
Abstract
Most disabled people have poor health status. They often have multiple diseases requiring continual medication. This study aimed to explore the factors associated with medication adherence among disabled people, with a particular focus on the factors associated with family and primary health care support. A questionnaire survey was conducted among 226 disabled individuals. The analysis was performed using an ordered logistic regression model, including 4 categories of predictor variables. We found that the community health service center played a positive role in improving medication adherence, whereas the role played by the participant’s family was more complicated. Specifically, those obtaining a brochure were more likely to have higher medication adherence (odds ratio [OR] = 2.732, 95% confidence interval [CI] = 1.349-5.532). Compared with those who were married, widowed participants (OR = 0.207, 95% CI = 0.069-0.620) and divorced participants (OR = 0.330, 95% CI = 0.057-1.914) had lower odds of having greater adherence, whereas the odds of having greater adherence for single participants were 1.679 times the same odds for married participants (OR = 1.679, 95% CI = 0.668-4.224). The odds of having greater medication adherence for participants receiving help with prescriptions from a family member were almost 60% lower than these odds for those who did not receive this kind of help (OR = 0.460, 95% CI = 0.216-0.979). Thus, the role played by participants’ family members was both protective and damaging, whereas the role of the community health service center was clearer. These findings merit further exploration.
Keywords
Medication adherence is quite significant to disabled people, as most of them have multiple diseases requiring continual medication.
Family support and social health care support were both tested in this article to figure out which variable matters more.
Family support played protective and damaging role simultaneously, the latter of which merited further exploration. The role of community health service center support was clearer: brochure delivering was the only effective way to improve medication adherence, indicating that there was a great deal more that family doctor teams could do to improve medication adherence among people with disabilities.
Background
Recent studies have shown that people with disabilities are less healthy compared with those without disabilities. This includes lower self-rated health, higher rates of obesity and diabetes, worse psychological health, higher levels of smoking, and poorer diet among disabled people. 1 In addition, about one-fifth of the disabled people have been found to have limited activity, which may trigger chronic diseases such as hypertension and diabetes. 2 A survey on the health status of disabled people in Australia reported that early onset of chronic conditions and chronic illness were more likely among people with disabilities: In rural Victoria, compared with the general population, a higher percentage of people with intellectual disabilities had diabetes (6% vs 12%), a higher percentage of people aged 18 to 39 with intellectual disabilities had heart disease (1% vs 8%), and a higher percentage of people with severe disabilities had hypertension (5% vs 9%). 3 Disabled people are more likely to have chronic diseases and require life-long medication, so medication adherence is especially significant to maintaining health for this population.
The consistency of individuals’ health-related behaviors with medical instructions (ie, adherence) is an important factor in health system effectiveness. 4 Treatment outcomes have been found to differ by 26% between high- and low-adherence patients. 5 Nonadherence increases morbidity, mortality, and avoidable health care costs for patients.6,7 Almost 125 000 deaths and 10% of hospitalizations in 2017 were estimated to be caused by lack of adherence in the United States. 8 Low medication adherence is a serious problem worldwide. The adherence rate to long-term medication therapies has been estimated at 40% to 50% in Hradec Kralove (Czech Republic). 5 More than 80% of people aged 65 years and above in the United States were found not to follow their prescription drug regimens, and more than 50% of patients taking antihypertensive drugs stopped treatment in 12 months.9,10 Recent research on medication adherence among disabled people is limited, but evidence has consistently shown low-adherence levels. Park et al 11 showed that disabled people were especially vulnerable to various diseases related to hypertension because of a low antihypertensive adherence rate. Another study found lower adherence among people with limb, brain, visual, auditory, or internal organ impairments than among those without these impairments.
