
Abstract
Protective behaviours could minimize COVID-19 spread.
Our research aims to find out how different information sources affect the intention to adopt protective behaviours.
Our research results implicated the potential measures to promote health education messages in a public health emergency to the public.
Introduction
An outbreak of pneumonia associated with the severe acute respiratory syndrome (SARS) was reported in Wuhan, China in December 2019 1 On January 2 30, 2020, the World Health Organization (WHO) declared this outbreak as a Public Health Emergency of International Concern (PHEIC). 2 On February 12, 2020, the WHO named this disease ‘The Novel Coronavirus 2019 Disease’ (COVID-19). 3 Ultimately, on March 11, 2020, the WHO declared the COVID-19 as a pandemic. As COVID-19 spread across the world in the following month, over 550000 people were infected and 47646 people died of COVID-19 by April sixth, 2020. China was even more heavily affected by COVID-19. By April sixth, 2020, over 80,000 were infected and 3349 people died of COVID-19 in China. 4 As over 60% of confirmed infected people reported a resident history of living in Wuhan city, 5 the Chinese government started to impose the lockdown to curb COVD-19 spread in major cities including Beijing and Shanghai. 6 Given that a majority of those infected with COVID-19 were located in urban areas, it suggested that people living in urban areas in China may have a high risk to contract COVID-19.
Understanding how people at high risk respond to the COVID-19 can guide public health interventions. For example, previous studies identified erroneous beliefs that the use of ivermectin, an antiparasitic agent used to treat parasitic infestations, was the best way to prevent COVID-19 and the use of cow dung and urine was the best way to cure COVID-19.7,8 These knowledge deficits could be addressed by public health education. Infectious diseases, such as COVID-19, as a major public health threat are best dealt with the use of vaccination. Unfortunately, in the first year of a pandemic, vaccines are generally unavailable. Instead, non-pharmaceutical behavioural protective measures can play a major role in minimizing the contagion of a novel virus. 9 Therefore, it is important to examine key factors for promoting the adoption of the recommended protective behaviours by as many individuals as possible through public health education.
Protective behaviours for decreasing the likelihood of infection and disease severity can be classified as preventive behaviours (e.g. hand washing, mask wearing), avoidant behaviours (e.g. avoiding crowds and public transport) and management of disease behaviours (e.g. taking antiviral medication). 10 Although behaviours from all these categories are effective to minimize the contagion of COVID-19, handing washing, masks wearing and social distancing have been mainly recommended by the National Health Commission of the People’s Republic of China. 11 However, there are key factors that influence people’s intention to adopt their protective behaviours. For example, how people perceive the risk of an infectious disease appears to influence their adoption of protective behaviours. 12 One theory to identify key factors to the adoption of protective behaviours is Protection Motivation Theory 13 (PMT). PMT provides a useful theoretical framework for understanding people’s response to a threat. PMT focuses on people’s motivation to adopt protective behaviours to avoid potential negative consequences. 13 It proposes that a high threat appraisal of a person assessed as perceived risk (i.e. the severity of the disease and the perceived vulnerability) will lead to the adoption of protective behaviour when the person believes that a protective behaviour will effectively reduce the risk (the perceived response efficacy) and that one’s self is capable of implementing the protective behaviour (the perceived self-efficacy). Therefore, high levels of perceived risk are assumed to predict the adoption of protective behaviours.
However, there are several questions regarding to determinants of intention to adopt protective behaviours during a pandemic. For example, worry as a cognitive process has been most closely examined in relation to anxiety and reflects negative affectivity that influences the perception of susceptibility to risk.14,15 Thus, adopting protective behaviours might be associated not only with the perceived risk for oneself but also with worry about contracting from others. 16 There are limited studies that assess social desirability bias when adopting protective behaviours. Social desirability bias is identified as people providing information in a perspective that they believe will be viewed favourably. 17 An increase in socially desirable responding may mask the intentions to adopt protective behaviours. It is often difficult to identify whether protective behaviours actually were adopted, or the adoption of protective behaviours was reported due to social desirability bias.
