
Abstract
Despite numerous studies on primary care doctors’ remuneration and their job satisfaction, few of them have quantified their views and preferences on certain types of remuneration. This study aimed at reporting these views and preferences on behalf of Greek doctors employed at public primary care. We applied a 13-item questionnaire to a random sample of 212 doctors at National Health Service health centers and their satellite clinics. The results showed that most doctors deem their salary lower than work produced and lower than that of private sector colleagues. Younger respondents highlighted that salary favors dual employment and claim of informal fees from patients. Older respondents underlined the negative impact of salary on productivity and quality of services. Both incentives to work at border areas and choose general practice were deemed unsatisfactory by the vast majority of doctors. Most participants desire a combination of per capita fee with fee-for-service; however, 3 clusters with distinct preferences were formed: general practitioners (GPs) of higher medical grades, GPs of the lowest medical grade, residents and rural doctors. Across them, a descending tolerance to salary-free schemes was observed. Greek primary care doctors are dissatisfied with the current remuneration scheme, maybe more than in the past, but notably the younger doctors are not intended to leave it. However, Greek policy makers should experiment in capitation for more tolerable to risk GPs and introduce pay-for-performance to achieve enhanced access and quality. These interventions should be combined with others in primary care’s new structure in an effort to converge with international standards.
Introduction
Most of the studies, published in the international literature, on primary health care (PHC) doctors’ remuneration have been conducted from a payer perspective. As such, they are descriptive of its technical implementation1-5 as well as its (potential) outcomes.6-10 From a provider perspective, the examined issue is superficially approached by multidimensional job satisfaction surveys.11,12 Few studies have quantified doctors’ preferences on and assessment of their type of payment.13,14 This is a surprising upshot given that most remuneration schemes are awarded after negotiations between competent authorities and professional associations7,15 along with the World Health Organization’s (WHO) 16 pillar of participatory leadership reforms as a means of achieving “better health for all.”
In Greece, PHC is provided by self-employed professionals, contracted or not with health insurance funds, and publicly-owned units. 17 The latter include (a) rural health centers and their satellite clinics, (b) urban health centers formerly owned by the largest health insurance fund, the National Organization for Healthcare Provision (EOPYY), 18 and (c) public hospitals’ outpatient departments. Self-employed professionals are paid on a fee-for-service (FFS) basis, while public servants are employed under predefined and “fixed” wages which are also elastic to fiscal developments. An abnormal attribute is that, despite the recent (January 1, 2015) administrative unification of type (a) and (b) units under the so called National PHC Network (PEDY), their medical staff’s wages and employment conditions have not been equated so far. Doctors at type (a) units (and type (c) as well) enjoy a special—and therefore higher—payroll, excluding rural doctors who are entitled to the standard public sector payroll. Full-time and exclusive employment contracts are applied to all of them. Doctors at type (b) units are also beneficiaries of the standard payroll; however, some of them have acquired the legal right to continue to operate their private practices, which was common before PEDY. This practice implies FFS payments. Doctors at type (c) units have similar FFS benefits because the operation of afternoon outpatient clinics increases their income through direct payments from patients. The Greek literature includes only 1 relevant study which revealed low satisfaction levels with salary among doctors at health centers when compared with their qualifications and workload. 19 The same study also ranked salary as the most crucial determinant of job dissatisfaction. It is therefore interesting to investigate their current point of view taken into account at least 2 successive cuts on payroll as a resultant of the ongoing financial crisis.
Against this background, this study aimed at representing the Greek public PHC medical staff’s views on their remuneration and identifying internationally applied remuneration schemes which would probably be more preferable by them.
Methods
A 13-item questionnaire was used (provided as a supplementary file), created by the authors and tested for its validity and reliability. The first 3 items refer to respondents’ professional details, the next 9 focus on assessment of the current payment system (5-point Likert scale) and the last one refers to preferences. Validity testing included 10 cognitive interviews based on the concurrent think-aloud method. 20 A 10-day test-retest reliability was applied to validate the temporal stability. The answers of the 20 participants revealed high and statistically significant Spearman coefficients of all items.
