
Abstract
Background
Morbidity and mortality related to acute poisoning is a major public health issue in both developing and developed countries. Community pharmacists have a crucial role in ensuring drug availability, increasing drug safety, counseling patients, overdose risk reduction and management, and provision of appropriate drug information. This study aimed to assess the availability of necessary antidotes in community pharmacies in Gondar and Bahir-Dar cities, Ethiopia, and the role of community pharmacists in the management of acute poisoning.
Methods
A cross-sectional survey was conducted in Gondar and Bahir-Dar cities. A self-administered, structured questionnaire was used for data collection and Statistical Package for Social Sciences (SPSS) version 24.0 was used for data analysis. Chi-square analysis was computed to identify the associated factors with a confidence interval of 95% and a P value less than .05 was used as a cut-point for statistical significance.
Results
Out of 101 community pharmacies invited to participate in the study, 80 of them completed the survey with a response rate of 79.2%. The overall mean antidote availability score was .59 (SD = .837), which falls within the definition of Poor availability. None of the pharmacies had kept all of the antidotes, and the maximum number of an antidote kept by a single pharmacy was 7 out of nineteen essential antidotes surveyed. The most commonly reported reason for the unavailability of essential antidotes was stock was not ordered (56.3%) followed by stock ordered but not delivered from suppliers (wholesalers) (20.0%). More than 3 fourth of the respondents (83.8%) had poor knowledge about the antidotes for the common poisonings.
Conclusion
There was a significantly very low availability of essential antidotes in the community pharmacies. Strategies should be implemented to improve pharmacist’s knowledge about antidotes, and management of poisoning emergencies through on-job training and provision of reference materials.
Introduction
Acute poisoning is a medical emergency in which the toxic effects occur almost immediately, usually within hours from the time of exposure. 1 Exposure to agrochemicals, medicines, and environmental agents may cause poisoning. 2 It is a common public health problem in low- and middle-income countries due to the absence of strong regulation and health care services. 3 In many low-income countries food poisoning, an overdose of drugs, insecticidal, herbicides, animal biting, and plant poisonings are the common cause of poisoning in human beings among which organophosphate poisoning is the leading cause of death especially in rural areas. 4
Currently, morbidity and mortality related to acute poisoning is a major public health issue in both developing and developed countries. 1 According to a WHO report, acute poisonings were estimated from 2 to 3 million cases annually; of which 1 million are severe poisonings resulting in 20, 000 deaths annually throughout the globe.5,6 The report also showed the distribution of poisoning mortality by region in which it was 8% in Africa, 7% in America, 5% in Europe, 19% in the Eastern Mediterranean region, 7% in the Southeast Asian region, and 7% in the west pacific region. 7 In Africa, organophosphate poisoning is a lead cause of poisoning. The report showed that in Zimbabwe around three-quarters of hospital admissions related to poisoning were due to self-poisoning using organophosphates and findings from Malawi revealed that 80% of suicide activities were using pesticide ingestion. 8 However, evidence shows that the lack of reliable in-country data and under-reporting is very common in many countries and makes it difficult to know the true impact of acute poisoning in these countries. 9 Taking snakebite envenoming alone, the under-reporting is believed to be over 70% in many developing countries, while conservative estimates show that, it kills 81,000–138,000 people every year, and leaves another 400,000 people with significant disabilities, such as amputated limbs and blindness.9,10
Management of acute poisoning is a challenge for health professionals. 4 It needs to properly define, identify, and quantify the causes of poisoning and the status of acutely poisoned patients. 11 Many countries do not have enough antidotes, screening tests, and proper treatment protocols. 12 In the management of poisoning, prevention from exposure to dangerous and potentially dangerous substances is very crucial. Antidotes are therapeutic substances that are important for the prevention or minimization of morbidity and mortality due to poisoning. 13 Besides, it is also important that the right antidotes be administered at the right time and right dose. The management of poisoning requires adequately equipped medical support and multi-health professional experts including pharmacists. 14
