
Abstract
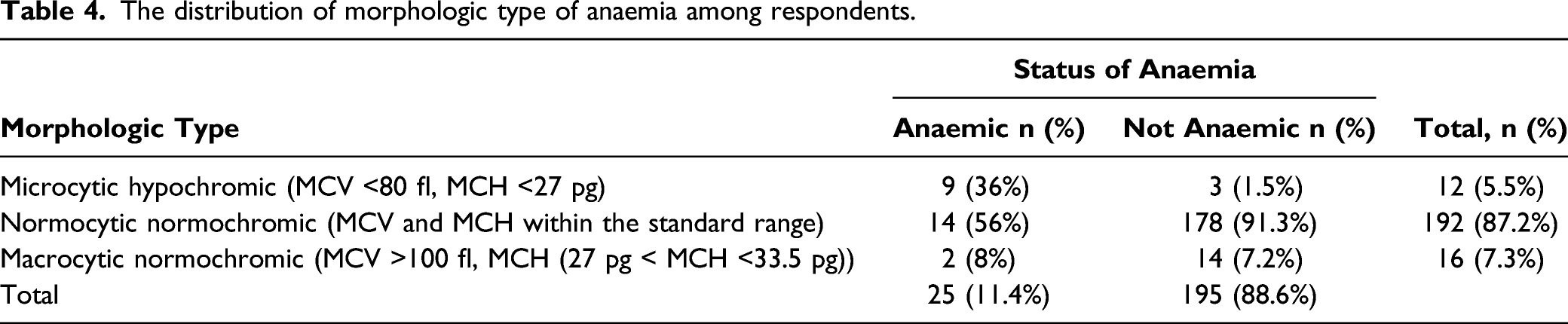
Anaemia during pregnancy is a major public health concern. Despite its wide scope and adverse effects including increased maternal and perinatal morbidity and mortality, and long-term adverse effects on the newborn, appropriate interventions using upstream approaches to public health have largely not been implemented. This study investigated the prevalence and associated factors of anaemia among pregnant women in four health facilities in the Kwabre East Municipality. A cross-sectional survey with a two-stage sampling technique was conducted on 220 pregnant women who attended antenatal care at the selected health facilities. Interview-based structured questionnaires were used. Bivariate and multivariate logistic regression were used to identify predictors. The prevalence of anaemia was 11.4%. Few women (25) were anaemic and morphologically, 14 (56%) had normocytic normochromic anaemia and 9 (36%) had microcytic hypochromic anaemia. Iron deficiency was reported in 19 (8.6%) pregnant women. Independent predictors of anaemia were iron sulphate intake (AOR [95% CI] = 3.16 [1.15, 7.37], ANC follow-up during pregnancy (AOR [95% CI] = 3.07 [1.59, 7.99], household size of ≥5 (AOR [95% CI] = 3.58 [1.75, 9.52], folic acid intake (AOR [95% CI] = 5.29 [2.65, 12.39] and the period in pregnancy AOR [95% CI] = ≥36 weeks 3.2 (1.3-4.5). Though anaemia prevalence has been low in urban areas as previously reported, collaborated healthcare measures that aim at eradicating the menace are encouraged. Maternal healthcare interventions including the administration of folic acid, regular iron sulphate intake and intensive education on early ANC are recommended.
Women’s health is crucial due to the contributions they play in the development of societies.
It will inform policies made by policymakers on the need to promote women’s health.
Institutions and individuals should intensify campaigns on maternal health-care use.