The first step for sampling was to gain knowledge of population metrics. At the beginning of the survey, we only knew the total number of doctors employed at National Health Service (NHS) health centers (and their satellite clinics) as general practitioners (GPs), residents or nonspecialized doctors (1851 people in total 21 ). So, we asked additional information for this spectacular group from the 7 Regional Health Authorities (RHAs). The employees lists retrieved allowed us to geographically stratify the population and also by medical specialty and medical grade. Finally, the sample consisted of 280 doctors employed at this kind of PHC units. Sampling required the application of random number tables on employees lists after taking into account the known population parameters (geographical area, medical specialty, and medical grade). Only 212 doctors in total responded, which means that an average response rate of approximately 76% was achieved. The individual response rates among geographical areas, medical specialties, and medical grades were similar. Answers were collected via e-mail during the last 2 months of 2014. We included informed consent ensuring that all information collected will be used only for our research and will be kept confidential.
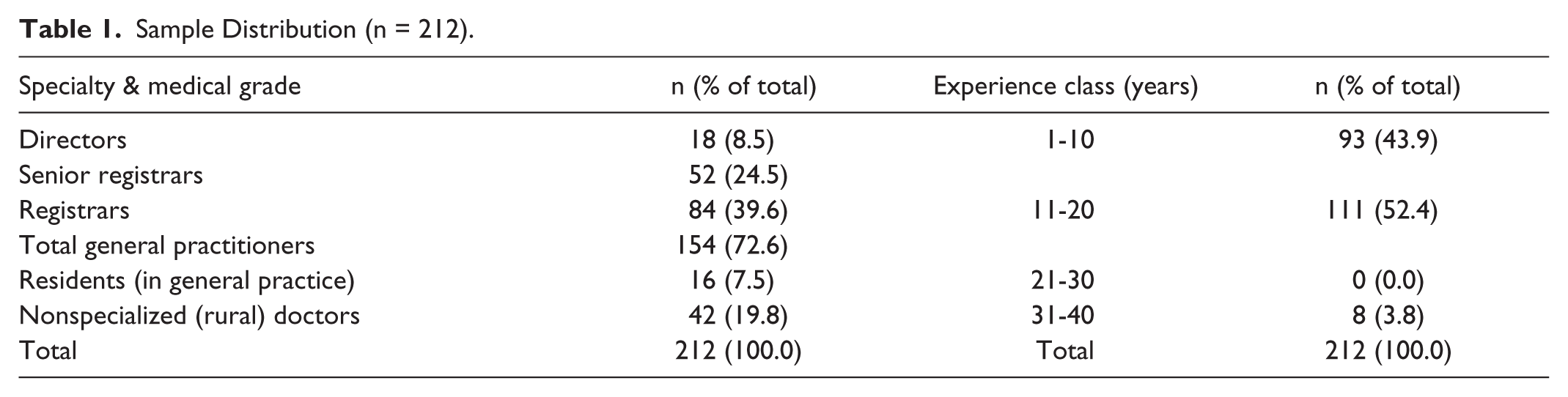
The sample attributes are demonstrated in Table 1 and show that most correspondents were GPs (72.6% of total). Among GPs, most of them were registrars (39.6% of total) in terms of medical grade, followed by senior registrars (24.5% of total) and directors (8.5% of total). All nonspecialized doctors were rural doctors and accounted for 19.8% of total doctors. At the same time, all residents were being specialized in general practice and accounted for 7.5% of total doctors. The predominant experience class was that of 11 to 20 years (52.4% of total), while only 3.8% of correspondents had experience higher than 20 years.
Sample Distribution (n = 212).
Standard statistical analysis on quantitative and ordinal variables was conducted, such as descriptive statistics, correlations, and parametric tests to compare means. Preferences on various remuneration methods were clustered using the decision trees technique. Its outcome is a tree (classification) which optimally predicts one doctor’s preferences based on his or her professional profile (medical specialty, medical grade, experience class).