The low medication adherence of disabled people remains unexplained, but it has been suggested that family support may be a significant factor. Studies have confirmed that married individuals tend to receive more and better health care than do the unmarried.12-14 Using data on 148 married patients with chronic pain and disability, Turk et al 15 showed that marital relationship quality was a critical mediator of chronic pain. Studies on drug adherence in Iranian patients with chronic diseases 16 and on promoting adherence in patients with β-thalassemia 17 have identified marriage as a significant factor in improving medication adherence, but further analysis has not been conducted. Besides, financial support is a significant part of family support, as widely documented in existing literatures. According to Cohen and Wills, 18 Winemiller divided social support into 5 categories, one of which was fundamental support, referring to financial aid and material resources. 19 In following studies, financial aid was considered as a significant perspective measuring family support.20,21
Support through primary health care is another factor thought to be important for medication adherence. In 2009, the Chinese government launched a new round of health care revolution, aiming to strengthen the primary health care system and to establish a well-functioning referral system. 22 The policy’s implementation strategy involves initially targeting vulnerable groups (including disabled people, older adults, and poor people) who make up approximately 30% of the population, and then to cover the entire population. 23 Individuals who are registered with a family doctor receive multifaceted services, including physical health examinations, health intervention plans, noncommunicable disease management, and frequently used medication services. Disabled people were prioritized by the government. A multi-cooperation intervention was adopted by community health service centers (CHSCs) to address the potentially complicated special situations faced by people with disabilities. Family doctors, family nurses, family pharmacists, and social workers work together to manage these people’s health. The initial intervention in CHSCs throughout China focused on medication. 24 Shanghai was the earliest pilot city implementing the family doctor system, which had been established in the year of 2013. Common measures taken by CHSCs in Shanghai focusing on people with disabilities include distributing informational medication brochures and providing medication education to improve patients’ understanding of medications and their adherence. However, the CHSC’s role in improving disabled people’s medication adherence has not yet been explored. This study tried to explore whether such measures mattered for the medication adherence for the disabled. Questionnaire was designed to collect related information. And we added one more variable, that is, “medicine use score,” within 15 items to test the effect of such measures, as recent studies had strongly suggested a positive effect of medicine knowledge on medication adherence.25,26
In general, this study aimed to explore the factors associated with medication adherence among people with disabilities, with a particular focus on factors linked to support from these people’s family and CHSCs, to provide new research ideas and directions for future investigations of medication adherence.
Methods
Data
The data were collected in Hongkou District, Shanghai. Using simple random sampling, we selected 230 individuals from the population of disabled people aged ≥18 years in the “Disabled People Information System” in Hongkou District. People with severe mental illness were excluded. We designed the “Pharmaceutical Service Demand Questionnaire for People With Disabilities” as a survey tool. This household survey was administered by trained investigators visiting the families of people with disabilities, accompanied by neighborhood committee officers who were familiar with these families to facilitate the survey administration. Data were collected on individual characteristics, disability status, family information, and CHSC service utilization. In total, 230 questionnaires were distributed. All questionnaires were collected, including 226 valid questionnaires, yielding an efficiency rate of 98.3%.
Measures
The dependent variable was “medication adherence,” the control variables were disability status and other individual characteristics that might affect medication adherence, and the key independent variables were family support and CHSC support.
Medication adherence
We used the Morisky Green Levine Medication Adherence Scale, 27 which includes 4 items: “Ever forgot to take medicines,” “Ever not followed the medication instruction manual,” “Ever stopped taking medicines when feeling better,” and “Ever stopped taking medicines if felt worse.” Response choices were “yes” or “no.” If the answers to the 4 questions were all “no,” participants were defined as having “full medication adherence.” If the answers to the 4 questions were all “yes,” participants were defined as having “full nonadherence.” Other participants were defined as having “some level of nonadherence.”
Individual characteristics
The included individual characteristics were sex (men [0] or women [1]), age, education level (primary school or below [1], junior high school [2], high school/secondary school [3], or university or higher [4]), retired (no [0] or yes [1]), medical payment method (insurance [0] or noninsurance [1]), and number of diseases.
Disability status
We included disability category (visual disability [1], hearing or language disability [2], physical disability [3], or multiple disabilities [4]) and disability level (level 1 [1], level 2 [2], level 3 [3], or level 4 [4]).
Family support
Family support was assessed using marital status (married [1], unmarried [2], widowed [3], or divorced [4]), monthly per capita income (<3000 yuan [1] or ≥3000 yuan [2]), family care (no [0] or yes [1]), and help from family members with prescriptions (no [0] or yes [1]). Monthly per capita income equals to family income divided by number of family members.