Pharmacists are one of the most trusted health professionals by consumers, 15 and have an important role in the management of acute poisoning and strengthening the health care team.16,17 For several years, pharmacies have also served as a sole source of drugs including antidotes for poisoning. 16 In global health, community pharmacies have a crucial role in ensuring drug availability, increasing drug safety, counseling patients, overdose risk reduction and management, and provision of appropriate drug information. 18 Besides, community pharmacists can also play an important role in the prevention of poisoning through the education and training of the public. 19 It is therefore very important for a pharmacist to have adequate knowledge about poisoning and its management as well as know-how to respond to an emergency involving intentional or unintentional poisoning.14,19 However, beyond these roles, pharmacists are underutilized throughout the world in the management of acute poisoning. 18
Compared to many developed countries, very little is known about the prevalence, management practice, and outcome of poisoning in developing countries. 20 The availability of essential antidotes at health facilities including community pharmacies is also a great challenge for many developing countries. A study conducted in Pretoria, South Africa reported that there was great variability in the stocking of antidotes at the community pharmacies in which 40% of the surveyed pharmacies stocked no antidotes at all and none of the pharmacies kept all the 19 antidotes listed. 21 Besides, frequent unavailability of antidotes at health care facilities, their expensive price, and often doubtful quality, forces many poisoning victims seek alternative and typically ineffective treatments from traditional healers. 10
In Ethiopia, pharmaceutical products are available at health facility pharmacy stores and pharmacy settings in the community; pharmacies, drug stores, and/or rural drug vendors. Pharmacies, drug stores, and rural drug vendors are types of community pharmacy setups that differ by the number and type of pharmaceuticals they hold. 22 In addition, pharmacies are run by pharmacy professionals that hold a pharmacy degree, and drug stores and rural drug vendors are managed by pharmacy diploma holders. In the country, there is unrestricted distribution and free access to insecticides, herbicides, and rodenticides which may contribute to the increased risk of the public to the hazardous effects of those substances.23,24 One retrospective study conducted at the University of Gondar hospital, Ethiopia revealed that the prevalence of acute poisoning was .67% among patients admitted to the emergency ward of the hospital. 25
The Ethiopian Food and Drug Authority (the then Drug Administration and Control [DACA]) Proclamation stated that “no person shall manufacture, import and distribute poisons unless s/he first have obtained a special permit from the authority, and any person who manufactures, imports or distributes poisons, shall keep detailed records of such poisons per the directives that may be issued by the authority and reports to same.” 26 In Ethiopia, although there are initiatives to establish poisoning centers, they are not currently functional, and thus victims are directly reporting and being treated at the health facilities.27,28
The following antidotes are listed in the National Essential Medicines List of Ethiopia (ENML); Acetylcysteine, Activated Charcoal, Calcium Gluconate Injection, Deferoxamine Mesylate, Digoxin Immune (Fab Ovine) Digoxin-specific, antibody fragments, Flumazenil, Lipid emulsion Injection, Phytomenadione (Vitamin K1), Sodium Nitrite, Physostigmine, Naloxone hydrochloride, Pralidoxime Chloride, Protamine sulfate, and Snake Venom Antiserum Polyvalent. 29 These antidotes together with additional antidotes not on the NEML (a total of 25 antidotes) are also included under the list of medicines for community pharmacies in Ethiopia. 30
To the authors' best knowledge, this is the first survey that summarized comprehensive data on the role of community pharmacists in the management of acute poisoning and the availability of antidotes among community pharmacies in Ethiopia. Therefore, this study aimed to assess the knowledge and practical aspects of community pharmacists in the management of acute poisoning, and the availability of essential antidotes in community pharmacies found in northern Ethiopia.
Study Methods
Study Design and Setting
A cross-sectional study was conducted from May 1st to June 7, 2020, on community pharmacies in Bahir-Dar and Gondar cities, Amhara regional state, Ethiopia. Bahir-Dar is the capital city of the region and is situated 565 km from Addis Ababa, the capital city of the country, while Gondar is located 185 km away from Bahir-Dar. Based on a projection from the 2007 National Census, the population size of Bahir-Dar is estimated at around 249,851, and 227,100 for Gondar (34). At the time of the study, there were 14 pharmacies, 32 drug stores, and 8 rural drug vendors in Bahir-Dar, while there were 19 pharmacies and 33 drug stores in Gondar.
