
Abstract
Background
Physical activity is associated with a reduced risk of several adverse obstetric outcomes, including preterm birth, gestational diabetes, and preeclampsia, anxiety, and depression. However, the majority of women do not achieve recommended levels of physical activity in either time or intensity. It was less known among pregnant women in Ethiopia. This study assesses the knowledge, attitude, and practice of physical activity among pregnant women attending antenatal care in Harari regional state, eastern Ethiopia from December 15, 2023 to January 15, 2024.
Methods
An institution-based cross-sectional study was conducted among 435 participants. A random sampling method was deployed to select study participants. A pretested and structured questionnaire was used to collect the data through a face-to-face interview. Data were entered into EpiData version 3.1 and analyzed using SPSS 26.0 software. Binary logistic regression was used to identify factors associated with physical activity practice. Adjusted odds ratio (AOR) with a 95% confidence interval was used to report the association, and statistical significance was declared at p-value < 0.05.
Results
The findings indicate that 50.1% (95% CI: 45.5–54.9%) of pregnant women were practice physical activity. Women attending health centers (AOR = 2.81, 95% CI: 1.85–4.26), aged 25–34 years (AOR = 1.94, 95% CI: 1.25–3.02), urban residence (AOR = 1.85, 95% CI: 1.17–2.91), and women with good perceived benefits (AOR = 4.78, 95% CI: 3.12–7.31) were significantly associated with physical activity.
Conclusion
The findings reveal that half of the study participants practice physical activity. Attending health centers, the age of women, residence, and positive perception of the benefit of physical activity were significantly associated with physical activity. Nurse practitioners should educate women about the benefits of regular physical activity and help them overcome the barriers to achieving recommended physical activity levels to improve perinatal outcomes.
Introduction
Physical activity (PA) is defined as bodily movement produced by skeletal muscles that results in energy expenditure (Harris et al., 2024). PA is believed to be essential to healthy pregnancy. Physical inactivity is a major risk factor of pregnancy complication (Dishman et al., 2021) and early death during pregnancy (Jones et al., 2021). Pregnant women who are physically inactive is at risk of gestational diabetes mellitus (GDM) (Xie et al., 2024), preeclampsia, gestational weight gain, labor and birth complication, and back pain (Gascoigne et al., 2023; Hailu et al., 2025). Besides, sedentary lifestyle raises the risk of perinatal depression (Garland, 2017). Globally, thousands of pregnant women pass away due to these risks and other immeasurable and preventable complications of pregnancy (Ferrari & Joisten, 2021; Silva-Jose et al., 2022). Maternal mortality ratio (MMR) is about 216 per hundred thousand in the world, and 546 in Sub-Saharan Africa (SSA) (Okwan & Kovacs, 2020). Ethiopia is one of the SSA with a high MMR, approximately 412 per hundred thousand (Harris et al., 2024). Health promotion and physical exercise is a vital activity to avoid pregnancy complication and death(Say et al., 2014).
The American College of Obstetricians and Gynecologists (ACOG) recommended that aerobic physical activity(PA) reduces weight gain and risk of gestational pregnancy diabetes by 25% in pregnancy (DiPietro et al., 2019). Physical activity during pregnancy mitigates the risks of large newborns, operative and instrumental deliveries, low back pain, perinatal depression, and cesarean section (CS) by 15% and coping with labor pain(Domenjoz et al., 2014).
Literature Review
Physical activity can reduce the risk of pregnancy-related illnesses such as depression by at least 25% and the risk of developing gestational diabetes, high blood pressure, and preeclampsia by 40%(Cilar Budler & Budler, 2022). According to the study in India, a sedentary lifestyle was a major risk factor for 50% of cesarean deliveries (Janakiraman et al., 2024). The systematic review randomized controlled trial reported that physical inactivity increases the risk of preeclampsia by 30–33% (Downs et al., 2012). Despite the benefits of PA, some pregnant women and clinicians are concerned that regular PA causes fetal risks even though the studies showing vigorous PA under dehydration (Kracht et al., 2024), in the supine position, and motionless posture (Okafor & Goon, 2020).
A global systematic review shows that a total of 59.09% of the studies indicated that participants had a low level of physical activity during pregnancy (Silva-Jose et al., 2022). Evidence shows that around 40% of pregnant women felt that they had the opportunity to be active, and fewer than 50% of women felt that they were able to be physically active (Kracht et al., 2024). In addition, a pooled systematic review shows that only 13.3% of pregnant women meet physical activity recommended by ACOG suggest that pregnant women should be exercise an average of 20 to 30 min a day (Rodrigues-Denize et al., 2024). A cross-sectional study carried out in São Paulo in southeastern of Brazil show that the prevalence of physical activity among pregnant women was 20.1% (Nascimento et al., 2015). In Africa, evidence shows that the practice of pregnancy physical activity (PPA) was low, mainly due to poor knowledge and awareness of its benefits (Maruf et al., 2017; Mukona et al., 2016; Santo et al., 2017).