CHSC support
CHSC support was measured using indicators of whether the participant had obtained a medication adherence brochure (no [0] or yes [1]), medication education (never [0], once or twice [1], or 3 or more times [2]), and the common sense regarding medicine use score, which were linked tightly to the primary health care practice in Shanghai. The common sense regarding medicine use score was calculated from 5 questionnaire items: “Can you correctly identify the production date and expiration date of the medicine?”; “Do you know the difference between prescription and nonprescription medicines?”; “Can you distinguish between health products and medicines?”; “Do you know how to correctly understand adverse medicine reactions?”; and “Can you read and understand medical instructions?” A value of 1 was added to the score for each item that was answered correctly. Higher scores indicate better common sense regarding the use of medicine.
Analysis
We first used descriptive statistics to present a simple overview of the sample characteristics. Categorical variables (eg, sex and education level) are presented using frequencies and percentages, and continuous variables are presented using means (±SD). We then created a statistical description of the physical condition of the disabled participants. Ordered logistic regression was performed to explore the effects of factors influencing medication adherence among disabled people. We present these results as odds ratios (ORs). EpiData (Version 3.1) was used for data entry and establishing a study database. The database was then converted into “.dta” format, and the statistical analyses were performed using Stata (Version 13.0). A significance level of 0.05 was used for all analyses.
Results
Sample Characteristics
Individual information
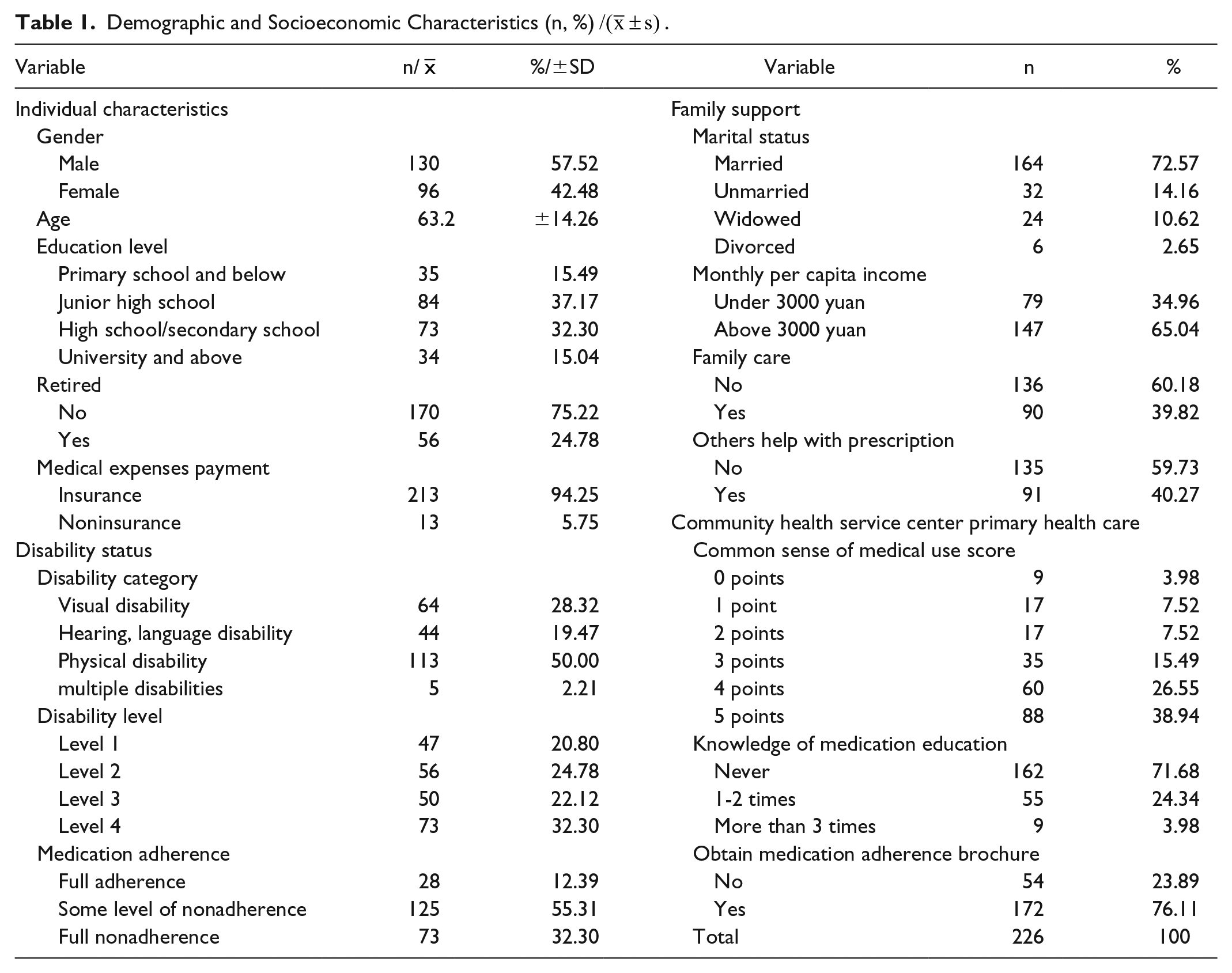
The sample included 130 men (57.52%) and 96 women (42.48%). The average age was 63.20 years (±14.26). A total of 84 participants (37.17%) had graduated from junior high school, and 73 (32.30%) had graduated from high school/secondary school. Most participants (170, 75.22%) had not retired, and 213 (94.25%) were covered by health insurance.