Results
The results of Table 2 suggest that public PHC doctors are extremely disappointed with their salary which was deemed lower than work produced by 96.2% of them. There were not any negative answers to the first question; thus, the mean agreement score was the highest one among all items (4.66). By contrast, few doctors believe that their colleagues of different specialty are salaried better (8.5% of total). Another interesting finding was that 34.9% of correspondents deemed their salary lower than that of private sector doctors of same specialty. Furthermore, doctors tended to agree on average that salary does not favor service quality and even more productivity, as at least half of them agreed to some extent with both declarations. Salary’s impact on service quality was also highly correlated with that on productivity, and the relevant Spearman correlation coefficient (rho) was statistically significant. Most doctors did not accept that salary motivates them to claim informal fees from patients (81.1% of total); however, 3.8% of them did so. About 39.6% of correspondents agreed that the current remuneration scheme forces them to violate the exclusive employment principle, but a little higher proportion of them (42.5% of total) refused it. Incentives to be employed at border areas were considered to be satisfactory by only 3.8% of total doctors. The corresponding rate concerning the sufficiency of incentives to opt for being specialized in general practice was barely 5.7%. Moreover, a semistrong and statistically significant negative correlation between first and ninth question was found and denoted that the lower the salary compared with work produced, the less satisfactory the (financial) incentives to choose general practice.
Assessment of Current Remuneration Scheme.
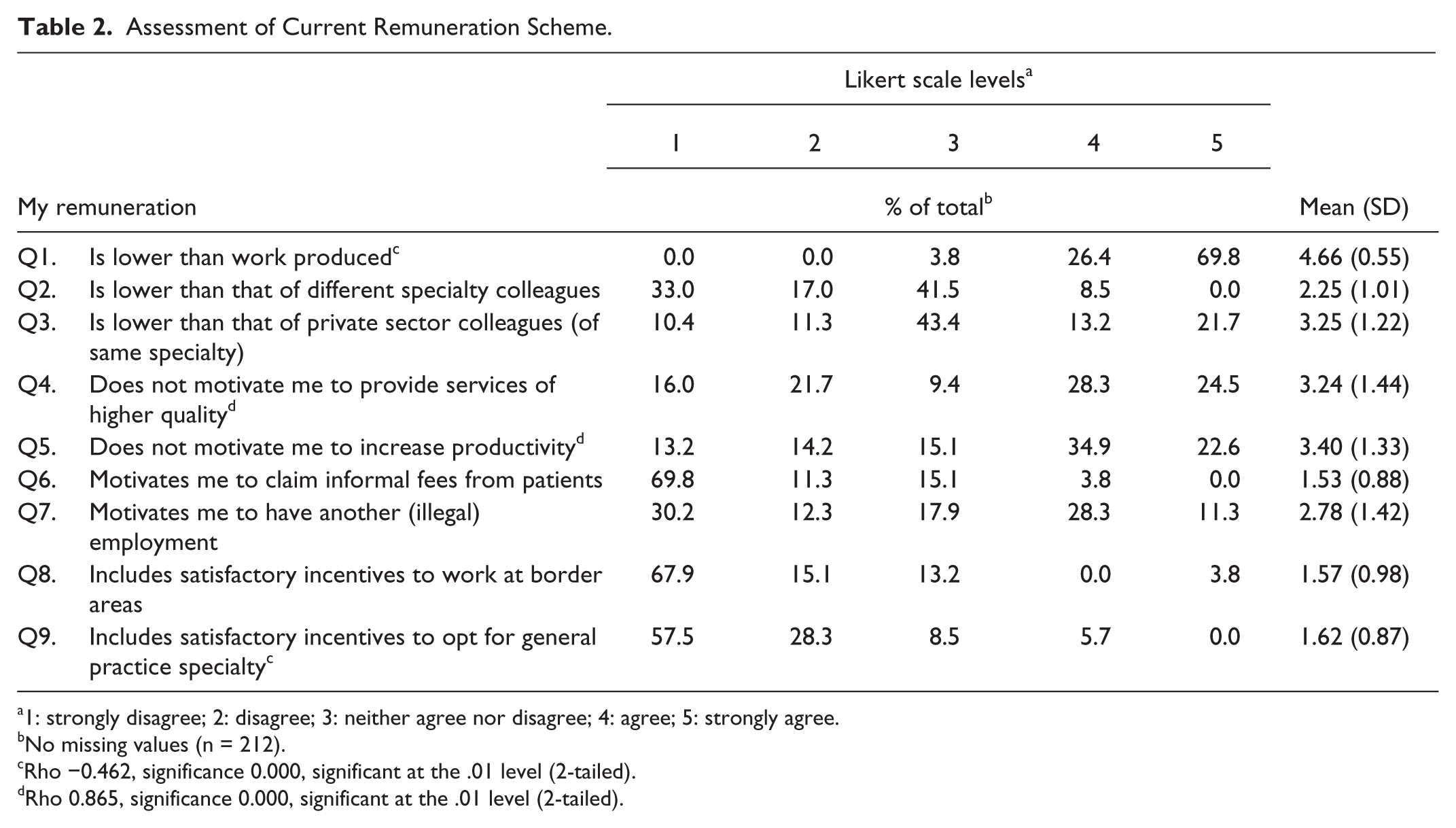
1: strongly disagree; 2: disagree; 3: neither agree nor disagree; 4: agree; 5: strongly agree.
No missing values (n = 212).
Rho −0.462, significance 0.000, significant at the .01 level (2-tailed).
Rho 0.865, significance 0.000, significant at the .01 level (2-tailed).
Table 3 summarizes the results of parametric tests to detect any differences between mean agreement scores after having classified the sample in accordance with its core attributes (of Table 1). Analysis of variance (ANOVA) test tracked whether there was at least 1 significant difference, whereas the post hoc test, Tukey Honest Significant Difference (HSD) examined all possible pairwise comparisons between means. Regarding the first question, residents appeared less disappointed