The choice of information sources may determine people’s knowledge to adopt protective behaviours. 18 In this study, information of COVID-19 disseminated through government-agency sources (i.e. government website information) in China is identified as ‘formal information’. Information of COVID-19 disseminated through social media (i.e. Weibo) and causal interpersonal communication between friends and family in China is identified as ‘informal information’. Trust is a key factor for effective communication of risk for uncertain infection risks and trust in perceived information influences behavioural change.19,20 Therefore, we propose that trust in formal and informal information may function differentially to adopt protective behaviours through effects on perceived risk and worry. Furthermore, this study also examined whether a measure of social desirability bias was associated with the intention to adopt protective behaviours.
Methods
The Theoretical Framework
A theoretical referential model (Figure. 1) was constructed that incorporated elements of trust in formal information (i.e. government website information, national television information and reports from government leaders), trust in informal information (i.e. social media, friends and family members), perceived risk, worry and protective behaviours (i.e. hand washing, mask wearing and social distancing). Due to limited literature on the relationships between trust in different sources of information, perceived risk, worry and protective behaviours, we hypothesized a model testing all possible relationship permutations between trust in different sources of information, perceived risk, worry and protective behaviours (Figure 1).

A conceptual model for understanding intention to adopt protective behaviours against COVID-19.
Study Design
This study was conducted via an online survey and was designed to measure 4 different constructs: worry about contracting COVID-19, the perceived risk of contracting COVID-19, trust in information about COVID-19 from formal source (i.e. government website information, national television information and reports from government leaders) and informal sources (i.e. social media, friends and family members), and protective behaviours (i.e. hand washing, mask wearing and social distancing) against COVID-19. In addition, the study included a general demographic questionnaire, and the social desirability scale. The complete compiled survey was available online for approximately 2 weeks until an adequate number of participants had completed it.
Participants
Participants self-identified a resident history of living in urban areas in China, as this study focused on participants that live in urban areas in China; and only 18 years and older were included. Participants were recruited via social media and via snowball sampling. Due to the number of constructs included, approximately 119 participants were required. 21 A total of 162 participants were recruited from March second to March 16th, 2021, and the survey was available online from November 2020 through November 2021. Institutional Review Board (IRB) approval with reference number 101820 was obtained prior to the start of the study from Adelphi University’s Institutional Review Board. Informed consent was obtained from participants prior to their participation in the study. There was no specific compensation for participating in this study. In order to ensure participants’ confidentiality, an anonymous link and a quick scan code were used to distribute the survey. The survey was translated and administered in Chinese.
Measures
All measures utilized were made available online through Qualtrics, an online survey construction and administration website. The designed survey was tested in a pilot study in terms of constructing items. Core items for the survey used in the pilot study were retained throughout. Minor changes were made; 1 item on trust in informal information about COVID-19 and 1 item on social distancing were deleted to refine the measurement.