Sample Size Determination and Procedure
The source population was all licensed community pharmacies in Gondar and Bahir-Dar cities, Ethiopia. During the study period, there were 54 licensed pharmacies in Bahir-Dar and 52 pharmacies in Gondar, respectively. Of the total available pharmacies, 5 of them participated in the pretest which was used for validation of the data collection tools, and these were excluded from the final survey. Then, from the remaining pharmacies, only one pharmacist was taken as some pharmacies may have more than one pharmacist on the premises. A random sampling method was used to recruit the final interviewed pharmacists from each pharmacy.
Pharmacists that were not available at the time of data collection and those that declined to participate were left out of the study. In situations when there was more than one pharmacist in one pharmacy and if one of them had declined to participate or was not available during the data collection time, a chance was given for the next pharmacist available to participate in the study. Though it did not happen during the present study, if the next available pharmacist had also refused to participate, then the data collectors were told to move to the next available pharmacy leaving the unresponsive/unavailable one.
A total of 101 community pharmacists were invited to participate in the survey (Figure 1). Availability of antidotes and the different roles of pharmacists in poisoning management were considered as dependent variables and the independent variables include socio-demographic characteristics of the study participants (sex, age, educational level, residency, year of work experience…), previous education/training on poisoning management, etc. (Figure 2) Workflow. Conceptual framework. *Financial problems, transportation problem, complexity of the purchasing system.

Data Collection Tool and Technique
Data were collected by 6 well-trained data collectors; 3 data collectors from Bahir-Dar and 3 from Gondar, using a self-administered, structured questionnaire. The questionnaire was developed after a careful literature review of previously conducted similar studies.21,31–33 The tool was pre-tested on 5 pharmacies and relevant modifications were performed before the commencement of the actual data collection. The final questionnaire constituted 17 items that were divided into 2 main sections
A pharmacy was classified as having a good availability of antidotes if it has stored ≥12 antidotes out of the 19 and classified as poor if have <12 antidotes. A pharmacist was classified as having good knowledge if correctly identify the antidotes for ≥5 out of the 8 toxicities and poor if responded for less than 5. Opioids, alcohol, benzodiazepines, digoxin, acetaminophen, iron, oral anti-coagulants, and heparin are the common causes of acute poisoning in Ethiopia. 28
Data Quality Assurance and Analysis
At the end of each day, the collected data were checked for completeness, accuracy, and consistency before feeding for analysis. The finally checked data were entered into and analyzed using Statistical Package for Social Sciences (SPSS) software for Windows version 24.0. Descriptive statistics like, frequency, percentage, mean, standard deviation, and median were used for data presentation. Chi-square analysis was computed to identify the associated factors with a confidence interval of 95% and a P value less than .05 was used as a cut-point for statistical significance.
Result
Demographic Information on the Study Participants
Socio-demographic characteristics of the study participants.

Availability of Antidotes
Availability of essential antidotes at community pharmacies.

Among the available antidotes, folinic acid was present in 1 drug store from the total of 28 drug stores, and 13 pharmacies out of the total 52 surveyed have stocked the antidote. The difference between the type of facilities was also statistically significant (P=.016). Concerning atropine, 8 drug stores out of the 28 (40%) had the antidote in their premises while 42.3% of the pharmacies (22 out of 52) had it in stock. Naloxone was only present in the pharmacies, 3 out of 52, while on the other hand activated charcoal was present in a drug store only, 2 drug stores out of the total 28.
