
Abstract
Recent studies have highlighted relationship of allergic diseases with vitamin D deficiency. The aim of the study was to evaluate the impact of maternal vitamin D levels in pregnancy on the formation of atopic dermatitis in early life. A total of 186 pregnant women and their infants who developed atopic dermatitis before the age of 2 years were involved in the prospective study. Most pregnant women (57.5%) were diagnosed with 25(OH)D deficiency (3.6 ± 4.4 ng/ml) (P = .000). Maternal 25(OH)D deficiency was directly related to atopic family anamnesis and relatively high IgE levels. In these cases, children developed atopic dermatitis before the age of 6 months (70.8%) with prevalence of moderate-severity (55%) and persistent course (68.3%) of the disease. The above mentioned supported the idea that the peculiarities of the formation of atopic dermatitis in young children are associated with low concentrations of vitamin D in mothers during pregnancy.
Introduction
Among other factors responsible for the increased prevalence of atopic dermatitis (AD) over the last few decades, the role of vitamin D has been attached a special significance. Since the complex interaction of the epidermal barrier dysfunction and the immune response in the pathogenesis of atopic dermatitis, is of great importance, and vitamin D is involved in both processes, it is reasonable to suppose that vitamin D status determines the risk or severity of atopic dermatitis. Such correlation is indicated by experimental and epidemiological data. 9 The biological action of vitamin D goes farther than maintaining calcium homeostasis, it has an immunomodulatory effect on both innate and adaptive immune system. Vitamin D receptors (VDRs) display a wide range of effects on immune cells (macrophages, T and B lymphocytes). Their activation leads to suppression of dendritic cells, activation of Th2 cell responses, and reduction of Th1 cell responses tilting the balance towards the production of anti-inflammatory cytokines. The effect of vitamin D on the degree of differentiation of Th1 and Th2 cells has also been determined. 20
Despite the widespread use of prenatal multivitamin complexes, vitamin D deficiency is common in pregnancy and lactation.15,21 According to the literature data available, 50%-86% of pregnant women appeared to have low vitamin D levels, the lack, and deficiency of which is especially common among the mid-latitude zone population. 5 Moreover, it was found that 25(OH)D is easily transmitted from mother to fetus and is involved in the process of embryogenesis, ensuring and regulating normal fetal growth and development, the formation of the skeletal system, the proliferation of endothelial cells, lymphocytes, skin and dendritic cells, controlling synthesis of certain placental hormones. 8
Vitamin D metabolism during pregnancy, characterized with a number of peculiarities, is stipulated by placental role in transport and metabolic processes. Placenta formation at 4 weeks of gestation ensures the transfer of 25(OH)D to the fetus, allowing its concentrations in fetal blood to reach 87% that of the mother’s concentrations. Vitamin D deficiency during pregnancy predictably determines a low vitamin D status of the child.10,11 Vitamin D levels in pregnant women are directly related to the anthropometric data in children, affect the formation of innate immunity, determining the development of chronic diseases, both in infancy and later in life.1,12
The role of vitamin D in pregnancy is of great interest since the study suggested that a low level of 25(OH)D in blood serum is a risk factor for maternal and fetal health. 14 Vitamin D deficiency in young children is associated with a high risk for developing type 1 diabetes, cardiovascular system disorders/pathologies, autoimmune diseases, obesity, oncological pathology, psoriasis, atopic diseases (asthma, allergic rhinitis, atopic dermatitis), and inflammatory bowel diseases (ulcerative colitis, Crohn’s disease).4,19 The studies demonstrated that the prevalence of atopic dermatitis (AD) was higher in children born from mothers with low fish or vitamin D intake during pregnancy.16,24 Bäck et al 2 showed that high intake of Vitamin D during the first year of life correlates with increased risk of atopic dermatitis at 6 years of age. Currently, there predominate the articles where an inverse relationship between vitamin D levels and the prevalence and severity of atopic dermatitis were highlighted. There is evidence that vitamin D deficiency at birth is associated with a higher risk of developing atopic dermatitis. 13 The mutually exclusive nature of the data available determines the necessity for the continuation of studies in this direction.
