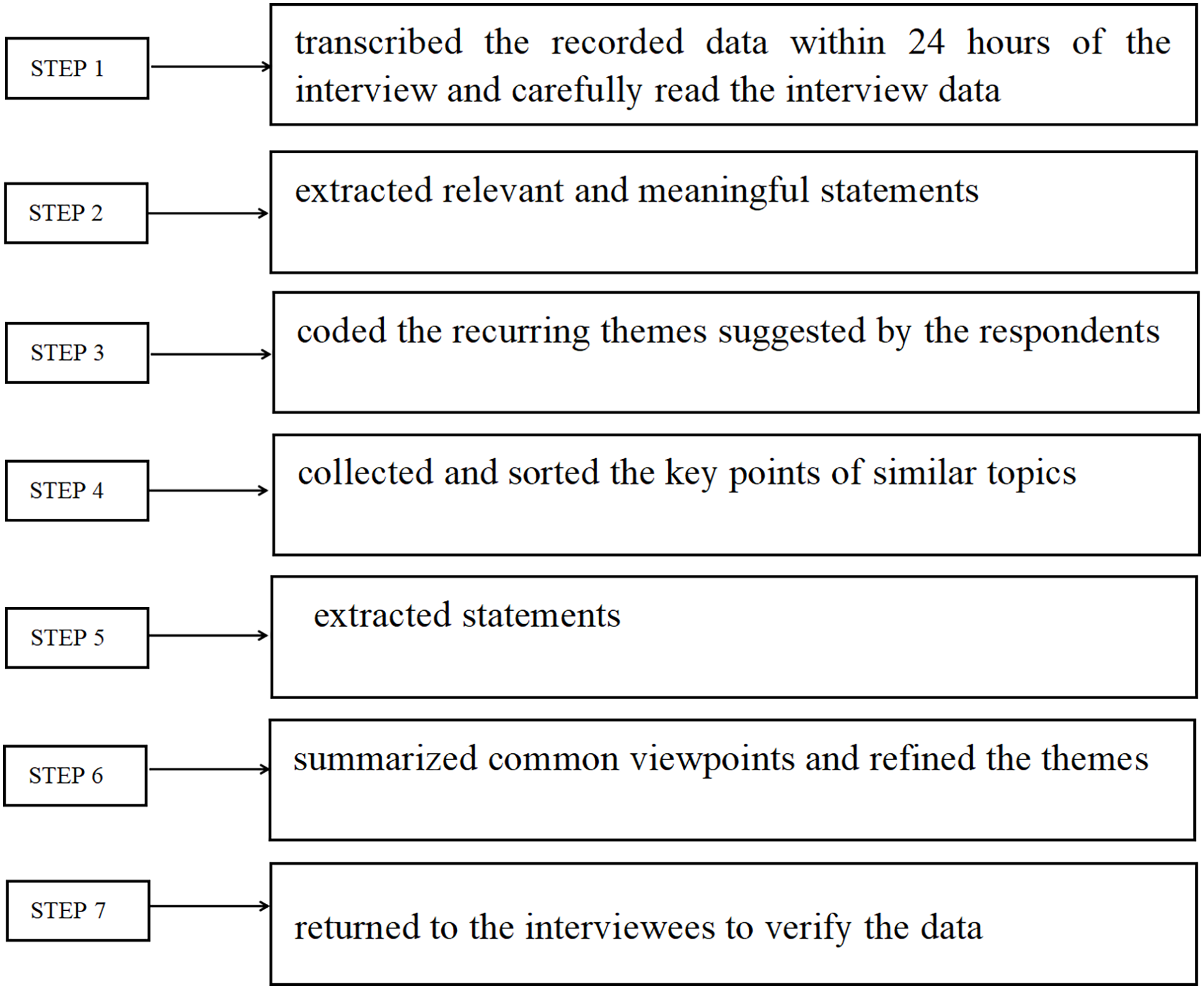
Steps of interview data analysis.