Introduction
Anaemia is a major public health problem globally among pregnant women in both low-and middle-income countries.1,2 The menace exerts serious consequences on the health of pregnant women and the unborn baby.3,4 In a report released in 2011 by the World Health Organisation, 1 the global anaemia prevalence for pregnant women and all women of reproductive age was 38.2% and 29.4%, respectively. The prevalence of anaemia is more alarming in the regions of South-East Asia, Eastern Mediterranean and Africa, which ranges from 37.7% to 41.5% for non-pregnant women and 38.9% to 48.7% for pregnant women respectively. 1 It is disheartening that the highest prevalence of anaemia is among children under 5 years and pregnant women.1,5
Anaemia during pregnancy is a major cause of maternal morbidity, and it is estimated with a haemoglobin concentration of less than 10 gm/dl. Any patient with haemoglobin of less than 11 gm/dl to 11.5 gm/dl at the start of pregnancy will be treated as anaemic. 5 Anaemia during pregnancy has both maternal and foetal consequences, hence, a major cause of morbidity and mortality among pregnant women especially in developing countries.6,7 It is in this regard that the WHO requires blood testing to detect syphilis and severe anaemia as major components of Antenatal Care (ANC) among pregnant women.1,8
The causes of anaemia during pregnancy are multidimensional. However, in developing countries, it is predominantly nutritional deficiencies in iron, folate and vitamin B12. Other causes of anaemia are loss of blood due to bleeding, failure of bone marrow to produce sufficient number of RBCs causing aplastic anaemia, and parasitic diseases. 9 Iron deficiency is the most common cause of anaemia and undermines the cognitive development of children and low productivity among adults. 10 Anaemia infections among pregnant women is a public health problem in Ghana. 3 However, among the regions in Ghana, anaemia prevalence ranges from as low as 2% in the Eastern region to 19% in the Northern, Upper East and Upper West regions. There is also a large variance in anaemia prevalence by ecological zones in Ghana. 11 Anaemia is 3 times higher in the Savannah zone (15%) than in the Coastal (4%) and Forest (5%) zones. 11
There have been a number of studies on anaemia in pregnant women including those in Ghana,12-15 Tanzania,7,16 Nicaragua, 17 Nigeria,18,19 Ethiopia, 20 Pakistan10,21 and Vietnam. 22 Specifically, the work of Khan et al. 21 focused on pregnant women from tertiary health facilities in urban settings and was limited to iron, folate and cobalamin deficiency in anaemic pregnant women. While Ewusie et al. 12 exclusively focused on under 5 children among Ghanaian population, Aikawa et al. 22 stressed on risk factors for iron-deficiency anaemia among pregnant women living in rural Vietnam. Anderson et al. 15 considered multiple factors including anaemia, obesity, hypertension and diabetes among residents of selected communities in Ghana., Fuseini et al. 13 in their study in the Kassena-Nankana district of Northern Ghana examined the association between anaemia and Plasmodium and or intestinal helminth infections during pregnancy.
In the Kwabre East Municipality, the focus of this study, the trend of anaemia in pregnancy cases from 2009 to 2012 has been progressively encouraging. In 2009, there were 1,851 (37.8%) reported cases, 2010 had 1,428 (29.6%) cases, 2011 witnessed 1,115 (24.3%) cases and in 2012, 1,032 (23.2%) cases were reported. In 2013, 825 anaemia in pregnancy cases were recorded with 430 reported in 2014. 23 There has been downward trend in anaemia prevalence among pregnant women in the municipality. Anaemia prevalence among pregnant women is a major indicator used to assess the effectiveness of interventions focused on maternal health care in Ghana. According to the Kwabre East Assembly, 24 the key reason for low anaemia prevalence is the implementation of focused ANC by the government of Ghana, which helps pregnant women to be taken care of by a particular healthcare provider through the period of pregnancy. Despite this intervention, anaemia is still prevalent in the municipality, though in lower rates. There is therefore, the need to undertake a study to determine the factors contributing to anaemia prevalence in the municipality six years after the implementation of the focused ANC. The findings from this study would be useful in informing maternal health policy and interventions in Ghana.
Methods
Study Setting
The study area is one of the 32 newly carved Municipalities by the government of Ghana in 2018. The Kwabre East Municipality was carved out of the former Kwabre Sekyere District in 1988. It is located almost in the central portion of the Ashanti region and within latitudes 60°45′ and 60°50′ North and longitudes 10°30′ and 10°35′ West. 11 The Municipality has a total land area of 246.8 square kilometres constituting about 1.01% of the total land area of Ashanti Region. The population of the Municipality according to the 2010 Population and Housing Census stands at 115,556 with 55,106 males 60,450 females. Data from the Kwabre East Assembly 24 reveal that ANC utilisation level is high and most pregnant women make use of the service due to the intense education embarked on by the District Health Directorate towards achieving the WHO standards of service use.
Study Design and Sampling
This study forms part of a larger research that investigated the socioeconomic determinants of antenatal care utilisation by pregnant mothers in selected health facilities in the Kwabre East Municipality. The study adopted a facility-based cross-sectional survey design to investigate the predictors of anaemia prevalence among pregnant women in the Municipality. These health facilities are publicly owned and were purposively sampled based on the administrative divisions of the Municipality and the free maternal health policy introduced by the Ghana government in 2003. 33
Study facilities and their Selected Sample Sizes.

The sample size was obtained by using the fractional approach, which suggests that any fraction of an intended population that is 10% or more is deemed representative especially if the sample is scientifically selected.