However, study showed in southwest Ethiopia around 46% of pregnant women were physically active during pregnancy (Golan, 2022). The other study from southwest Ethiopia reported that 76.4% of pregnant women were physically inactive (Hailemariam et al., 2020). Moreover, study done among pregnant women attending antenatal care at public and private health facilities in Mekelle Ethiopia, 79.3% were classified as sedentary lifestyle (Hailemariam et al., 2020). While research confirms the health benefits and safety of engaging in physical activity throughout pregnancy for both mother and baby, there is limited knowledge about the physical activity practices among pregnant women in Ethiopia. Therefore, this study aimed to assess the practice of physical activity and its associated factors among pregnant women attending antenatal care in public health facilities of Harari Regional State, Eastern Ethiopia.
Materials
Study Area and Period
This study was conducted in Harari region's Public Health Facilities, in Eastern Ethiopia. Harari Region is 516 km east of Addis Ababa, the capital city of Ethiopia. The region has a total of nine districts (3 rural and 6 urban) with 36 kebeles (19 urban and 17 rural kebeles), which is the smallest administrative unit. Based on the 2022 national population census projection, the region has an estimated total population of 276,000. Out of these, about 137,000 were females and 139,000 were males, 72,525 households, and 8740 pregnant women. In 2022, the region had 42 public health facilities (2 hospitals, 8 health centers, and 32 health posts) (Shama et al., 2021). This study was conducted from December 15, 2023 to January 15, 2024.
Study Design and Population
An institution-based cross-sectional study design was employed among pregnant women attending ANC in selected public health facilities of the Harari region in eastern Ethiopia. All pregnant women age 18 year and above were included in the study, however, pregnant women with medical complications or contraindications such as pre-eclampsia, severe anemia, cardiovascular diseases, and women with injuries that limit mobility, and severe mental health conditions that could impede physical activity were excluded.
Sample Size Determination and Procedure
A sample size of 435 persons were computed by Epi-Info version 7.2 using single population proportion formulas. Accordingly, the proportion of physical activity was considered from a previous study conducted in northern Ethiopia (57.9%) (Gebregziabher et al., 2019) with the assumptions of a confidence interval of 95%, a margin of error of 5%, and a 10% response rate. Finally, a sample size of 435 persons was calculated. The sampling procedure was first the facilities in the region were stratified based on urban and rural health facilities and then, four out of seven urban health centers, one out of two public hospitals, and two out of four rural health centers were randomly selected by a lottery method. Then, estimated sample sizes were proportionally allocated to each sampled facility using the total pregnant women attending antenatal care monthly in that facility that reviewed from December 15, 2023, to January 15, 2024, updated HIS registry available at each facility. Then, a separate sampling frame was prepared in each health facility and finally, eligible participants were recruited and invited to study using a systematic sampling technique.
Data Collection Methods
Data were collected using pretested structured questionnaires adapted from standardized pregnancy physical activity questionnaire(PPA) (Chasan-Taber et al., 2004).The PPAQ measures the frequency and duration of activities and gives an intensity value to each activity. The questionnaire contains socio-demographic characteristics, reproductive and medical variables, knowledge, attitude and perception-related factors, and physical activity. A structured face-to-face interviewer-administered questionnaire was used to measure physical activity. It contains a total of 31 activities/items grouped into four themes: household activities, occupational, sports/exercise and transportation, and sedentary activities. Pregnant women were asked the amount of time spent on an activity per day/per week during pregnancy for each activity which ranged from zero to seven days per week. Physical activities were categorized based on the domains (i.e., household, occupation, sport, and sedentary). Initially, the instrument was developed in English language and then translated into Afan Oromo and Amharic language and back-translated to English to check its consistency. Six midwives with bachelor's degree data collectors and one master public health supervisor who fluently speaks Amharic and Afan Oromo languages were recruited based on their previous similar exposure. Data were collected through face-to-face interviews using a standardized pregnancy physical activity questionnaire. A Pre-test was conducted on 5% of the sample size in a separate facility of the region that was not selected. During pre-testing, the inconsistency was corrected to reduce the problems encountered while filling out the questionnaire, and revision was incorporated into the final questionnaire. The participants were interviewed in a quiet separate area in/around the facility after explaining the purpose of data collection.
Dependent Variable
Practice of physical activity
Independent Variables
Sociodemographic factors: age, marital status, residence, education level, occupation and average monthly income. Reproductive factors are type of facility where ANC attended, pregnancy intention, gravidity, parity and abortion. In addition knowledge, attitude and perception, awareness, perceived benefits and barriers were included in the study.