Demographic questions included age, gender and education level. Social desirability was measured using Marlowe and Crowne social desirability scale. 22 This widely used measure consists of 33 self-report items that assess individual-level social desirability bias. It utilizes a true and false response category. It has been shown to have a good reliability (r = .88), as well as good convergent validity with similar measures (r = .46–.80). 22
Trust in formal information (i.e. I trust reports from government leaders about COVID-19) was assessed with 3 items. Participants were asked about their agreement with these 3 items. Responses were made on five-point scales of agreement ranging from ‘strongly disagree’ to ‘strongly agree’. The reliability of these 3 items was assessed using Cronbach’s alpha (α), which at .95 indicated the internal consistency between items was high. 23 The convergent validity of the construct was assessed using the average variance extracted (AVE), which at .86 indicated a good convergent validity. (Table 1) 24
Trust in informal information (i.e. I think it is the best to know about COVID-19 by listening and watching people around me talk about it) was assessed with 3 items. Each item was assessed using responses on categorical five-point scales of agreement. The reliability of these 3 items was assessed using Cronbach’s alpha, which at .63 indicated the internal consistency between items was acceptable. 23 The convergent validity of the construct was assessed using AVE, which at .65 indicated a good convergent validity. (Table 1) 24
Worry about contracting COVID-19 (i.e. I am concerned about contracting COVID-19) was assessed to indicate the level of worry with three items. Responses were made on five-point scales of agreement ranging from ‘strongly disagree’ to ‘strongly agree’. The reliability of 3 items was assessed using Cronbach’s alpha, which at .79 indicated the internal consistency between items was high. 23 The convergent validity of the construct was assessed using AVE, which at .60 indicated a good convergent validity. (Table 1) 24
Perceived risk of contracting COVID-19 (i.e. there is a chance that COVID-19 spreads in my community) was assessed to indicate perceived probability of developing COVID-19 with 3 items. Each item was assessed using responses on categorical five-point scales of agreement. The reliability of 3 items was assessed using Cronbach’s alpha, which at .71 indicated the internal consistency between items was high. The convergent validity of the construct was assessed using AVE, which at .49 was below the threshold. If the AVE value was less than .5, but the composite reliability (CR) which at .74 was higher than .6, the convergent validity of the construct is still adequate. (Table 1) 24
Hand hygiene was assessed with 3 items to indicate frequencies of use of 3 hand hygiene practices: hand washing after sneezing, coughing and touching noses; use of liquid soap for hand washing, and hand washing after touching common objects. Reponses were made on a five-point scale of frequency ranging from ‘never’ to ‘always’. The reliability of 3 items was assessed using Cronbach’s alpha, which at .82 indicated the internal consistency between items was high. 23 The convergent validity of the construct was assessed using AVE, which at .62 indicated a good convergent validity. (Table 1) 24
Social distancing behaviours were assessed with 3 items to indicate frequencies of the adoption of 3 social avoidance behaviours due to COVID-19: avoiding going to crowded places, avoiding using public transport and avoiding eating out. Reponses were made on a five-point scale of frequency ranging from ‘never’ to ‘always’. The reliability of 3 items was assessed using Cronbach’s alpha, which at .73 indicated the internal consistency between items was high. 23 The convergent validity of the construct was assessed using AVE, which at .5 indicated a good convergent validity. (Table 1) 24
Wearing masks were assessed with 3 items to indicate frequencies of the adoption of wearing masks under 3 different circumstances due to COVID-19: wearing masks when having close contact with other people, wearing masks when using public transport, and wearing masks in crowded places. Responses were made on a five-point scale of frequency ranging from ‘never’ to ‘always’. The reliability of 3 items was assessed using Cronbach’s alpha, which at .82 indicated the internal consistency between items was high. 23 The convergent validity of the construct was assessed using AVE, which at .64 indicated a good convergent validity. (Table 1) 24
Reliability and Validity Analysis.