Ethical Consideration
The study was approved by the research ethics committee of Zhoupu Hospital. This study was granted ethical exemption by the Ethics Committee of Zhoupu Hospital (2022-C-193-E01). All procedures were in accordance with the ethical standards of the Declaration of Helsinki. Participants were instructed to read the consent form to ensure that they fully understood the study’s purpose and procedures and the risks and benefits of participating in it. They were assured that their data would be kept confidential and anonymous.
Results
Based on the interview outline, 4 themes and 10 subthemes were extracted for analysis (Table 2).
Thematic Analysis Results of the Functional Orientation of Community Nurses in Chronic Nursing.

Provision of Personalized Extended Nursing Services for Patients, Implementation of Continuous Treatment and Nursing Plans
The diagnosis is clear, and the condition is stable. Patients with chronic diseases are mainly treated and rehabilitated in the community. General practitioners are the decision-makers of specialized diagnosis and treatment, and community nurses are the main executors of continuous care. 10 D2: “Community nurses have the role of a safety net. General practitioners solve diagnostic problems, and the process from diagnosis to treatment mainly involves community nurses.” N10: With the development of medicine, community nursing is no longer a simple injection and medication. In addition to all kinds of common monitoring of blood pressure and blood glucose, the following nursing services can be provided: home oxygen therapy; PICC, fistula and other catheter care; chronic wound and fistula care; peritoneal dialysis care; stroke sequelae, fracture and other rehabilitation care; the application of appropriate technology for traditional Chinese medicine nursing; home hospice care; and community nursing.
Implementation of individualized management
In the community, patients live in a geographically scattered manner, and for the majority of elderly patients, individualized nursing is the focus of continuous care of patients with chronic diseases.
Expansion of the points and areas of disease observation and evaluation
Community nurses should dynamically understand the overall situation and disease process of patients. N11: “Community nurses should evaluate the patient’s current medical history, health risk factors, health knowledge, health behavior, psychological problems, support system and home environment.” N2: “When understanding the patient’s current situation, nurses should understand the patient’s medication and the patient’s curative effect.” N1: “Elderly patients tend to have multiple diseases, and the changes in their condition should be observed according to the characteristics of the patients. The electronic nursing record sheet (file) can systematically collect the patient’s condition data, pictures and other intuitive content, which is convenient for comparison before and after, early identification and effective response to the risk factors for deterioration of the condition.”
Provision of technical guidance for patients’ self-care
Self-care plays an important role in the health care of chronic disease patients in the community. It is very important to guide patients to implement correct and standardized self-care. N10: “After patients with chronic diseases are diagnosed, there will be a process to master self-care skills. A few years ago, I performed a project and successively enrolled 42 insulin injection patients. None of the injection methods was correct. After guidance, these 42 patients learned to inject.” In the guidance of self-care technology, community nurses should take the initiative to make up for the gap between medical institutions. When guiding patients to master self-care technology, they should not copy mechanically, according to the patient’s own management solution and action, and they should teach patients to do self-care in the simplest and most acceptable way.
Effective patient self-health management and guidance
Health education is a kind of nondrug intervention that also accounts for an important proportion of patients’ self-health management. N4: Most patients with diabetes will choose a larger hospital when they seek medical treatment. Many patients will take the medicine after they go home. They will neither regularly monitor blood glucose nor attend follow-up visits, or they will stop taking the medicine when they feel no symptoms. Therefore, patients with diabetes need not only medication but also continuous and comprehensive health guidance and help. N9: “Guide patients to take medicine on time, eat reasonably, exercise reasonably, perform self-test and evaluation, use rehabilitation aids, etc. The content, opportunity and form of individualized health education are the key points that should be considered in the effectiveness of individualized health education.” N6: “When patients find problems during various examinations (blood glucose monitoring, complication examination, etc. ), [nurses should] communicate with patients in time and do a good job in health education on relevant problems.” N7: “Carry out targeted health education for patients in different periods after discharge. For example, health education 1 week and 1 month after fracture operation should have different contents.”