than GPs and rural doctors on average, registrars less disappointed than senior registrars, and younger doctors (experience of 1-10 years) less disappointed than those with experience between 11 and 20 years. Regarding the second question, GPs constituted the only specialty group which disagreed on average that salary is lower than that of different specialty colleagues (mean score = 1.97), registrars’ mean disagreement was stronger (mean score = 1.60) than that of other medical grades, and doctors of highest experience (31-40 years) disagreed unanimously (mean score = 1.00). When asked whether their salary is lower than that of private sector colleagues of same specialty (third question), there were not any significant differences between specialties and medical grades, but doctors of 11 to 20 years’ experience were the only ones to agree on average (mean score = 3.71). GPs’ level of agreement with the proposal that salary does not motivate them to provide services of higher quality (fourth question) was much higher than that of other specialties (mean score = 3.45), but among GPs, registrars agreed less than average (mean score = 2.98). Classification based on experience level denoted significant differences between all groups; in particular, the more the experience the higher the mean agreement score (mean scores = 2.60, 3.64, and 5.00, respectively). GPs’ level of agreement with the proposal that salary does not promote their productivity (fifth question) was higher than that of nonspecialized doctors, among GPs, directors agreed more than registrars on average, and the most experienced doctors (31-40 years’ experience) agreed unanimously, similarly to the previous question. Salary as a motivator to claim informal fees from patients (sixth question) caused more positive answers by residents than other specialties, and registrars than directors. Furthermore, salary as a push to multiple employment (seventh question) was underpinned by nonspecialized doctors (mean score = 4.38) and those with up to 10 years’ experience (mean score = 3.24); however, GP directors were vigorously negative (mean score = 1.44). Incentives to work at border areas (eighth question) were deemed more unsatisfactory by GPs than nonspecialized doctors, senior registrars deemed them less unsatisfactory than other medical grades did, and there were no significant differences in terms of experience level. Last, incentives to opt for GP specialty (ninth question) were deemed more unsatisfactory by registrars than senior registrars, and no other significant differences were detected.