Data Analysis
The proposed model (Figure 1) was evaluated by using Analysis of Moment Structure (AMOS, ver. 28). Structural Equation Modelling (SEM) is a statistical technique for simultaneously estimating and testing the relationships between measured variables and latent variables and provides the accommodation with measurement errors of the constructs in the model. Adequacy of the conceptual model was tested before testing the full structural model. The conceptual model (Figure 1) was tested using SEM with protective behaviours, entered the model as observed variables, perceived risk and worry entered in the model as mediator variables. Trust in formal information and trust in informal information were entered as latent variables. In the conceptual model, the disturbances of these 3 protective behaviours outcomes were assumed to be correlated where disturbances represent the unexplained variances. 25 For example, adopting protective behaviours during a public health emergency could be influenced by some causes which were not fully explored such as previously existing health conditions. 26 During the COVID-19 pandemic, these 3 protective behaviours were recommended and occurred at the same time. As such, it is reasonable to assume that all these 3 behaviours were correlated and influenced by some unexplained causes. To test the full structural model, maximum likelihood estimation (MLE) was used to estimate squared multiple correlations, regression weights and standardized estimates simultaneously. 25 Multiple model fit indices including Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), and Root Mean Squared Error of Association (RMSEA) were used to evaluate the model fit, and a CFI >.9, TLI >.95, and RMSEA <.05 indicated a good model fit. 27
Results
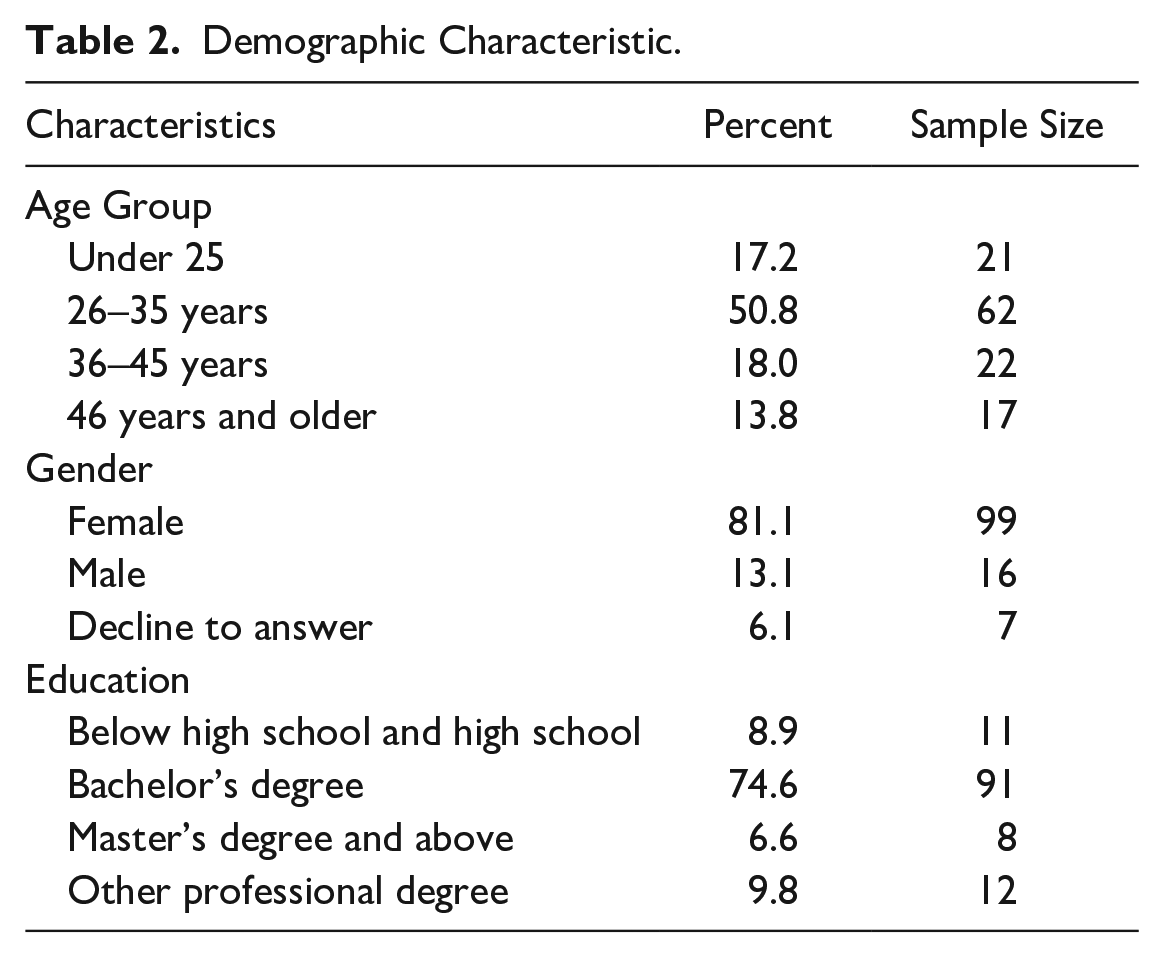
A total of 122 valid respondents were retained by excluding those who did not complete the entire survey, a response rate of 75.3%. Respondents consisted of 16 males (13%) and 99 females (81%); 7 respondents prefer not to answer about their gender. About half (51%) of the respondents indicated that they were 26–35 years old. 91% of the respondents indicated that they had at least a bachelor’s degree (Table 2).