Improvement of patient treatment and rehabilitation compliance
Patient compliance is an important part of successful treatment. The most obvious consequence of poor patient compliance is that the disease is not alleviated or cured or is even aggravated. The cultivation of patients’ treatment and rehabilitation compliance is conducive to improving the effect of continuous care of patients with chronic diseases. N4: “Train patients to transition from passive treatment to active participation in health management.” N10: “Rehabilitation compliance is different for everyone. We should first inform patients of the purpose, significance and positive effects of rehabilitation. When patients make progress, we should actively give positive feedback, encourage and affirm the results, and then carry out rehabilitation training step by step to improve compliance step by step.”
Creation of an Environment of “Peer Education” for Patients
Organizing geographically scattered patients and establishing peer relationships is very beneficial for improving the self-efficacy of patients. N14: “Encourage patients to participate in volunteer activities in health service centers and build partnerships by serving other patients.” N13: “For health education, the family members of patients with diabetes are actively invited to participate in monthly health education activities for patients with diabetes. The family members of patients with good blood glucose control are invited to introduce their family members’ experience in sugar control and their sharing of what they can and have done in sugar control.”
Provision of Supportive Care Services for Caregivers, Guidance on Appropriate Nursing Techniques to be Used
N10: “In many cases, the time for family members to accompany and take care of patients is the longest. If the family members can better master some nursing skills, this will play a decisive role in the recovery of patients. Therefore, direct and appropriate nursing operation guidance can be given to the family members of patients, and some health education materials and links to health science can also be distributed.” N6: “When giving individual guidance to patients, it is recommended that the family members of patients also learn relevant knowledge together.” N5: “In terms of nursing guidance, we should learn to transform thinking and try to convey home care methods to family members in an easy-to-understand popular science way.”
Psychological support for family members
Chronic disease patients in the community live with their families for a long time, especially elderly patients who are unable to move and take care of themselves, which has an impact on the body and mind of their family members. N6: “While communicating with patients, we also pay attention to the cognition of family members on related diseases and communicate and guide them in time.” N3: “Give positive information feedback to family members, establish patients' confidence in rehabilitation and improve their enthusiasm for patient care.” For the families of patients with poor prognosis, especially those with hospice care at home, we should do a good job in their psychological construction, inform them of the worst outcome, try to calmly accept the current situation of patients, and encourage them to do their best. For some families of patients with serious psychological problems, they can also contact the community neighborhood committee to help them obtain the help of the community."
Helping patients and families understand diagnosis and treatment information and resources
The continuous dispensing of drugs for patients with stable conditions, timely medical treatment for patients with changing conditions, timely help of community medical staff for daily health care, etc., are all types of information that caregivers are concerned about. N5: “The medical resources of the patient’s family members are limited, and community nursing staff should provide the required medical resource information for the patient’s family members as much as possible, including 2-way referral, long-term care insurance, etc..” N10: “Helping patients or family members understand how to contact family doctors and obtain necessary and feasible medical care services.” N9: “Nurses can act as coordinators to help patients achieve resource integration.”
Participation in Patient Health Management of the Family Doctor Team, Effective Health Archive Management
The maintenance of community health archives, which record the occurrence, development, treatment and prognosis of residents’ diseases, is one of the important tasks of community health services. D1: “To some extent, community nurses are the assistants of general practitioners and the most important partners, which is reflected in that community nurses are the main managers of health records.” N9: “Dynamic update and management of health records of contracted chronic disease residents and tracking of disease prognosis of discharged patients.” N15: “In the process of managing health records, [nurses should] do a good job in the case management of community patients.”
Cooperation with family doctors in patient follow-up
D3: “Close cooperation between doctors and nurses can improve the quality of continuous service, and the outcome of service objects is good. Under the leadership of general practitioners, nurses give full play to their professional knowledge and technical operation expertise, accurately and timely implement the diagnosis and treatment plans and treatment measures of general practitioners, and do specialized nursing well.” D1 seamlessly connects family doctors in the family doctor team and provides contracted services.