25
In a related study by Burns and Bush,
26
it was revealed that a sample size of 5% of a population of study is deemed appropriate to achieve its purpose if it was scientifically chosen. Hence, the sample size of 22.6% of the total population from the selected health facilities was deemed to be scientifically appropriate. The proportional stratified sampling technique was used to determine the sample sizes using the formula; n= (ni/N) *S, where ni= facility population, N= total population and S= sample size. The same formula was used based on the variance in population of study respondents from selected facilities. As a result, the margin of error for the determination of the sample size was .02 and the proportion of the study population likely to agree that pregnancy anaemia is a major public health concern was assumed as 10% (0.10). The figures were then substituted into the formula outlined by Moser and Kalton
27
for determining sample size. The formula is given as

Data Collection and Analysis
The selection was based on the level of ANC attendance at the selected prenatal outpatient departments of selected facilities using the Municipal Health Information Management System software. 23 In effect, a list of pregnant women aged between 15 and 49 was obtained from the ANC units of the sampled health facilities. Subsequently, simple random sampling technique was used to select 220 pregnant women for the study. Data collected from respondents included demographic characteristics, health status, family planning services, social support systems, quality of service, choice of facility, level of utilisation and views on caregivers.
A face-to-face interview using structured questionnaire was employed to obtain data about sociodemographic characteristics, dietary habit, ANC follow-up, multivitamin intake, taking meat and animal products, sulphate intake, folic acid intake, sleeping under insecticide treated nets (ITNs), use repellents/coils/sprays and nutrient supplementation at their pregnancy period at the time of data collection. Blood pressure, height and weight and body mass index (BMI) of respondents were calculated in the forms of (weight (kg)/height (m2)). Serum ferritin levels using the DPC Immulite 1 ferritin assay (Diagnostic Products Corporation, Los Angeles, USA) were taken. Again, erythrocyte sedimentation rate (ESR) was measured using the Sediplast system (LP Italiana Spa, Milan, Italy); Diagnostic Products Corporation, Los Angeles, USA); complete blood counts (CBC) were performed using Sysmex KX-21 Hematology Analyzer (Sysmex Corporation, Kobe, Japan) were run on venous blood samples. The WHO criteria for anaemia (haemoglobin concentration b11 g/dL) 28 were used in this study. Also, urine and stool samples using iodine were obtained to determine the presence of pathogens in the intestines of study participants.
Raw data for the study were first entered into SPSS version 21 and then imported into STATA version 20 statistical package for analysis. Descriptive statistics in the form of standard deviation, means, and percentages were carried out using tables. Again, the binary logistic regression analysis was to evaluate the difference in anaemia prevalence in relation to the relevant variables. To assess the strength of association and statistical significance in bivariate analysis, odds ratio and 95% CI for odds ratio were calculated to determine their significant levels.
Results
Characteristics of Study Participants
Sociodemographic characteristics of pregnant women on anaemia prevalence (n = 220).

Prevalence of anaemia in relation to dietary habit, ANC follow-up and nutrient supplementation during pregnancy (n = 220).

Prevalence and Predictors Among Study Respondents
The distribution of morphologic type of anaemia among respondents.
Multivariate analysis of risk factors for anaemia using stepwise algorithm.

Logistic regression analysis of factors influencing anaemia in pregnancy.

Discussion
The general prevalence of anaemia in this study was 11.4%, and aligns with the multiple indicator cluster survey, 8 conducted in Ghana. Our findings discovered that the intake of food supplements (iron, folic acid, multivitamins) by pregnant women helped reduce anaemia (Table 6), and facilitated growth and proper development of both the pregnant mother and the foetus.1,3,4 Thus, the supplementation of iron sulphate, folic acid and other food supplements, and ANC follow-up during current pregnancy of participants significantly reduced the prevalence of anaemia as compared to those who did not take these supplementations.4,1 4 This study revealed anaemia and iron difficiency prevalence of 11.4% and 8.6%, respectively among study respondents. These are considerably lower than most of those previously reported including that of Nybo et al. 29 being 20.0%. Again, Thirukkane and Zahara 30 reported anaemia prevalence of 42.3%, and Aikawa et al. 22 reported anaemia prevalence as 43.2%. In a related study in Ghana, Lassey et al. 31 reported 56% of urban pregnant women in Ghana had haemoglobin levels below the 11 g/dL threshold while that of Mockenhaupt et al. 32 revealed the prevalence of anaemia and iron deficiency as 54% and 46% respectively among 540 rural pregnant women. Again, the findings of this study are in agreement with the work of Engmann et al. 14 which reported anaemia and iron deficiency among Ghanaian pregnant women from urban areas as 34% and 7.5, respectively. The possible reason for the low rates in anaemia and iron-deficiency anaemia among pregnant women in the present study could be due to the progressive improvement of ANC services alongside the focused ANC adopted by the Kwabre East Municipal health directorate.