Data Collection Methods
The level of physical activity during pregnancy was measured using 31 items/questions. These items captured details on the frequency, duration, and intensity of various physical activities across the four domains: household/caregiving, occupational, leisure, and sedentary activities. The total physical activity was calculated as the sum of (duration * intensity) for each question. Each activity was classified according to intensity in Metabolic Equivalent Task (MET) sedentary (< 1.5 MET), low (1.5 to < 3.0 MET), moderate (3.0 to 6.0 MET), and vigorous-intensity (> 6.0 MET), and the type of labor, domestic (e.g., caring for a person), and sports/exercise (Chasan-Taber et al., 2004). Pregnant women were asked to select the best estimating amount of time spent on an activity per day/per week during pregnancy for each activity and the duration ranged from zero to seven days per week. The total activity was then quantified in MET minutes per week and categorized as “Good” and “Poor” activity based on the median. Participants with MET scores equal to or above the median were classified as having a “good” physical activity, while those with scores below the median were classified as having a “poor” physical activity. Based on this, we categorized individuals as good (≥ 60.36), or poor (< 60.36) (Bockler et al., 2021).
The attitude toward physical activity was measured using 6 items/questions with response options of “yes” and “no”. A response with a higher score indicates a positive attitude toward physical activity. A composite index score was calculated by sum-up the response of all items. Pregnant women who scored median and above composite score was classified as a good attitude, and those who score below the median were classified as a poor attitude toward physical activity (Ainsworth et al., 2011).
The perceived benefit of physical activity during pregnancy was assessed through 13 items designed to capture the participants’ beliefs about the positive outcomes of physical activity. Each item has a 5-point likert scale with response options ranging from “Strongly agree” to “Strongly disagree” to express the degree of their agreement (Okafor & Goon, 2021). Participant response was sum-up to form a composite score. Participants who scored the median and above were categorized as a good perceived benefit of physical activity, and those who scored below the median were categorized as a poor perceived benefit (Ainsworth et al., 2011).
Perceived barrier to physical activity was measured using 8 items that identify hinder to engage in physical activity during pregnancy. Each item was rated on a 5-point likert scale, with responses ranging from “Strongly agree” to “Strongly disagree”. A composite score was calculated by summing the score of all items, with higher scores indicating a greater perception of barriers to physical activity. Participants who score median and above were categorized as a good perceived barriers, and those who score below the median were considered to have a poor perceived barriers to physical activity during pregnancy (Sytsma et al., 2018).
Data Quality Control
Two days training was given for data collectors by principal investigator regarding how to select the participants, obtain informed consent, keep confidentiality and privacy of the study subjects and use the questionnaire. A pretest was conducted on 5% of the sample size in a separate non-selected facility two weeks prior to the actual data collection and amendments were made to the questionnaires prior to use the instrument. Principal investigator and supervisor checked filled questionnaire on daily before receiving it from each data collector and they randomly selected a filled questionnaire to cross check its completeness and errors on the spot. Overall supervision was carried out by the principal investigator on daily based.
Data Processing and Analyses
After the completeness and consistency of the data were checked the data was entered into EpiData version 3.1, and exported to SPSS version 26.0 for data cleaning and analysis. Multicollinearity was checked using the variance inflation factor (VIF) for independent variables. Bivariable and multivariable binary logistic regression analyses were done to identify factors associated with the practice of physical activity. Independent variables with a P-value < 0.25 in the bivariable analysis were considered for the multivariable analyses model. Adjusted odds ratio (AOR) with 95% CI was used to report association and the significance level was declared at P-value < 0.05.
Results
Socio-Demographic Characteristics
A total of 435 pregnant women participated in the study with a mean participant age of 26.1 (±4.6) years, and 54.5% of the participants in the age group of 25–34 years. More than half, 52.6% of the participants were urban residents, and 90.1% of the participants were married. Regarding educational status, about 41.4% of women were attending secondary school. About half, 51.3% of the participants were housewives. The median average monthly income of the participants’ family was 2800 Ethiopian birr with an inter-quartile range (IQR) of 2200 (Q1 = 1500, Q3 = 4700), which is lower than the current average monthly salary in Ethiopia (Table 1).
Sociodemographic Characteristics of Pregnant Women in Harari Regional State, Eastern Ethiopia, 2024 (N = 435).