Demographic Characteristic.
Respondents reported they mostly or completely trusted information from formal sources (reports from government leaders, government website and TV) (mean = 4.57, scale 1–5). In contrast, respondents reported they have less trust in information from informal sources (social media, friends and family) (mean = 3.03, scale 1–5). Respondents generally reported low perceived risk of COVID-19 (mean = 2.09, scale 1–5) while they reported a greater worry of contracting COVID-19 (mean = 4.09, scale 1–5). Adopting the protective behaviours recommended by National Health Commission of the People’s Republic of China for hand washing (mean = 4.43, scale 1–5), mask wearing (mean = 4.85, scale 1–5) and social distancing (mean = 4.00, scale 1–5) were highly prevalent. 63.9% of respondents (78 out of 122) reported above average score in social desirability (mean = 7.4, scale 0–13).
The SEM model (Figure 2) fitted well to the data with CFI = .992, TLI = .975 and RMSEA = .044, respectively. The standardized covariance, path coefficients and the explained variance of each endogenous variable are shown in Figure 2. Trust in formal information was significantly associated with perceived risk (β = −.18) and significantly and positively associated with worry (β = .28). Trust in informal information was significantly and positively associated with perceived risk (β = .57). Subsequently, perceived risk was significantly associated with social distancing (β = −.17), and worry was significantly and positively associated with mask wearing (β = .25) and significantly associated with hand washing (β = −.27). Trust in formal information was significantly and positively associated with hand washing (β = .26) while trust in informal information was significantly and positively associated with social distancing and hand washing (β = .26). Perceived risk was significantly and positively associated with worry (β = .32). The model explained 35.4% of the variance on perceived risk but only explained 14.9% of the variance on worry, 6.5% of the variance in social distancing, 6.2% of the variance in mask wearing and 15.0% of the variance in hand washing.

A structure equation model for understanding intentions to adopt protective behaviours against COVID-19.
In Figure 2, it was hypothesized that effect of trust in informal information to adopt social distancing behaviour was mediated by perceived risk. The direct effect of trust in informal information and indirect effect of trust in informal information via perceived risk to adopt social distancing behaviour including the point estimate and 95% confidence interval are shown in Table 3. Trust in informal information has a direct significant effect on adopting social distancing behaviour (point estimate = .19, 95% CI: −.01 to .4). While trust in informal information had a significant indirect effect on perceived risk (point estimate = .64, 95% CI: .48–.81), perceived risk did not have a significant indirect effect on adopting social distancing behaviour. This result indicated that perceived risk did not mediate the relationship between trust in informal information and social distancing behaviour. In Figure 2, it was hypothesized that effect of trust in formal information to adopt hand washing behaviour was mediated by worry. The direct effect of trust in formal information and indirect effect of trust in formal information via worry to adopt hand washing behaviour including the point estimate and 95% confidence interval are shown in Table 3. Trust in formal information had a significant direct effect on adopting hand washing behaviour (point estimate = .28, 95% CI: .12–.42). Trust in formal information had a significant indirect effect on worry (point estimate = .20, 95% CI: .04–.35) and worry had a significant indirect effect on adopting hand washing behaviour (point estimate = −.25, 95% CI: −.42 to −.07). This result indicated that worry partially mediated the relationship between trust in formal information and hand washing
The Direct and Indirect Effect of Trust in Informal/Formal Information on Social Distancing/Hand Washing Via Perceived Risk/Worry.

*Formal: Trust in formal information; informal: Trust in informal information.