The aim of the study was to evaluate the effect of vitamin D levels in pregnant women on development of atopic dermatitis in infants at extremely early age.
Materials and Methods
A prospective study was conducted on the basis of K.Chachava S/R Institute of Perinatal Medicine, Obstetrics and Gynecology. A total of 186 pregnant women and their newborn babies have been examined. Observation of pregnant women was carried out throughout the entire period of pregnancy until delivery, while for newborns up to 2 years, by providing visits at the age of 6, 9, 12, and 24 months, respectively. A total of 120 children who developed atopic dermatitis at the age of 2 years were involved in the study population, and 66 children with no clinical signs of atopic dermatitis or allergic family history formed a comparable control group.
The study protocol was approved by the Research Ethics Committee.
The study inclusion criteria: physician-confirmed diagnosis of atopic dermatitis, presence of typical skin lesions and informed consent of the parent for study participation.
The study exclusion criteria: atypical course of the disease, congenital (developmental) anomalies, hereditary diseases, concomitant acute somatic pathology.
The diagnosis of atopic dermatitis was verified through the criteria defined by Hanifin et Rajka while the severity of disease was scored by using the SCORAD index, respectively. The mother-child couple questionnaire included: maternal demographic, social and clinical data, detailed family history of atopy, child anthropometric data, diet/dietary pattern, AD course peculiarities, concomitant allergic reactions, and etc. The venous-blood serum 25-hydroxyvitamin D concentrations (25[OH]D) in pregnant women were determined by the electrochemiluminescence binding assay (ECL) (apparatus: COBAS e411; manufacturer ROCHE). Venous blood test was done at 14-16 weeks of gestation. IgE levels were determined in the peripheral blood of pregnant women. According to the recommendations proposed by the International Society of Endocrinology, 6 vitamin D concentrations were estimated by using the following criteria: <20.0 ng/ml—deficiency, 20.0-29.0 ng/ml—insufficiency, and >30.0 ng/ml—normal supply. For providing the statistical analysis of the results obtained, the software packages—Microsoft Excel 2010 and SPSS/v18 have been used. The arithmetic mean and standard deviation (SD) were defined as the parametric data. The median, quartiles, and interquartile range (IQR) were defined for 25(OH)D level as well. The probability value—P < .05 was taken as the lower confidence limit.
The Study Results
The data of the studied pregnant women are presented in Table 1.
Social-Demographic and Clinical Characteristics of Pregnant Women.

The selective analysis showed that the average age of pregnant women does not differ significantly, ethnic Georgian mothers, 25-34 of age, with higher education in most cases, prevailed in both groups. Low income indicators were almost equal, and poor living conditions were more common in the main group (P = .007). In both groups, the majority were first-time mothers (49.2% and 50.8%, respectively). The frequency of cesarean section with indication prevailed in the study group (39.2% and 27.3%).
59 mothers (49.2%) out of 120 pregnant women whose children developed atopic dermatitis at early age, had atopic family anamnesis. The average age at disease onset was 11.8 ± 5.5 years. In most cases atopic dermatitis was accompanied by other allergic reactions, a number of cases of atopy reported by fathers (Figure 1). They were regularly treated with hormonal (30.5%) and antihistamine (79.7%) preparations.

Parental atopy in the studied contingent.
The gestational age, gender profile and anthropometric data of the children did not differ significantly in the reference/compared groups, the early neonatal period passed without any physiological changes, on the fourth-fifth day all newborns were discharged home. Anthropometric and medical characteristics of children are given below in Table 2.
Basic Characteristics of Infants with Atopic Dermatitis (n = 120).