Reproductive and Obstetric Characteristics
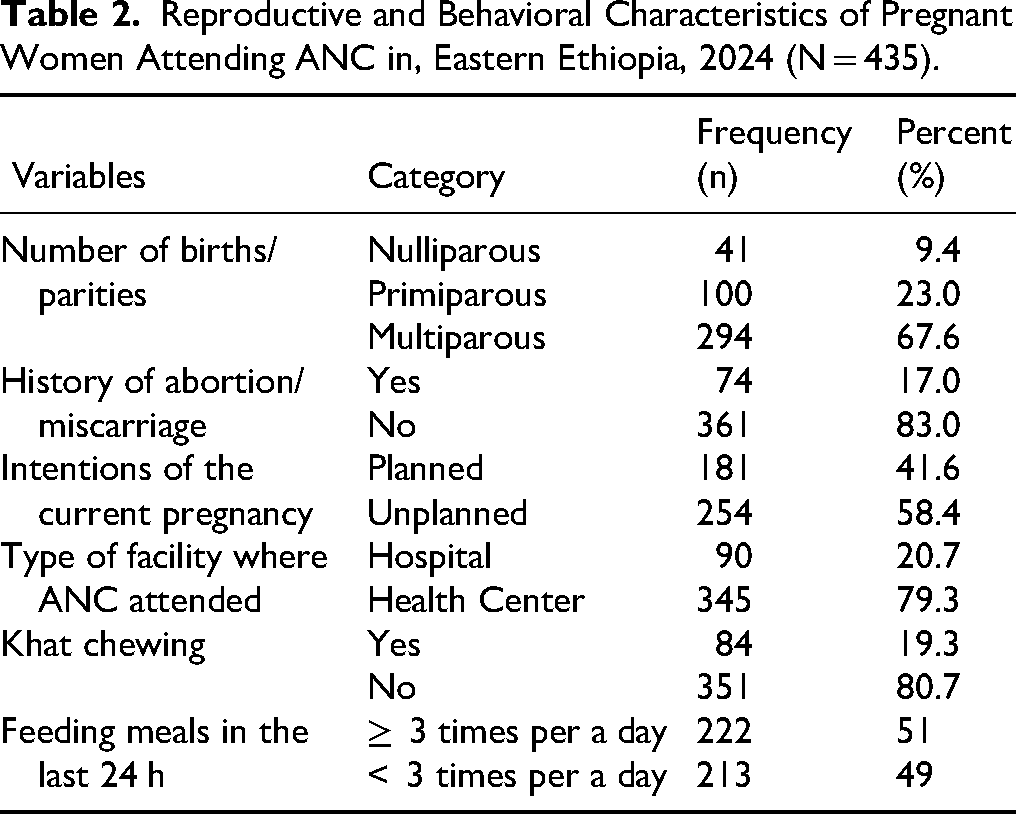
Regarding on the number of birth or parities, 9.4% of the participants were nulliparous and 67.6% of the participants were multigravida. The majority of pregnant women (83%) of the participants had no history of abortion/miscarriage, and less than half, 41.6% of the participants had plans for their current pregnancy, while about more than half, 58.4% were unplanned pregnancy. More than three-fourths, 79.3% of participants attended antenatal care at a health center during the current pregnancy. Around one out of five (19.3%) pregnant women were chewing Khat during the current pregnancy, and nearly half (49.0%) of the participants were feeding meals less than three times per day (in the last 24 h before data collection) during the current pregnancy (Table 2).
Reproductive and Behavioral Characteristics of Pregnant Women Attending ANC in, Eastern Ethiopia, 2024 (N = 435).
Knowledge, Attitude, and Perception Toward Physical Activity
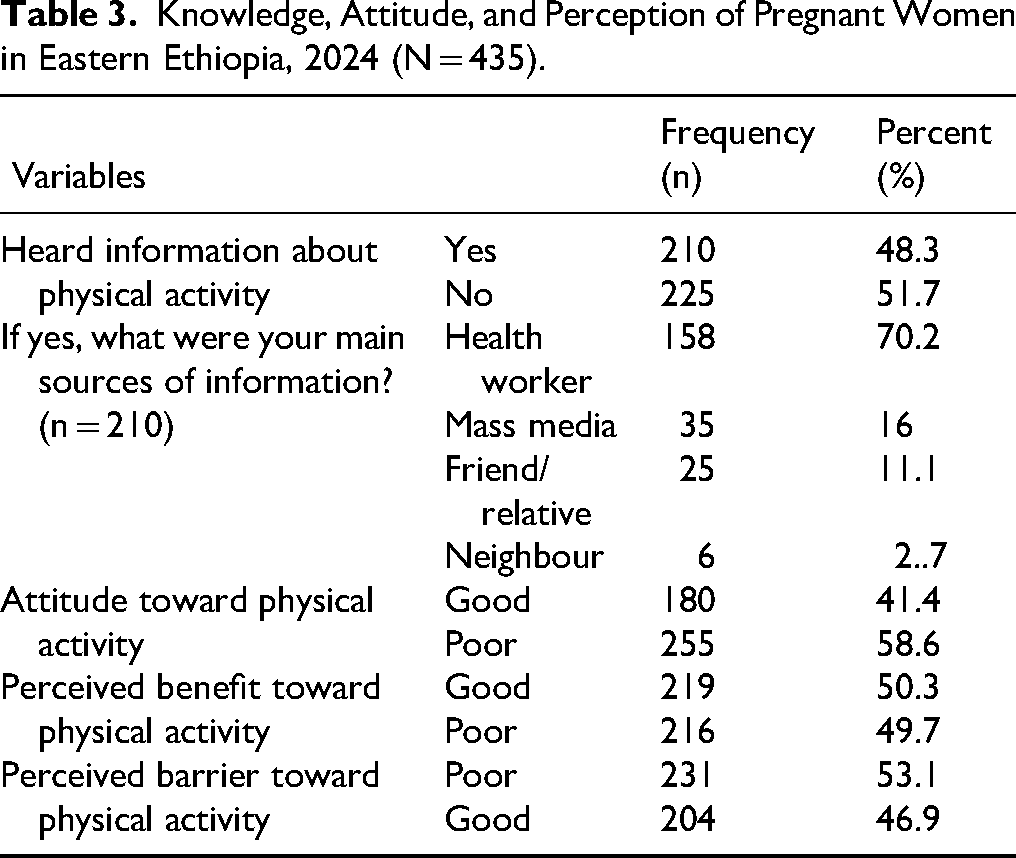
Above half (51.7%) of the study participants heard information about pregnancy physical activity, of those who heard information the majority (70.2%) heard from health workers followed by mass media (16%) as the main source of information. A significant proportion, 58.6% of the participants had poor attitudes toward physical activity. Half (50.3%) of participants had good perceived benefits toward physical activity, and 53.1% of the participants had lower perceived barriers toward pregnancy physical activity (Table 3).