Effective multidimensional and multidimensional coordination
D2: “In chronic disease management, community nurses are very important. They have in-depth, long-term experience in management and can identify problems in time.” N8: “Community nurses also play a connecting, extending, and coordinating role in team chronic disease management. They coordinate between doctors and patients and neighborhood committees and patients, and they coordinate physical examination arrangements and chronic disease screening.” N8: “Team cooperation among family teams and cross-departmental cooperation among multiple departments.” N9: “Work communication and coordination between community nurses and nursing stations, street elderly committees, neighborhood committee elderly workers, community volunteers and volunteer service teams.” N12: “Community nurses and public health doctors should assist in the whole process management. If the condition changes, they should be hospitalized in the community health service center. If it is more serious, they should contact the superior medical institutions of the medical consortium for further diagnosis and treatment to prevent more serious complications.”
Discussion
Community Nurses Are Important Providers of Continuity of Care for Patients With Chronic Diseases
With the increasing number of chronic diseases and limited medical resources, patients with chronic diseases, clear diagnoses and stable conditions mainly return to their families and live in the community, which seems to be an important source of continuous medical care. Through interviews with stakeholders, this research preliminarily clarifies the role that community nurses should play in chronic disease management and extended care, which can also provide a reference for local governments seeking to clarify the responsibilities of community nurses in the future. An Australian study shows that the role of community nurses on multidisciplinary teams caring for patients with chronic diseases is mainly embodied in 6 aspects: advocate, supporter, coordinator, educator, team member and evaluator. 11 The concept of community nurses as advocates needs to be strengthened. This study also determined that the position of a community nurse in chronic disease management is as an executor and collaborator on the family doctor team, rather than the dominant position. To better implement the practices of community nurses in the continuous management of chronic disease care so that patients can smoothly transition from hospital to home, difficulties in the implementation process need to be explored and practical problems resolved. This study also suggests that the most prominent functional orientation of community continuous care is individualized nursing. In the community, the characteristics of geographically scattered patients require community nurses to carry out nursing in the form of individualized nursing. 12 Combined with the characteristics of patients, community nurses carry out personalized self-care and self-health management and promote patients’ compliance with treatment and rehabilitation to meet the diversified and differentiated nursing service needs of patients from an individual perspective. 13 Community nurses give patients multiple forms of diversified nursing care, making continuous care more accurate. 14 Family plays an important role in the process of patient disease rehabilitation. Community nurses provide appropriate nursing operation guidance to patients’ families, which makes continuous care more convenient. Community long-term and seamless professional care is an important guarantee for patients to delay the development of the disease, reduce complications, improve the treatment effect and improve the quality of life after referral or discharge. In terms of continuous treatment, nursing and rehabilitation measures, community nursing, with its unique functional advantages, involves carrying out extended care in the form of direct nursing and optimizing continuous care based on telephone follow-up. Community nurses are the providers of continuous care care for chronic diseases.
“One Specialty and Many Abilities” and the “Combination of Specialty and Generality” of Community Nurses Are the Basis for Effective Community Continuous Care
In today’s aging society, there are a large number of elderly patients with chronic diseases in the community. The coexistence of multiple diseases is a significant feature. It is very common for patients to have multidimensional nursing needs. The results of this study suggest that community nurses providing continuous care for patients with chronic diseases not only have long-term experience and multiple and multidimensional nursing contents but also cover a wide range, which establishes very high requirements for the specialized nursing, communication and guidance ability of community nurses. 15 Especially in the community control of emergency public health events, due to the presence of elderly people and patients with mobility difficulties, the direct care function of community nursing is more prominent, which can effectively solve the adverse impact of emergency control or inconvenient travel on patients’ medical treatment. When designing the training of community nursing staff, managers should be close to the needs of patients’ treatment and rehabilitation and the practical needs of nursing staff and should pay attention to the scientificity, standardization and innovativeness of the training content. It is necessary to strengthen the training of specialized nurses and provide specialized nursing care for elderly patients with chronic diseases. In the United States, advanced community practice nurse specialties include emergency, home health, adult, geriatric, neonatal, and pediatric care, as well as women’s health, physical and mental health, school health, and subspecialties such as oncology, diabetes, and neurological disease. Each specialized training has a different emphasis. 16 The UK also offers specialized training for community nursing in community health, general care, mental health, pediatrics, health supervision, and family care. 17 The specialties covered by community nurses in various provinces include wound ostomy, venous therapy, diabetes, clinical nutrition, maternal and infant care, tumor, critical illness, cardiovascular disease, emergency and first aid. However, the number of programs is small, and their popularity is not high; thus, services cannot correspond to the characteristics of the community dominated by chronic diseases and cannot meet the population’s needs.18,19 The Shanghai Community Nursing Committee applies knowledge management theory to cultivate the community characteristic of “one specialty and multiple abilities” for management nurses and the “combination of specialty and generality” to improve the comprehensive ability of nurses’ specialized nursing, guide them to apply what they have learned, and provide standardized, safe, effective and convenient continuous care for community patients with chronic diseases. The implementation of the project provides in-home patients with convenient and fast access to specialized nursing support and more targeted, professional, rich and effective health care.