Assessment of Current Remuneration Scheme by Specialty, GPs’ Medical Grade, and Experience Class.

Note. GP = general practitioner; ANOVA = analysis of variance; HSD = honest significant difference.
Significance level .05.
Mean difference significant at the .05 level.
Node 0 of Figure 1 represents the overall results concerning preferences on type of remuneration, and shows that the most preferable remuneration system among correspondents was a combination of capitation with FFS (24.5% of total). Alternate options included the current system (17.9%), salary combined with capitation (16%), salary combined with FFS (15.1%), and capitation (10.4%). It is important to point out that 65.1% of doctors chose a system which included salary, whereas the remaining 34.9% of them were attracted by pure or combined per capita fees. The remaining nodes represent the optimally classified preferences. More specifically, capitation combined with FFS was recommended mainly by GPs of the 2 highest medical grades (i.e., senior registrars and directors), as shown in nodes 1 and 4. The latter node implies that this particular group of GPs is more tolerable to risk given that 57.2% of them preferred salary-free schemes. On the contrary, only 21.4% of registrars (node 3) would prefer pure or combined-with-FFS capitation, but most of them would prefer it only if combined with salary. The preferences of younger doctors are quite different (node 2); 24.1% of rural doctors and residents would prefer salary combined with FFS and 20.7% of them are supporters of the current scheme. Slightly more than one fourth of them would take the risk of salary-free schemes. However, only doctors of this particular cluster proposed the introduction of financial incentives, the so-called pay-for-performance (P4P).

Overall and classified preferences on remuneration (decision tree).
Discussion
The aforementioned results are consistent with the findings of the previous Greek study, in accordance with which 73.2% of doctors at NHS health centers had been considered unhappy with their salary in comparison with their qualifications and work produced. 19 Thus, dissatisfaction does not appear to be created by the Greek crisis, but the successive wage cuts starting from 2011 have boosted the proportion of dissatisfied doctors to a great extent (see answers to the first question). It is also of great importance that previous studies, even these on secondary care, confirm that the lowest score in job satisfaction for Greek doctors was that concerning salaries.22,23 Moreover, answers to the first question showed that the only significant difference was that between doctors of 11 to 20 years’ experience and those of up to 10 years’ experience. This result does not absolutely confirm that older doctors tend to be more dissatisfied with their remuneration.12,19
Answers to the second question revealed that few doctors believe that their colleagues of different specialty are salaried better, which is consistent with the fact that the current payroll is irrelevant to specialty. Actually, rural doctors’ standard payroll relies primarily on the years of work experience combined with professional qualifications (e.g., postgraduate education) and includes only 2 kinds of allowances: (1) family allowance and (2) frontier allowance. Contrarily, special payroll depends primarily on the medical grade, not directly linked to work experience, but has 3 additional allowances. Regarding third question, over one third of doctors deemed their salary lower than that of private sector colleagues of same specialty, especially those of midlevel experience (11-20 years), which would maybe cause health professionals’ shift from public to private sector or career brake in the near future. 24 Answers to the next 2 questions indicate that respondents agree on average with the negative impact of salary on productivity and quality of services,25,26 and this impact was highlighted by the most experienced doctors. On the contrary, the vast majority of doctors refused the negative impact of salary on their professional morality, but residents were almost indifferent to the linkage between salary and informal payments, and younger doctors, especially rural doctors, declared that they are led to dual practice even though it is prohibited. The latter cannot be dissociated from the fact that rural doctors are the only ones (at NHS health centers and satellite clinics) not enjoying the special payroll.
Over 8 out of 10 respondents, especially GPs, did not agree that there are satisfactory incentives to work at border areas (eighth question), due to which the Greek PHC might be threatened by shortage of medical staff at border areas. This situation could deteriorate after a recent law which lifted the mandatory rural service as a precondition for submission to medical specialty exams (given that rural doctors usually work at remote health centers or satellite clinics). Best practices can be found either in France 4 where there are financial incentives for self-employment at rural areas or in Australia 27 where subsidies to employers are granted under similar circumstances.