Knowledge, Attitude, and Perception of Pregnant Women in Eastern Ethiopia, 2024 (N = 435).
Level of Physical Activity
The proportion of physical activity practice among pregnant women was 218 (50.1%, (95% CI: 45.5, 54.9%), and the median of overall physical activity score (MET) was 60.36 Hrs per week with an inter-quartile range of 57.17(Q1 = 38.1; Q3 = 95.2). Regarding the specific domain of physical activity, 50.1%, 49.0%, and 51.5% of the participants score household activities, occupational activities, and leisure-time physical activities, respectively. However, 70.6% of the participants experience light sedentary activities (Figure 1).

Level of Physical Activity Among Pregnant Women in Eastern Ethiopia, 2024 (N = 435).
Factors Associated with Level of Physical Activity
In the Bivariable analysis, age, education, residence, marital status, pregnancy intention, awareness and attitude toward physical activity, perceived benefit toward physical activity and perceived barriers toward physical activity were candidates at p-value < 0.25 (Table 4).
Bivariable Logistic Regression Associated with Physical Activity Among Pregnant Women in Eastern Ethiopia, 2024 (N = 435).
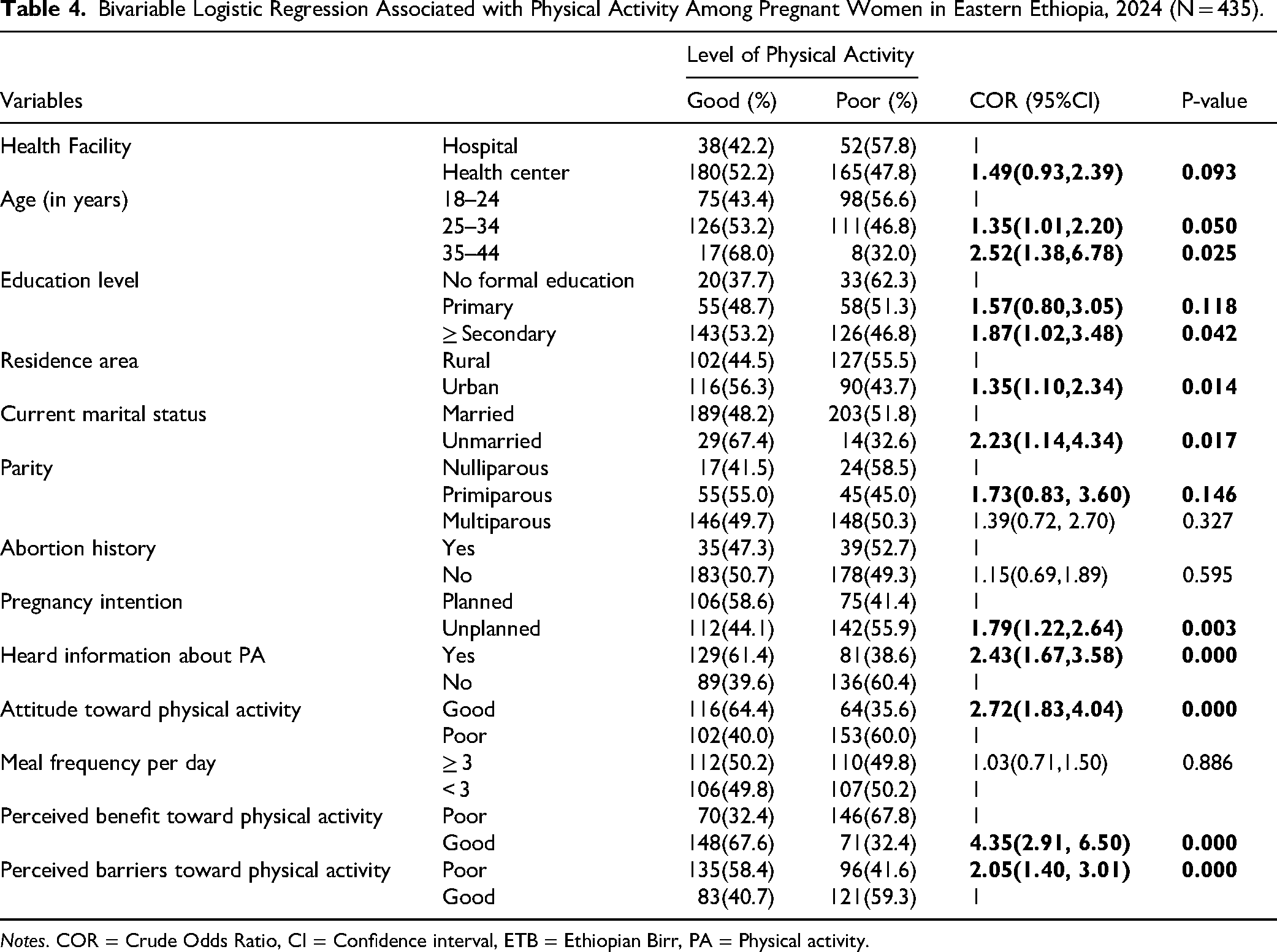
Notes. COR = Crude Odds Ratio, CI = Confidence interval, ETB = Ethiopian Birr, PA = Physical activity.
In the multivariable analysis, the odds of physical activity were nearly three times higher (AOR = 2.81, 95% CI: 1.53, 5.16) among pregnant women who attended ANC services at the health center compared to those who were attending ANC at the hospital. The odds of physical activity were two times higher (AOR = 1.94, 95% CI: 1.24, 3.02) among pregnant women in the age group of 25–34 years old compared to those aged 18–24. The odds of physical activity were 85% higher (AOR = 1.85, 95% CI: 1.12, 3.06) among pregnant women residing in the urban area compared to those residing in the rural area. The odds of physical activity were two times higher (AOR = 2.35, 95% CI: 1.13, 4.90) among pregnant women who were currently not living together/others compared to those who were currently living together/married. The odds of physical activity were nearly five times higher (AOR = 4.78, 95%CI: 3.08, 7.42) among pregnant women who had good perceived benefits toward physical activity compared to those who had poor perceived benefits toward pregnancy physical activity (Table 5).