Disability status
There were 113 people (50%) with physical disabilities, 64 (28.32%) with visual disabilities, 44 (19.47%) with hearing and language disabilities, and 5 (2.21%) with multiple disabilities. Levels 1 and 2, representing more severe disabilities, were reported by 103 people (45.58%), whereas 123 participants (54.42%) reported level 3 or level 4 disabilities, which were less severe.
Family support
Most participants (164, 72.57%) were married, and 32 (14.16%), 24 (10.62%), and 6 (2.65%) were unmarried, widowed, and divorced, respectively. Monthly per capita income was not high: 79 people (34.96%) reported <3000 yuan/month. The percentages of disabled people receiving family care and help with prescriptions were both around 60%.
CHSC support
A total of 183 people (80.98%) scored ≥3 points on CHSC support, 162 (71.68%) had never received medication education, and 172 (76.11%) had received a medication adherence brochure.
Medication adherence
In terms of medication adherence, 28 people (12.39%) had full adherence, 73 (32.30%) had full nonadherence, and 125 (55.31%) had some level of nonadherence (see Table 1).
Demographic and Socioeconomic Characteristics (n, %)
Physical Condition of People With Disabilities
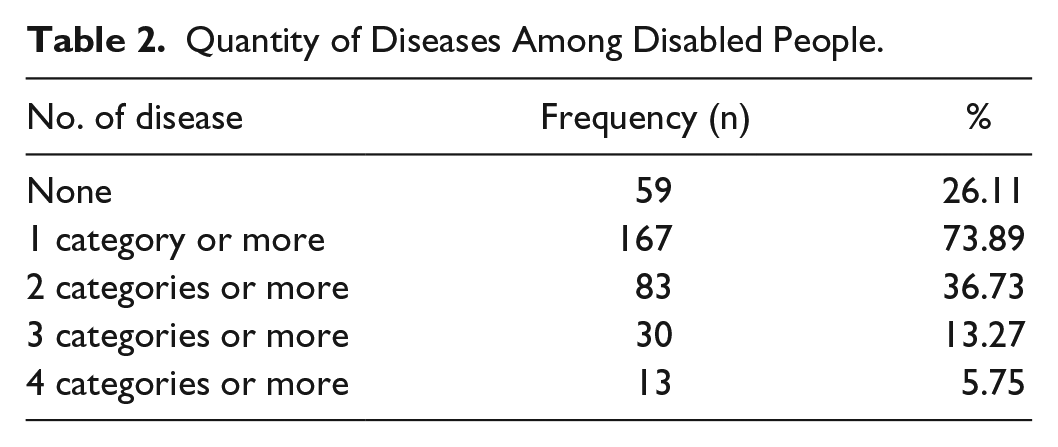
The physical condition of the study participants was quite poor. The majority of participants (73.89%) had at least one disease, 36.73% had at least 2 diseases, 13.27% had at least 3 diseases, and 5.75% had at least 4 diseases. The probability of a disabled person suffering from one disease was very high, and they often suffered concurrently from several diseases (see Table 2).
Quantity of Diseases Among Disabled People.