Moreover, approximately 86% of doctors questioned the effectiveness of existing incentives to make general practice an attractive specialty, which is known to be crucially influenced by working conditions and earnings, 28 and is additionally confirmed by the negative correlation between the first and the ninth item of our questionnaire. Furthermore, any improvement of these incentives would change the PHC structure as more medical school graduates would be attracted to general practice.14,29
The results regarding doctors’ preferences on their type of remuneration show that most PHC doctors prefer capitation combined with FFS to salary. Almost two thirds of them belong to a distinct group: GPs of the 2 highest medical grades. In total, 85% of individuals preferring the alternative payment system are GPs. Contrarily, 72% of residents and rural doctors did not opt for a payment not including fixed payments (salary). These results are coherent with the Norwegian case in which younger doctors are less tolerable to risk and desire salaried contracts.13,14
Another topic to be debated is whether remuneration constitutes a sound motivational factor of PHC doctors in Greece. A previous study on Greek hospitals showed that this happens only for those with managerial positions. 30 However, literature suggests that financial incentives make sense only if employees are convinced there is strong linkage between performance and rewards.31,32 On that occasion, the provisions of both standard and special payroll fall short of international standards.
A last emerging topic is that PHC generalists prefer mixed per capita payments like these applied to self-employed professionals in several European countries while PHC specialists would remain salaried. This could be criticized as favoritism shown to GPs especially in the case of higher earnings than specialists. Besides, in Organisation for Economic Co-operation and Development countries it is not used GPs to gain higher income than specialists. 33 However, as described above, changes in remuneration could rationalize the ratio of generalists to specialists 34 which is anyway distorted in Greece. 17
The aforementioned topics lead to some recommendations to health policy makers. First of all, PHC doctors in Greece should be motivated despite payroll constraints and also the most motivated doctors, and therefore most likely to highly perform, should deserve financial incentives. This presupposes a flexible payroll system. Second, policy makers should take into account that any changes on remuneration could eliminate systemic distortions such as dual practice, informal payments, belittlement of specific medical specialties, and so forth.
Limitation of the study was that we did not include specialists at NHS health centers whose preferences might be significantly different. Medical staff at other PEDY units were also excluded, because these units had not being fully monitored by RHAs at the time this survey was conducted. Medical staff at public hospitals’ outpatient departments constitute a further exclusion because, in any case, they cannot be easily separated from other medical staff of secondary or tertiary care. Moreover, the questionnaire did not include a gender item which would be useful for extra classifications. Finally, the results on preferences were unable to capture each doctor’s motivation in his or her choice. In other words, it is not clear whether the respondents chose the remuneration scheme which is better for themselves, their patients, or the entire health system. This is crucial information for health policy makers.
Conclusion
The main conclusion of this study concerning the public PHC doctors in Greece is their growing dissatisfaction with the current reimbursement method, howbeit they do not reach a consensus to change it. Only GPs of higher medical grades look ready to replace their ostensibly fixed income with per capita payments and/or FFS. This conceals that probably dissatisfaction relies on the amount of remuneration instead of the type of payment itself. However, radical changes in the remuneration of GPs, who have already expressed their preference on capitation through their professional associations, and adjustments to the remuneration of all medical specialties by introducing incentives (pay-for-performance), can lead to improved quality and access. In addition, the competent authorities have a great opportunity to reform the organizational structure of PHC using adjustments to remuneration and employment conditions as an intermediate objective.
Footnotes
Author Contributions
All authors participated in the research progress, revising the manuscript for important intellectual content and approved the final version for publication. SK and CK set up the study design under supervision of NP. SK collected all the data. SK analyzed and interpreted the data under supervision of and with help from NP and MT. SK drafted the manuscript with support from CK and NP.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.