Multivariable Logistic Regression of Factors Associated with Level of Physical Activity of Pregnant Women in Eastern Ethiopia, 2024 (N = 435).

Notes. AOR = Adjusted Odds Ratio, CI = Confidence interval, ETB = Ethiopian Bir.
Discussion
The study aimed to assess the practice of PA and its associated factors among pregnant women in the Harari region of eastern Ethiopia. The findings show that half of the study participants practiced PA during pregnant. Factors associated with PA were maternal age, marital status, attendance ANC at health center, place of residence, and beliefs about exercising during pregnancy.
The study reveals that the prevalence of physical activity among pregnant women was 50.1%, higher than a pooled meta-analysis (34%) in Ethiopia (Kasahun et al., 2023), Sidama (25.5%) Ethiopia (Belachew et al., 2023), Tigray (20.7–21.9%) Ethiopia (Belachew et al., 2023; Hailemariam et al., 2020), Dessie town (32.2%) Ethiopia (Yimer et al., 2024) in Karnataka state (40.3%) India (Janakiraman et al., 2024), urban Chinese women (11.1%) (Zhang et al., 2014). This may be the current study participants included from urban and governmental health institutions, and used a larger sample size than other studies. In addition, the study participants had good knowledge and a favorable attitude toward pregnant physical exercise during pregnancy. However, this study finding is lower than study in Nigeria (84.7%) (Ribeiro et al., 2022) and United Arab Emirates (75%) (AlBlooshi et al., 2023), and India (92.8%) (Ana et al., 2021). The discrepancy may be due to the variations in the sample, sociocultural characteristics, and measurement tools used. Additionally, since over half of the pregnant women in this study are housewives with low to middle income. They are less likely to outsource household tasks and other services, which could have contributed to low physical activity (Hoodbhoy et al., 2018). In Ethiopia due to the traditional culture, people assume that pregnancy is a vulnerable period that requires rest and protection, and the primary reason for not exercising during pregnancy is fear of miscarriage (Hailemariam et al., 2020).