In terms of disease categories, 111 participants (49.12%) had hypertension. This was followed in frequency by coronary heart disease, stroke, hyperlipidemia, diabetes, and fatty liver, with specific morbidity rates of 16.81%, 13.72%, 13.72%, 9.73%, and 9.73%, respectively. In addition, people with disabilities often concurrently suffered from multiple diseases. For example, 24 people had both hypertension and coronary heart disease, accounting for 21.62% of the participants with hypertension; 20 people with hypertension also suffered from diabetes, accounting for 18.02% of those with hypertension. We inferred that most people with disabilities required medication services, making it particularly important to study medication adherence and its impact among this group (see Table 3).
Categories of Disease for Disabled People, n (%).

Multivariate Analysis of Medication Adherence
The ordered logistic regression analysis included 4 categories of predictor variables: individual characteristics, disability status, family support, and CHSC support. After including all variables, the pseudo R2 was 14.7% and the log likelihood value was −183.469 (P = .000), indicating quite good model fit.
The results of the ordered logistic regression showed that the 4 variable categories all significantly affected the medication adherence of disabled people. This was consistent with our preliminary research hypothesis, suggesting the necessity of controlling for these additional variables when testing the effects of family and CHSC support. Specifically, among the explored demographic characteristics, age had a significant impact on adherence. Each year of age increased the odds of greater adherence by 5.5% (OR = 1.055, 95% confidence interval [CI] = 1.022-1.089). There was an obvious pattern between education and medication, but this was not statistically significant. Compared with the odds for those with primary school or less education, the odds of having greater adherence were 1.433 times higher (OR = 1.433, 95% CI = 0.565-3.635) for those with junior high school education, 2.504 times higher (OR = 2.504, 95% CI = 0.907-6.912) for those with high school/secondary school education, and 2.929 times higher (OR = 2.929, 95% CI = 0.858-9.994) for those with university-level education or above. In terms of disability status, categories of disability were a significant predictor of medication adherence. The odds of having greater medication adherence for those with physical disabilities were lower than the same odds for those with visual disabilities (OR = 0.402, 95% CI = 0.199-0.814; see Table 4).
Ordered Logistic Regression Predicting Medication Adherence Among Disabled People.
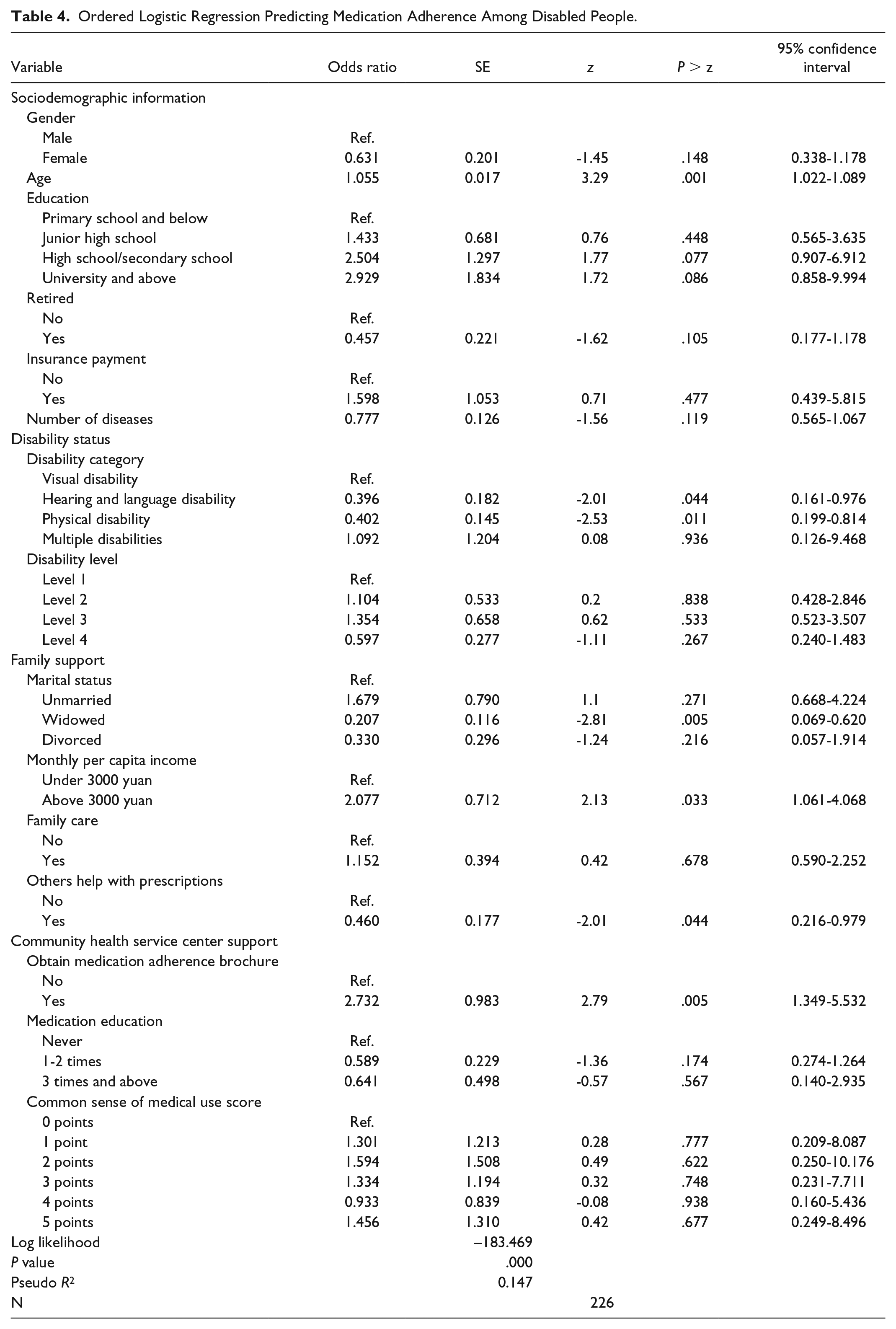
The effects of the family support variables were much stronger. Unmarried people had the highest odds of having greater adherence among the 4 marital status categories: Unmarried people’s odds of having greater adherence were 1.679 times the same odds for married persons (OR = 1.679, 95% CI = 0.668-4.224). Disabled people who were widowed or divorced had the worst adherence: For those who were widowed, the odds of having greater adherence were 79.3% lower than the same odds for married people (OR = 0.207, 95% CI = 0.069-0.620). Family income and family care had positive effects on medication adherence, but