The variations in anaemia prevalence among these studies could also be attributed to the differences in broader health systems and health responses targeted at the well-being of pregnant women. The difference in anaemia prevalence in the current study could further be attributed to improvement in the standard of living, with personal hygiene and the planned initiative of the government of Ghana to meet the sustainable development goal 3 by 2030. In studies by Mockenhaupt et al. 32 and Akowuah et al. 33 it was found that the Ghana health service has instituted focused ANC, maternal healthcare component, which enables individual pregnant mothers to receive health care from a particular health staff in the entire period of pregnancy. The findings indicate that the predictors of anaemia among pregnant women are iron sulphate, low use of ANC during pregnancy, large household size and folic acid. This supports observations from Ghana,8,13,34 Tanzania 7 and Nicaragua 17 which revealed that older pregnant women are more susceptible to be anaemic compared to their younger counterparts. In addition, a comparative study between Indonesia and Ghana by Mocking et al. 35 revealed similar study outcomes.
In the study, logistic regression analysis indicated that age was a key predictor of anaemia among pregnant women with beta co-efficient and z statistic of 1.44 and 8.27, respectively. This observation is in agreement with Melku et al.
20
who in their work in Gondar, Northwest Ethiopia, found that older pregnant women were more prone to anaemia than their younger counterparts. Possible reason for age as a predictor of maternal anaemia might be due to the poor feeding pattern of older pregnant women and the experience on safe multiple pregnancies, which do not make most of them attend ANC at early stages of pregnancy. The study demonstrated that mothers who have family size of more than
Additionally, the study findings revealed that the choice of facility, mothers’ satisfaction, attitude of caregivers and quality of service were in their various degrees of significance (Table 6). The study outcomes realised that the full utilisation of ANC helps to decrease anaemia prevalence among pregnant mothers under the 2015 WHO anaemia prevention and control guidelines 1 due to the immense education received. 36 Hence, the Pearson chi-square statistic for mothers’ satisfaction (data not shown) was highly significant at 1 percent. Thus, the above observation is in agreement with the study of Akowuah et al. 2018 and d'Ambruoso et al. 200533,37 in Ghana which concluded that the satisfaction of maternal health care services significantly influenced the degree at which pregnant mothers utilised ANC services. Furthermore, the Pearson chi-square statistics on attitude of caregivers and quality of service received by pregnant women (data not shown) in addition to the multiple regression analysis were significant in the study results. These findings are in agreement with the studies of.38,39 However, the findings of Al-Mehaisen et al.
Limitations of the Study
One of the limitations of this study is that the number of pregnancies and childbirths of respondents in relation to history of anaemia prevalence was not enquired. Again, the study could not determine which of the predictors preceded the other because of the cross-sectional study design used. The final limitation of the study was the exclusion of both tertiary and primary health facilities as the study was executed in secondary care facilities that were in primarily urban centres.
Conclusion
The study reports a relatively low prevalence of anaemia and iron deficiency among pregnant women in urban Ghana compared to those previously reported. The focused ANC organised by the Municipal Health Directorate for pregnant women could be among the reasons for the low prevalence. In terms of morphological types of anaemia, the predominant types reported by the study were normocytic normochromic, microcytic hypochromic and macrocytic normochromic. The main predictors of maternal anaemia were age of pregnant women, household size, ANC follow-up during pregnancy, folic acid intake in present pregnancy and sleeping under ITNs. In order to control the prevalence of anaemia and iron deficiency, the broader healthcare system is encouraged to make available folic acid in facilities and pregnant women must be encouraged to take more folic acid in addition to fruits at all times especially during pregnancy. Intense education on the need to fully utilise ANC must be strengthened to ensure early detection of potential pregnancy-related complications. Again, education on maternal health promotion should include sleeping under insecticide treated bed nets. In addition, programmes and policies aimed at reducing anaemia in pregnancy should target mothers with large household sizes since such families tend to be financially handicapped.
Footnotes
Acknowledgements
The authors wholeheartedly thank all laboratory staff who sincerely helped to collect data sample in the running of laboratory analysis. The authors are also grateful to the midwives and the pregnant women for their voluntary participation in the study. Lastly, we would like to thank the Kwabre East Municipal Health Directorate for both personnel and logistic support.
Authors' contributions
AJA is the principal investigator of the study and participated in its conception and design. AJA and EOA carried out the literature review and drafted the entire manuscript. AJA, EOA and AOA participated in data collection and were involved in the analysis. EOA meticulously reviewed the manuscript. All authors read and finally approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All data supporting findings are available upon request