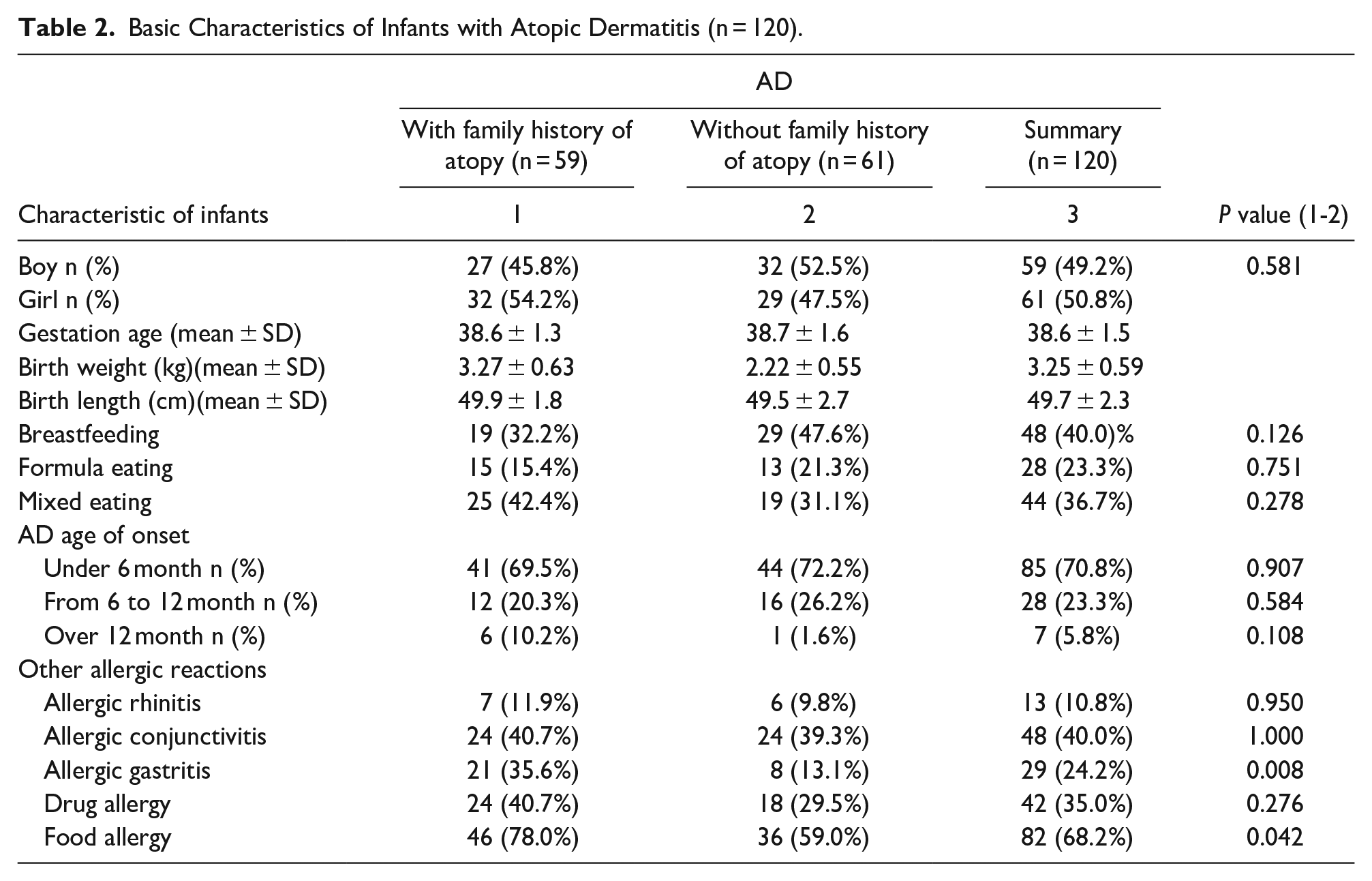
48 children were breast-fed (40.0%), 44 mixed-fed (breast milk/formula) (36.7%). In most cases the debut of atopic dermatitis was <6 months of age (70.8%). Of the other manifestations of atopy, special attention should be paid to allergic gastritis, and prevalence of food allergies, in case of hereditary loaded anamnesis with allergic diseases. The rate of vitamin D normal supply, insufficiency and deficiency in the pregnant population is given in Table 3.
Frequency of 25(OH)D Normal, Insufficiency and Deficiency in Pregnant Women (n = 186).

According to the results obtained, normal supply of 25(OH)D was fixed in 12.5%, insufficiency—in 30%, and deficiency in 57.5% (13.6 ± 4.4 ng/ml)of mothers of children with AD, respectively.