the effect of family care was not statistically significant. For family income, the odds of having greater medication adherence were 2.077 times higher among people with disabilities in families with incomes ≥3000 yuan than among those in families with incomes <3000 yuan (OR = 2.077, 95% CI = 1.061-4.068). However, similar to the complicated relationship between marital status and medication adherence, we found a lower odds of having greater adherence among people whose families helped with prescriptions, compared with those without this help (OR = 0.460, 95% CI = 0.216-0.979; see Table 4).
A clearer relationship was found for the role of CHSC in medication adherence. The odds of having greater medication adherence were 2.732 times higher among disabled people who had received a brochure on medication adherence than among those who had not received such a brochure (OR = 2.732, 95% CI = 1.349-5.532). However, no regular pattern was found between medication education and adherence: Those who had never received medication education had better adherence than the other 2 groups. The relationship between the common sense regarding medicine use score and adherence was also unclear (see Table 4).
Discussion
Patients’ medication adherence has received a great deal attention worldwide.28,29 Because of their particular physiological conditions and limited activity, disabled people have a higher susceptibility to disease and are more likely to suffer concurrently from multiple diseases. Medication adherence therefore plays a significant role in the health and survival of people with disabilities. Although low adherence has been reported among disabled people, the reasons for this have not previously been explored. This study used an empirical investigation to explore the medication adherence of disabled people and to further analyze the dominant factors affecting their adherence, paying special attention to family and CHSC support.
Health and Medication Adherence Status
The present study found high morbidity and low adherence. Most (73.89%) of the disabled participants suffered from at least one disease, and only 12.39% had full adherence, whereas 32.30% had full nonadherence. This is far lower than previously reported adherence rates among patients with diabetes (65%-85%), 30 and it is also lower than the average adherence in the United States (50%). The study by Park et al on antihypertensive medication adherence indicated that people with disabilities had lower medication adherence (54.5%) than did their nondisabled counterparts (57.5%). 11 We also explored the reasons for lower adherence among disabled people.
Disability Status and Other Individual Factors
An ordered logistic regression analysis was conducted to explore factors affecting medication adherence among disabled people. We found that age significantly affected adherence, which is consistent with multiple previous studies.31-33 We observed a clear positive association between level of education and medication adherence, which has been repeatedly verified in previous studies.34,35 We also found that people with physical disabilities had poorer adherence, compared with those with other types of disabilities. Previous studies have noted that people with physical disabilities often tolerate high levels of pain,36,37 resulting in lower adherence.