Reasons for Unavailability of Antidotes
The most commonly reported reason for the unavailability of essential antidotes was “stock was not ordered” 45 (56.3%) followed by “stock was ordered but not delivered from suppliers” 16 (20.0%). (Figure 3) Common reasons for the unavailability of essential antidotes at community pharmacies.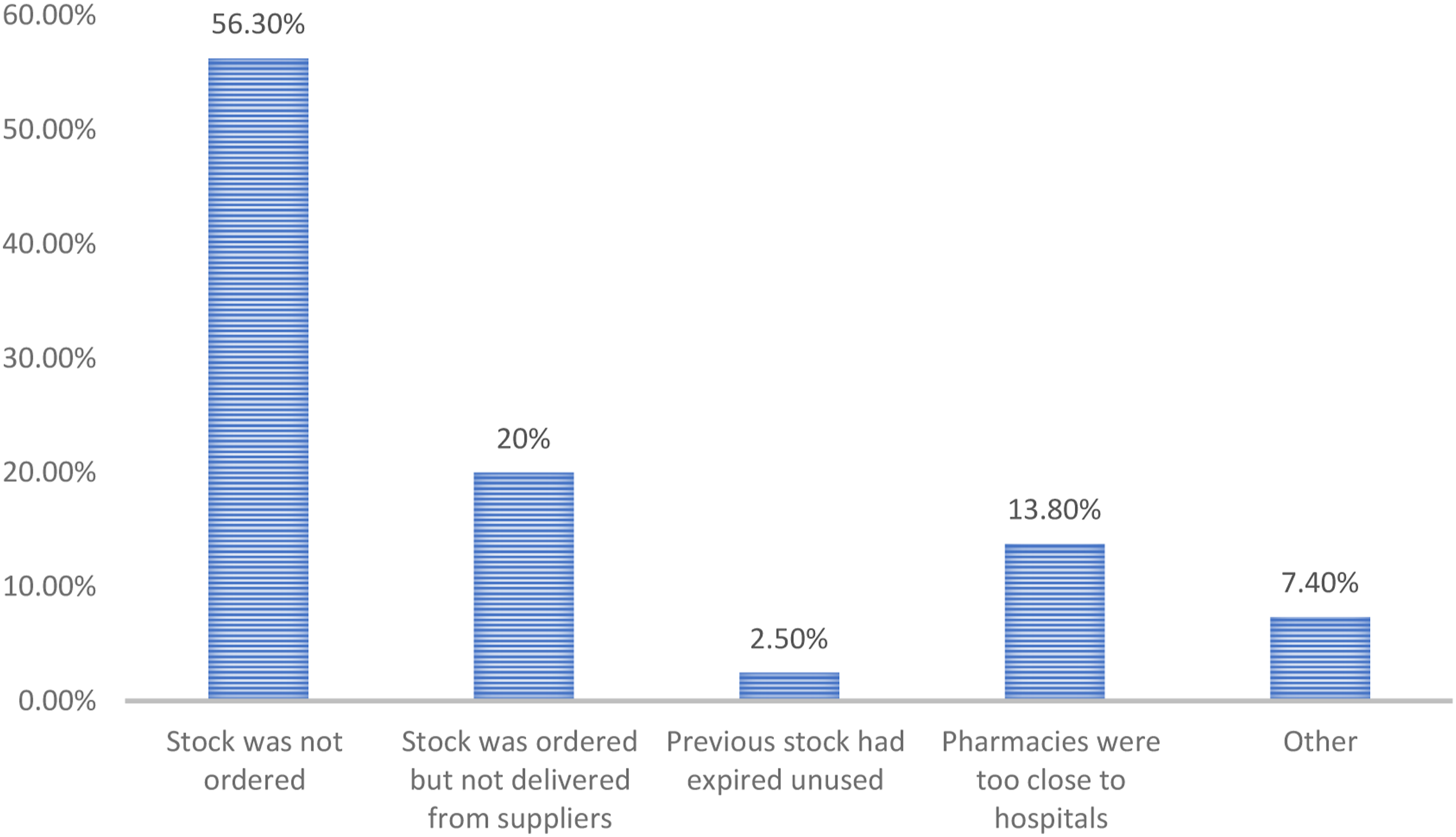
Knowledge of Community Pharmacists About the Common Antidotes
Factors associated with pharmacists’ ability to identify poisoning materials ingested by a patient.

Pharmacists’ response to the antidotes for common poisonings/toxicities.

Poisoning Management Practice of Community Pharmacists
Roles of community pharmacists in the prevention/management of acute poisoning.


Common poisoning materials for the poisoning cases experienced at community pharmacies in Gondar and Bahir-Dar (N = 7).
When asked about what was the first thing they will do if a poisoned person suddenly presented to their facility, 29 (36.3%) of them reported that they will refer to a physician while 22 (27.5%) reported that they will first ask what happened. (Figure 5) First measure taken by community pharmacists if a poisoned person presented to them (N = 80).