The simple moderation model which hypothesized that perceived risk to adopt social distancing behaviour and worry to adopt mask wearing and hand washing behaviours were moderated by social desirability bias was tested. The simple moderation model fitted well to the data (CFI = .99, TLI = .95, RMSEA = .47). The interaction between perceived risk and social desirability bias was not statistically significant while the interaction between worry and social desirability bias was statistically significant (point estimate = −.05, 95% CI: −.09 to −.02) as shown in Table 4. Social desirability bias significantly moderated the relationship between the adoption of mask wearing behaviour and worry.
The Effect of Social Desirability on the Relationship Between Worry and Mask Wearing.

Discussion
Based on our hypothesized SEM model, we investigated how perceived risk and worry mediated the effects of trust in different information sources to adopt protective behaviour against COVID-19, and how social desirability interacted with perceived risk and worry to affect the adoption of protective behaviour in China. Our study found that the respondents generally had mostly or completely trusted information from government-agency source and reported low perceived risk of COVID-19. As indicated by the SEM, respondents trusted more in formal information had lower perceived risk of COVID-19 which in turn was associated with less people agree to adopt social distancing behaviour. One possible reason is that respondents reported more trust in information from government-agency source were more optimistic about avoiding COVID-19 and had confidence that China can win the battle against COVID-19. Both optimistic about COVID-19 and confidence in Chinese government further account for less people agree to adopt social distancing behaviour.
In contrast, according to the SEM, respondents trusted more in informal information had higher perceived risk of COVID-19. This finding provides some insights that information disseminated through social media and interpersonal communication would help people understand the risks more compared to information disseminated through government-agency source. According to the SEM, respondents trusted more in formal information had greater worry of contracting COVID-19 which in turn was associated with more respondents agree to adopt mask wearing behaviour but less respondents agree to adopt hand washing behaviour. This suggests that seeking information from government-agency source can produce concerns given the dangerous infectious disease. Subsequently, more people preferred to wear masks to reduce worry about contracting COVID-19 and maintain a good health status. One possible reason for less respondent agree to adopt hand washing behaviour could be respondents were more likely to stay at home as concerns about contracting COVID-19 grow. Our study also found that greater trust in informal information was associated with more people preferred to wash hand and social distancing. This suggests that information from social media and interpersonal communication may help to promote different types of protective behaviours. When social desirability bias was low, people have a greater worry about contracting COVID-19 would be more likely to wear masks. When social desirability bias was high, the willingness to wear masks remained same while worry about contracting COVID-19 increased. One possible reason is that mask wearing had been widely adopted by people living in China. Wearing masks in public would not be necessarily viewed favourably by others.
Limitations of this study need to be acknowledged. First, factor loadings on some items were relatively small. As a consequence, the validity for 1 latent variable was weaker than expected. Second, a relatively low explained variance of protective behaviours was found, indicating that other factors need to be considered for the prediction to adopt protective behaviours in the future study.
Conclusions
This study demonstrates the influence of trust in different information sources on 3 different types of protective behaviours during COVID-19 and provides important insights into how perceived risk and worry would affect the adoption of health protective behaviours. This study found people trust in informal information from social media and interpersonal communication would be more likely to adopt mask wearing and hand washing protective behaviours. It indicated the potential measure to promote health education messages through informal source to help the general public to adopt more types of protective behaviours. People trust in formal information from government-agency source has lower perceived risk of COVID-19 and less likely to adopt social distancing. It may suggest that the health education message about perceived risks from government-agency source need to be adjusted to promote the adoption of social distancing behaviour. People trust in formal information showed a greater worry about contracting COVID-19 and more likely to wear masks. It may suggest that the public health message from government-agency source about worry would persuade more people to wear mask. These findings can provide support to influence the effectiveness of public health disease control measures and the dissemination of different health education messages in different platforms in the future.
Supplemental Material
sj-docx-1-inq-10.1177_00469580221090411 – Supplemental material for Source of Information on Intentions to Adopt Protective Behaviours During COVID-19 in China
Supplemental material, sj-docx-1-inq-10.1177_00469580221090411 for Source of Information on Intentions to Adopt Protective Behaviours During COVID-19 in China by Jiadong Yu, Bernard S. Gorman and Carolyn M. Springer in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.