CHSC Support Factors
We found that obtaining a medication adherence brochure was an important variable affecting medication adherence, but the effects of the other examined CHSC support variables (medication education and common sense regarding medicine use score) were not statistically significant. In China, it is difficult for disabled people to obtain medication-related education.31-33 In this context, providing medication adherence–related brochures may be a feasible way to provide medication education for people with disabilities. However, knowledge regarding medicine use, which is a major topic in the strategy to affect behavior through knowledge, was not directly related to medication adherence. In China, CHSCs are increasingly playing a more significant role in health management, and there is therefore a great deal that family doctor teams could do to improve medication adherence among people with disabilities.
Family Support
The present study showed that marriage plays a role in medication adherence that is simultaneously both protective and damaging. Adherence was far lower among widowed and divorced people than among married people, suggesting that a sound marriage may improve medication adherence among disabled people. This is consistent with the results of a study conducted by Dabaghian et al. 16 A related qualitative study of 18 β-thalassemia patients listed “marriage as a facilitator” as one of the 9 factors contributing to medication adherence, and medical personnel participating in the study agreed that marriage can improve adherence to some degree. 17 However, we also found that the odds of having greater adherence were 1.679 times higher among unmarried disabled people, compared with the same odds among married disabled people. Taken together, these results show that marriage plays a role that is simultaneously both protective and damaging. Previous research has shown that most never-married disabled people live with their parents or other family members or are cared for by social welfare agencies. We found that the odds of having greater adherence were 1.152 times higher among disabled people with family care than among those without family care, after controlling for marital status. This indicates that family care plays an important role in promoting adherence among disabled people.
Another complicated finding in the present study was that those whose family members helped with prescriptions had significantly lower adherence than did those without such help. This was an unexpected finding because family aid might be expected to improve medication adherence, as has been suggested by recent studies.34-36 However, our study suggests that family support has various dimensions, and the agreement regarding family support in previous findings may focus on the effect of mental support, rather than other kinds of assistance. This topic merits further research to explain these relationships more fully.
Limitations
The present study had several limitations. The first limitation relates to the focus on study participants with disabilities. Because people with disabilities are difficult to reach for surveys, the sample size in this study was relatively small. Furthermore, because of privacy concerns, we were unable to pursue a more in-depth investigation. Second, the study lacked detailed information on family characteristics and social support (eg, the number of family members, whether the participant lived with their parents, and whether the participant was housed by a social welfare agency). It would be valuable to distinguish differences in effects related to marriage (spouse), other family (especially parents), and social support. Third, our study did not consider mental disability. The special circumstances of individuals with mental disabilities should be considered in further research specifically on this group. Besides, we selected the CHSC support variables according to the practice of CHSCs in Shanghai, which might vary over time. More common variables from fundamental theories were worth exploring.
Conclusion
Support from both CHSCs and family plays an important role in medication adherence for people with disabilities. Marriage was found to be potentially both protective and damaging in terms of medication adherence. Being in a sound marriage is particularly positive, but we found unmarried people to have the best adherence, verifying that family care had a significant effect. The suggestion that some kinds of family support negatively affect medication adherence merits further exploration. The role of CHSC support is clearer: We found that providing brochures was the only effective way to improve medication adherence, which indicates that there is a great deal more that family doctor teams could do to improve medication adherence among people with disabilities.
Footnotes
Acknowledgements
The authors thank the trained investigators from Ouyang Community Health Service Center for visiting the selected disabled people. They especially appreciate the help of the Ouyang Sub-district neighborhood committee officers, who accompanied the investigators to facilitate the successful completion the household survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Natural Science Foundation of China (71403171, 71904145), Shanghai Jiao Tong University China Hospital Development Research Institute 2019 local high-level university hospital management special project (CHDI-2019-C-01), Program for Young Excellent Talents in Pudong New Area Health System (PWRq2016-26), Pudong New Area Health System Leading Personnel Training Program (PWRL2017-05), the Young Medical Talents Training Program of the Pudong Health Bureau of Shanghai (Grant No. PWRq 2016-18).