Moreover, pregnant women are not allowed to implement a large amount of physical exercise demanding activities, such as cleaning and outdoor work. Sociocultural factors and misconceptions about physical activity during pregnancy may also contribute to the observed awareness gap. In some Ethiopian communities, traditional beliefs discourage physical activity during pregnancy due to perceived risks to maternal or fetal health, which may reduce women's likelihood of seeking or engaging in antenatal exercise (Tesfaye et al., 2020). Studies in east Africa highlight that cultural beliefs often shape maternal health behaviors, with certain communities perceiving exercise as harmful during pregnancy, potentially impacting the overall level of awareness around antenatal exercise. Low physical activity has been linked to increased risk of diabetes and cardiovascular diseases in pregnant women (Assah et al., 2009; Hjorth et al., 2012).
In this study, 51.6% of participants reported having heard about antenatal exercise, which is notably lower than South Africa (70.2%) (Okafor & Goon, 2021), and Ethiopia (56.3%) (Yimer et al., 2024). The differences observed in awareness levels are attributed to several factors, including health education policies, accessibility to healthcare services, and sociocultural influences across different regions. The awareness in South Africa (70.2%) was considerably higher than these findings. This difference could be partly explained by South Africa's ongoing health promotion initiatives, which focus specifically on maternal health, including the benefits of antenatal physical activity (Okafor & Goon, 2021). South Africa has invested in extensive health education campaigns about the benefits of regular exercise during pregnancy (Okafor & Goon, 2021). These initiatives largely urban-centered have proven effective at enhancing knowledge around maternal health practices, including antenatal exercise, especially where media exposure to health campaigns is greater.
In this study, almost 43.4% of the respondents were knowledgeable about pregnancy physical activity which is comparable with pooled meta-analysis (46%) in Ethiopia (Kasahun et al., 2023), but it is higher than the findings in Gondar (39.5%) Ethiopia (Janakiraman et al., 2021), in Baghdad city (39%) (Benyian, 2024), however, in contrast the fining of this study was lower than finding in Nigeria (52.4%) (Bockler et al., 2021)and Sidama Ethiopia (72.1%) (Belachew et al., 2023), Dessie Amhara Region Ethiopia (56.3%) (Yimer et al., 2024), Bhair Dar Ethiopia (55.8%) (Bayisa et al., 2022). The discrepancy might be due to the differences in time lag when the previous researches were conducted, educational background, sociocultural differences, and due to study populations difference (Yimer et al., 2024).
This study indicates that 70.6% of women are engaged in sedentary activities during the current pregnancy. This finding is consistent with previous research that highlights troublingly low physical activity among pregnant women, with 79.3% classified as sedentary (Hailemariam et al., 2020), but higher than a study conducted in Nigeria (49.0%) were sedentary(Adeniyi et al., 2014). Pooled meta-analysis shows that more than half of the participants, 58% of their time (range 57.1 to 78%) spent in sedentary activities during pregnancy impacted maternal or offspring outcomes (Fazzi et al., 2017).This finding highlights an important interventions on increasing physical activity among pregnant women.
The study shows that women attending a health center had 2.81 times higher odds of physical activity compared to those attending a hospital. This finding is in agreement with a study from Uganda that showed women attending antenatal services in primary care settings had higher physical activity levels due to routine health promotion activities (Bayisa et al., 2022). Similarly, a study in China showed that women visiting primary health facilities were more likely to receive counseling on physical activity, which increased their participation in physical exercise (Yimer et al., 2024). While another found that pregnant women attending ANC at health centers had more favorable perceptions of physical activity compared to those at tertiary hospitals in Nigeria (Emmanuel et al., 2024). These findings highlight that health care workers in the health center might be have more time to counsel maternal health care of pregnancies and births, therefore they are more experienced in maternal health care services-related matters.
Pregnant women aged 25–34 years were 1.94 times higher odds of physical activity compared to those aged 15–24. Similarly, study done in Nigeria found that older pregnant women (25–34) years had more engaged in physical activities due to greater awareness of health benefits and more motivation for maternal health (Adeniyi et al., 2014). This finding is also in line with a previous study in Dessie town and Mekelle, Ethiopia (Hailemariam et al., 2020; Yimer et al., 2024). This age group might be due to having a better educational level, good knowledge, and a better understanding of physical activity during pregnancy. Studies in western countries, like the United States have also reported that women aged 25–34 years tend to have higher levels of physical activity during pregnancy likely due to greater health literacy and access to health information (Downs et al., 2012).
This may be the result of the fact that pregnant women in this age group were more actively engaged in various types of physical activity and had better knowledge, attitudes, and comprehension of physical activity during pregnancy (Yimer et al., 2024). A possible reason might be pregnant women of younger ages in Ethiopia were more actively engaged in different household and occupational activities during pregnancy compared to older women. In Ethiopia, religious beliefs and culture have an impact on social values. Specifically, it is common to find within a single household that younger household members would be expected to manage any household or occupational activities as a sign of respect for older household members (Hailemariam et al., 2020).