The Link Between Patient Information, Relationships and Management is the Premise of Good Continuing Care
Currently, extended care has not completely broken through the barriers of patient information, relationships and management between hospitals and community health service centers, which affects the implementation of extended care in China. The literature also suggests that information transfer has been the most prominent of the content areas of Continuity of Care. 20 Information is insufficient regarding care needs, goals, nursing interventions and outcomes. 21 Wu proposed that to achieve continuous care, it is also necessary to improve the mechanisms and facilitate the coordination and cooperation between institutions and personnel through the intervention of information technology. 22 In the practice of continuous care, 2-way referrals and other medical reforms proposed by the National Health Commission, patient information and treatment services continue across institutions, hospitals and nurses, and the internal division of labor and cooperation, information connectivity and seamless transitions still need to be sorted out.
Limitations to This Study
Due to the limitation of the study design, we only explored the role of community health nurses in the continuation of care for patients with chronic diseases from the perspective of community health managers and community nurses. There was a lack of support, such as the perspective of partner family doctors and patients. Thus, the role of community nurses in the continuation of chronic disease care in these 2 aspects was not fully explored. This will be part of our future research.
Conclusion
When practicing the requirements of continuing care, 2-way referral and other medical reform work proposed by the National Health Commission, patient information and treatment services are continued across institutions, and the division of work, cooperation and connectivity between hospitals, nurses in superior hospitals, community nurses, and family medical teams needs to be established. Wu suggests that information technology is key to realizing continuous care, improving the mechanisms and facilitating coordination and cooperation between institutions and personnel. 22 This study finds that innovating the localized continuing nursing model and the model of postservice education and continuing education 3 will improve the level of health care and the abilities of community nurses. This study can serve as a reference for the development of this work and collaborations that will optimize continuous care services for the best and consistent patient care.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
Yuzhong Yan, Weiqun Liu, and Jinjin Ge contributed to conception and design of the study. Enfang Fan, Xi Yang, and Liping Chu conducted data acquisition. Jinjin Ge, Yongfang Zhang, and Enfang Fan carried out data analysis. Jinjin Ge and Yongfang Zhang contributed to interpretation of data. Yuzhong Yan, Weiqun Liu, and Jinjin Ge drafted the manuscript. Jinjin Ge, Yongfang Zhang, and Xiaoling Zhou revised the manuscript. All the authors read and approved the final manuscript.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are not publicly available due to privacy but are available from the corresponding author on reasonable request.
Author’s Note
Xiaoling Zhou Guizhou is also affiliated to Medical University, Guizhou, China.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by by grants from Pudong Health Bureau of Shanghai (PWRd2019-03) and the Shanghai Pudong New Area Health System Discipline construction Program (PWYts2021-02). The funding bodies had no role in the study design, data collection, analysis, interpretation of data, or writing the manuscript.
Ethics Approval and Consent to Participate
The study was approved by the research ethics committee of gongli hospital of Shanghai Pudong New Area (2022-C-193-E01). All procedures performed in studies involving human participants were in accordance with the ethical standards of the Declaration of Helsinki. Participants were instructed to read the consent form to ensure they fully understood the study’s purpose and procedures, and the risks and benefits of participating in it. They were assured that their data would be kept confidential and anonymous.
Consent for Publication
Not applicable.