Vitamin D (25[OH]D) deficiency during pregnancy prevailed in both cases: with hereditary anamnesis of atopy (62.7%) and without it (52.5%) and was reliably more common among the mothers of children with AD, compared with control groups (OR -5.51, 95% CI 2.58–11.9, P = 0.000). In mothers of children with AD, summary average value of 25(OH)D was lower (19.7 ± 8.5) than the one in the control group (26.3 ± 8.2) indicating the vitamin D deficiency in pregnant women (Figure 2).
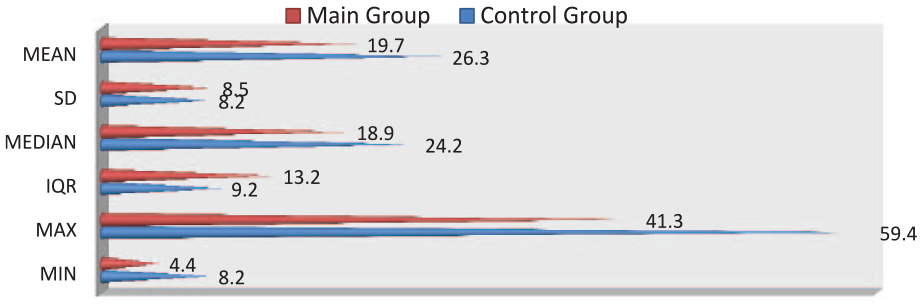
Quantitative indicators of maternal 25(OH)D concentration (n = 186).
In the study group of pregnant women, the median level of serum 25(OH)D was 18.9 ng/ml and the interquartile range (IQR)—13.2, respectively. The median level of 25(OH)D in pregnant women with atopy was 18.7 (IQR—8.9) and without atopy—18.9 (IQR—16.3), respectively. As for the control group, where atopy was not observed in either pregnant women or children, the median level of serum 25(OH)D was 24.2 ng/ml and the interquartile range—9.6.
Investigation of IgE concentrations in the peripheral blood of pregnant women revealed an increase in IgE levels in 62.7% of mothers with atopy (37 pregnant women) and in 24.6%—without atopy (15 cases) (OR—5.15, 95% CI 2.19-12.28, P = .000). Quantitative changes in IgE concentrations are given in Table 4.
Quantitative Indicators of Maternal IgE Concentration in Pregnant Women (n = 120).
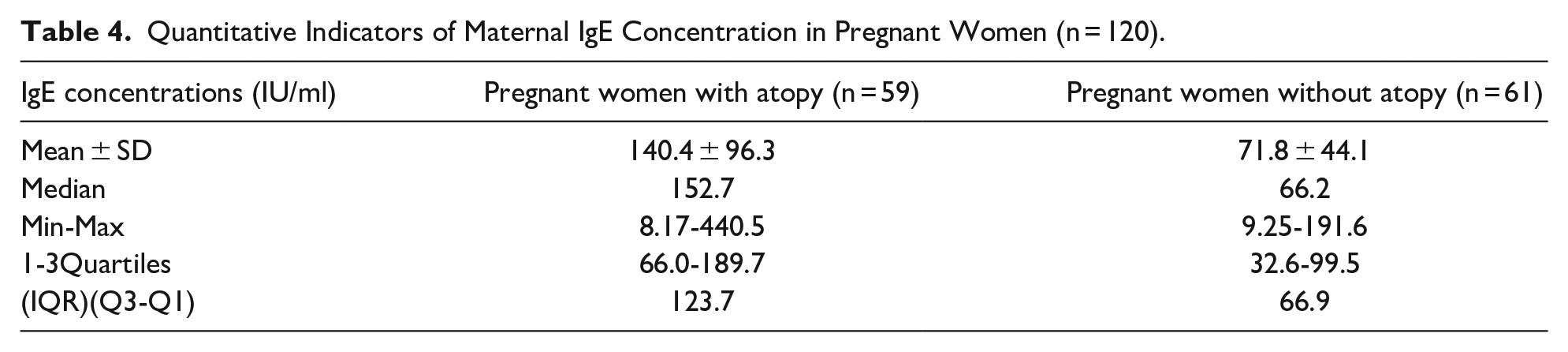
The median level of IgE in atopic mothers was 152.7 IU/ml (IQR—123.7) that is 2.5 times higher than the indicator obtained in pregnant women without atopy (66.2 IU/ml, IQR—66.9). The serum 25(OH)D concentrations in atopic mothers with elevated IgE levels was 18.6 ± 9.1 ng/ml. The association of 25(OH)D concentration in pregnant women with the peculiarities of AD course in children has been studied. Age at disease onset, assessment of the AD severity according to SCORAD index, the nature of disease course were taken into account (Table 5).