The finding showed that women residing in urban areas had 1.85 times higher odds of physical activity than those in rural areas. This is in line with a study in Ethiopia that urban women had higher odds of maintaining physical activity during pregnancy compared to rural women (Hailemariam et al., 2020). Similarly, studies from Europe and North America reveal that urbanization positively correlates with activity levels due to better infrastructure and social support for physical activity. Reflects differences in infrastructure, availability of resources, and social support systems contribute favorable environment for physical activity. Urban environments typically offer superior walking condition and access to public recreational facilities, which are strongly associated with meeting recommended physical activity levels during pregnancy relative to rural settings. Conversely, rural areas often present barriers to facility access and lack of the social supports needed to engage in physical activity.
Additionally, this study found that pregnant women who were not living together had 2.35 times higher odds compared to those living together/married. This might be pregnant women who were not living together with her partner could be more active compared to those who were living together due to child care, and household duties and responsibility. This is consistent with study conducted in Tanzania found that unmarried women or those with alternative living arrangements had higher physical activity levels, potentially due to fewer household responsibilities or social expectations that can limit free time. A similar pattern was observed in Poland, where single women showed more independence in following physical activity routines, while married women reported challenges due to caregiving duties (Puciato & Rozpara, 2021). However, this study contradicts with the findings in Mekelle Ethiopia (Hailemariam et al., 2020), in South Africa, being married was positively associated with PA (Watson et al., 2017). This discrepancy might be the majority of study participants in Mekelle attending high school level of education, and about 94% living in the urban area. Moreover, the difference could be due to the sociocultural of the population, sample size, and type of tools used in the study. These findings illustrate the need for comprehensive interventions that address social, environmental, and individual factors to enhance physical activity during pregnancy. Expanding health education and community outreach may significantly increase the acceptance of physical activity recommendations among pregnant women.
Finally, this study found that pregnant women with a good perception of the benefits of physical activity was 4.78 times higher odds of physical activity than those with poor perceptions. This study is in line with a study conducted in Deber Markose Referral Hospital, Northwest Ethiopia (Addis et al., 2022) showing women with high awareness of physical activity benefits had significantly higher activity levels. This study also comparable with studies in Australia and Canada that educational interventions and perception shifts effectively improve physical activity among pregnant women (Davenport et al., 2019). This result aligns with findings from others, indicating that pregnant women generally view physical activity as beneficial, important, and safe in comparison to those who hold negative perceptions. Nonetheless, a significant number of women fail to meet the recommended physical activity guidelines during pregnancy, which is contrast to the guidelines for non-pregnant individuals.
Strengths and Limitations of the Study
The study tried to address the knowledge, attitude and level of physical activity among pregnant women. The Nurse practitioners should educate pregnant women about physical activity benefits and safety. Nurse practitioners can help women overcome barriers to meet physical activity guidelines. Nurses’ role supports pregnant women to enhance knowledge of exercise and increase exercise behaviour during pregnancy through nursing process at antenatal care clinic. Pregnant women focus on preforming at least 150 min per week moderate-intensity aerobic PA. The limitation of this study might not be generalized to the whole pregnant women population. In addition, the current study did not include important information like dietary habits, preexisting health conditions, and missed in-depth data on cultural norms, family support, and community beliefs, which could influence the PPA.
Implication for Nursing Practice
Understanding a pregnant woman's knowledge, attitude, and practice (KAP) regarding physical activity is crucial for nurses to provide effective care and promote healthy pregnancies. Nurses can leverage this understanding to tailor education, address misconceptions, and encourage safe and appropriate physical activity during pregnancy, ultimately improving maternal and fetal outcomes. Nurses should actively educate pregnant women about the benefits of physical activity, such as reduced risk of gestational diabetes, improved mood, and easier labor. Address misconceptions that many women fear that exercise may harm the fetus, which leads to low participation. Use culturally sensitive approaches, especially in communities where exercise during pregnancy is seen as inappropriate
Conclusions
This study revealed that pregnant women reported low physical activity practice. Factors such as antenatal care attendance, place of residence, marital status, maternal age, and personal beliefs were significantly associated with physical activity. Thus, integrated physical activity counseling should be instituted into Antenatal Care (ANC) services specifically at the hospital level. Intervention that improve awareness on the benefits of physical activity during pregnancy along with personalized counseling should be considered rural dwellers, married and young age women.
Footnotes
Abbreviations
Acknowledgment
We are grateful to the participants and would also like to acknowledge the data collectors and supervisors.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from Haramaya University, the College of Health and Medical Sciences, Institutional Health Research Ethics Review Committee (IHRERC). The ethical approval ref.no was IHRERC/237/2023 on November 30, 2023. Respondents gave written consent and signature before starting interviews. The study was carried out by the Declaration of Helsinki.
Consent to Participate
All participants provided their written consent to participate in the study, which was obtained prior to the interviews.
Consent for Publication
Not applicable. This study does not involve the publication of any identifiable patient/participant data or images
Authors’ Contributions
RSA, AM, and BHA conceived the study, analyzed the data, and wrote the first draft of the manuscript. All authors contributed to the interpretation of the results. All authors commented on drafts and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request