Chi-square analysis was also conducted to identify factors associated with the pharmacist’s ability to identify the poisoning agent a patient may have ingested when presented unconscious to his/her facility. The results showed that previous education/training on toxicology/poisoning management was significantly associated with pharmacists’ ability to identify the causative agents (P = .002) (Table 3).
Discussion
The present study assessed the pattern of essential antidotes availability at 2 cities in North Ethiopia and examined the role played by community pharmacists in the management of acute poisoning.
The study revealed that from the total community pharmacies surveyed, the majority of them (58.8%) do not have any of the essential antidotes and the overall mean antidote availability score was also significantly very low. This finding was very lower when compared with a similar study conducted in Pretoria, South Africa in which 60% of the community pharmacies surveyed had at least one antidote and the maximum number of an antidote stored by a single pharmacy being 11/19 compared with 3/19 in the current study. 21 This is very concerning because antidotes are the mainstay of treatment for poisoned patients and their availability is a crucial factor for the overall prognosis and outcome of the patient. Even though the occurrence of acute poisoning is a rare condition, if it is not properly treated for the first time, it can result in serious consequences for the patient’s future health (including death) in which the timely administration of an antidote is a determinant. 14
In the current study, the overall percentage availability of activated charcoal is significantly very low, 2.5%. This is very concerning since organophosphate (pesticides) poisoning and toxicity from bleaching agents are the common types of poisonings in Ethiopia for which activated charcoal is an important component of the management protocol.28,32 Organophosphates and bleaching agents were the leading causes of poisoning in studies conducted in Addis Ababa,31,34 and Gondar. 25 This showed that activated charcoal should always be available in every pharmacy premises and stocked in enough amounts.
The most commonly reported reasons for the unavailability of essential antidotes were not ordering the stock, the stock is ordered but not delivered from suppliers, the proximity of the pharmacies to hospitals, and the previous expiry of antidotes without being used, respectively. These findings were similar to a study conducted in Pretoria, South Africa. 21 Even though some of the reasons may be logical, such as because of fear of money loss due to expiry as many of them may not be utilized, it is not acceptable not to order or keep antidotes for only fear of financial loss as this will leave the community in great danger. Any delay in the administration of an antidote for any reason could negatively affect the overall prognosis of the patient and could also increase his/her chance of death from the poisoning. Similarly, proximity to a hospital is not a valuable reason for not keeping antidotes because hospitals may also not have a regular stock of antidotes or may run out of stock. One probable reason that may be associated with the health care system could be “stock being ordered but not delivered from suppliers,” as this may rather denote a problem in the pharmaceutical supply chain system. In the Ethiopian health care system, public health facilities (public hospitals, health centers and health posts) mainly obtain their pharmaceuticals including antidotes from the government, the Ethiopian Pharmaceutical Supply Agency (EPSA), unless the agency is stocked-out itself and in which case they can procure from private agencies. However, private health institutions including community pharmacies can purchase pharmaceuticals from EPSA and/or private companies without any restriction.
In the present study, more than 3 fourth of the respondents had poor knowledge about the antidotes for the common poisonings, and more than 3 fourth of them were unable to identify the specific type of poisoning material using the patients’ symptoms and/or any additional physical diagnosis, if he/she presented to them unconsciously. This is very worrying because pharmacists are expected to master such kinds of knowledge due to their expertise (as they took pharmacology and toxicology courses more than the other health professionals) and this will render them from making a significant contribution to the management of poisoned patients. 19
A pharmacist is expected to contribute to the management of poisoning/toxicity in various ways. As a result of his/her detailed knowledge of over-the-counter and prescription drugs, and other potentially dangerous materials, a pharmacist can serve to make judgments on the type of material ingested and the toxic liability of that specific material. 19 She/he can do this not only through the gross examination of the product, but the specific analysis of the ingested material that s/he acquired through his/her training in analytical and medicinal chemistry. With additional information from the patients’ caregivers or other sources, the pharmacist should also be more familiar with other medications that the poisoned person may also be taking and he/she can contribute to the therapeutic management by selecting the appropriate drug therapy for that particular patient. 19
Evidence from a previous study conducted in Ethiopia showed that the education level of victims of acute poisoning was reported to be lower. 35 This brings a huge responsibility for pharmacists to master a great deal of knowledge in the overall aspects of poisoning prevention and management. They should provide proper counseling and guidance to such victims whenever presented to their premises to prevent future similar incidences. Such types of counseling services should also include psychological guidance and support as previous studies reveal that intentional poisonings were very common in Ethiopia.25,34–37 As such, pharmacists need to equip themselves with such kinds of knowledge and skill to provide good pharmaceutical care, and effectively execute their professional responsibility.