Association of Maternal 25(OH)D Level with AD Course in Children.

According to the data obtained, at 25(OH)D deficiency in pregnant women, atopic dermatitis developed in 70.8% of children <6 months of age; according to the SCORAD index, the moderate course of the disease prevailed in both groups with hereditary atopy (54.2%) and without it (55.7%). The prevalence of AD persistent course (68.3%) against the background of 25(OH)D deficiency is of great significance.
Discussion
A number of studies focused on evaluating the effects of vitamin D levels on the prevalence and the course of atopic dermatitis showed that 25(OH)D level was higher in patients with mild course of AD compared with patients with moderate to severe AD. 16 Recent studies have revealed associations of allergic diseases with vitamin D deficiency. 21
There are epidemiological data that vitamin D deficiency during pregnancy increases the risk of developing allergic diseases including atopic dermatitis, food allergies, asthma and allergic rhinitis in children. However, the immunological mechanisms of this effect are not yet clear. 15 Miyake et al 16 suggested that high concentrations of umbilical cord blood vitamin D serve as protective mechanisms against the development of atopic dermatitis (AD), wheezing, and upper respiratory tract infections. The above-mentioned does not apply to asthma and allergic rhinitis. 3 As for the role of vitamin D in the development of asthma and atopic dermatitis, presumably, the majority of immune cells are vitamin D receptors and there is evidence of genetic linkage of these receptors with asthma.17,18
Deficiency of 25(OH)D in pregnant women showed a trend to increase that was confirmed by the following data—57.5% of the studied women had 25(OH)D deficiency (13.6 ± 4.4 ng/ml) in both cases—hereditary load with atopy, and without it, during pregnancy. In addition, the 25(OH)D value was significantly different from those of conditionally healthy pregnant women (OR—5.51, 95% CI 2.58-11.9, P = .000). It should also be noted that the presence of atopy in mothers did not significantly change the situation.
The study results have revealed that atopic dermatitis in mothers with 25(OH)D deficiency is characterized by a relatively high incidence rate, early-age onset, and persistent-moderate course, indicating the association between vitamin D deficiency in pregnant and clinical features of atopic dermatitis (AD) in children. Similar results were suggested by Vestita M and Wang S.22,23 In addition, it should be emphasized that maternal 25(OH)D deficiency was directly associated with the family atopic history and relatively high IgE levels, having been consistent with literature data, according to which relatively high IgE level at atopia correlates with a low level of blood serum vitamin D. 7 More research is required to assess the role/status of vitamin D in development of atopic pathology among the pediatric population taking into account genetic and environmental factors.
Conclusion
Based on the results obtained, atopic hereditary predisposition (hereditary load) and vitamin D deficiency in pregnant women cause prognostic discrimination in terms of AD formation in early childhood. Detecting vitamin D levels in pregnant women can be applied as predictive criteria for the interpretation of formation, progression and severity of atopic dermatitis. According to the above-mentioned, a wide-scale study regarding to the correction of vitamin D deficiency in pregnant women can be considered as an important preventive measure for atopic dermatitis in young children.
Supplemental Material
sj-pdf-1-gph-10.1177_2333794X211022916 – Supplemental material for Impact of Maternal Vitamin D Status on the Formation of Atopic Dermatitis in Young Children
Supplemental material, sj-pdf-1-gph-10.1177_2333794X211022916 for Impact of Maternal Vitamin D Status on the Formation of Atopic Dermatitis in Young Children by Mariam Petriashvili in Global Pediatric Health
Footnotes
Author Contributions
Mariam Petriashvili is the only responsible and corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.