In general, the present study revealed that the availability of antidotes for managing poisoning emergencies at community pharmacies is incomplete and needs to be improved. Recent evidence shows that antidote deficiency is a worldwide problem but the degree of the problem and the main reasons are different across countries.38–41 Stringent policies that ensure the availability of essential antidotes at health care facilities and monitoring pharmacy professionals’ ability to manage emergency poisonings are mandatory. The ministry of health and other local governments may need to impose stringent regulations regarding the availability of essential antidotes at these facilities and punish those that violated the regulations. For example, in the United States, the state of California has sanctioned a hospital for violating a regulation that require the availability of prescribed medications 24 hours a day. 42 In addition, it is recommended that pharmacies have sufficient items of antidotes to improve the overall management practice of acute poisoning and pharmacy professionals should take the responsibility in preparing a list of antidotes that should be available at their premises at all times. This could also include the adaptation of clear procurement procedures for obtaining other antidotes in an emergency, as it is in New Zealand. 38 Organizing an expert panel representing diverse disciplines such as; clinical pharmacology, medical toxicology, critical care medicine, hematology/oncology, hospital pharmacy, emergency medicine, emergency medical services, pediatric emergency medicine, pediatric critical care medicine, poison centers, hospital administration, and public health could be an effective strategy to create recommendations for antidote stocking. 43
Strategies should also be implemented to improve the overall knowledge of community pharmacy professionals on how to identify and treat emergency poisonings. Evidence shows that, overall antidote awareness creation programs and continuous educational programs of health care professionals together with record keeping of poisonous cases are very effective strategies. 40 Besides, in addition to providing educational programs, higher education institutes such as Universities could also engage in establishing poisoning centers and collaborate with health care institutions (hospitals). 39
Limitation of the Study
As the current study is a cross-sectional study, it cannot reveal a cause-and-effect relationship. The second limitation could be, as most of the answers were dependent on the pharmacist’s response to the various questions, there may be respondent bias in case of some sensitive questions. The study was conducted in 2 cities, Bahir-Dar and Gondar, and thus even if most cities and health programs in the country may share similar characteristics, generalization of the results to other geographic areas with different properties could be difficult.
Conclusion
There was a significantly very low availability of essential antidotes in the community pharmacies. The pharmacist’s knowledge about poisoning materials and their antidotes was also unsatisfactory denoting a need for further training in the subject area. Gaps in the supply chain system were also identified that could determine the timely availability of essential antidotes.
Recommendations
Community pharmacies should keep essential antidotes in their premises at all times with a particular focus on antidotes used for the most common acute poisonings in the areas. Strategies should be implemented to improve pharmacist’s knowledge about antidotes, and management of poisoning emergencies through on-job training and provision of reference materials. Improvements are also needed in the pharmaceutical supply chain system as the supply lead-time to avail essential antidotes on time is a very determinant factor for the effective management of acute poisonings.
Footnotes
Acknowledgments
The authors would like to thank all the study participants for their participation and collaboration in the study.
Author’s contributions
All authors contributed equally to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Competing interests
The authors declare that they have no competing interests.
Funding
The author’s received no specific funding for this work.
Ethical Consideration
The ethical committee of the school of pharmacy, the University of Gondar, had approved this study with an approval number of SoP-784/2020. The study was performed following the Declaration of Helsinki as revised in 2013 and the study participants were well informed about the purpose of the study as well as participation was voluntary. Informed written consent was obtained from each of the participants before data collection, and the data was collected anonymously with no personally traceable information on the questionnaire. The confidentiality of the data was also maintained throughout the study.
Consent for publication
All the authors have given their final approval of the manuscript and agreed for publication.
Availability of data and materials
The data sets generated and/or analyzed during the current study are not available in public due to the requirement of confidentiality upon which consent was secured from the study participants but is available from the corresponding author on reasonable request.