
Abstract
Additional intervention and medical treatment of complications may follow the primary treatment of a ureteral stone. We investigated the cost of the treatment of ureteral stone(s) within 45 days after initial intervention by means of retrospective analysis of the National Health Insurance Research Database of Taiwan. All patients of ages ≥20 years diagnosed with ureteral stone(s)( International Classification of Diseases, Ninth Revision, Clinical Modification/ICD-9-CM: 592.1) from January 2001 to December 2011 were enrolled. We included a comorbidity code only if the diagnosis appeared in at least 2 separate claims in a patient’s record. Treatment modalities (code) included extracorporeal shock-wave lithotripsy (SWL; 98.51), ureteroscopic lithotripsy (URSL; 56.31), percutaneous nephrolithotripsy (PNL; 55.04), (open) ureterolithotomy (56.20), and laparoscopy (ie, laparoscopic ureterolithotomy; 54.21). There were 28 513 patients with ureteral stones (13 848 men and 14 665 women) in the randomized sample of 1 million patients. The mean cost was 526.4 ± 724.1 United States Dollar (USD). The costs of treatment were significantly increased in patients with comorbidities. The costs of treatment among each primary treatment modalities were 1212.2 ± 627.3, 1146.7 ± 816.8, 2507.4 ± 1333.5, 1533.3 ± 1137.1, 2566.4 ± 2594.3, and 209.8 ± 473.2 USD in the SWL, URSL, PNL, (open) ureterolithotomy, laparoscopy (laparoscopic ureterolithotomy), and conservative treatment group, respectively. In conclusion, URSL was more cost-effective than SWL and PNL as a primary treatment modality for ureteral stone(s) when the possible additional costs within 45 days after the initial operation were included in the calculation.
Keywords
Introduction
Ureteral stone is a common disease worldwide with increasing incidence and prevalence.1,2 Extracorporeal shock-wave lithotripsy (SWL) and ureteroscopic lithotripsy (URSL) are the 2 most common procedures performed to treat ureteral stones in more developed countries. 2 Medical expulsion is applicable when the stone size is relatively small. Other more invasive modalities include percutaneous nephrolithotripsy (PNL) and open or laparoscopic ureterolithotomy. Shock-wave lithotripsy is often an outpatient procedure, whereas URSL may require admission in certain situations. Extracorporeal shock-wave lithotripsy is most efficacious for smaller stones incarcerated in the upper ureter, whereas URSL provides a better stone-free rate for larger or more distal stones.3,4
Many studies have compared the effectiveness between the 2 procedures; however, there are fewer studies on a national level. There are 2 reports from Taiwan. Huang et al 5 used hospital-based records to compare the effectiveness of the 2 treatments and showed that URSL was significantly more effective than shock-wave treatment for upper-third ureteral stones. Chang et al compared treatment effectiveness for distal ureteral stones and showed that URSL was more efficacious than SWL in both cost and success rate. 6 There are additional procedures after primary treatment such as removal of double-J stent, salvage stone removal, and medical treatment of complications, which may alter the cost and initial treatment strategy, but less studies focused on this issue.
We investigated the cost of treating ureteral stone(s) including the cost generated within a 45-day postoperative period by retrospective analysis of the National Health Insurance Research Database of Taiwan. The primary objective of this study is to compare the cost-effectiveness between SWL and URSL on a national level in Taiwan. The secondary outcome is to delineate the relationship between underlying comorbidities and cost.
Methods
Database
This retrospective cohort used a database derived from the National Health Insurance Research Database of Taiwan. The data are a derivative of the National Health Insurance Program of Taiwan that covers more than 99% of the population. The personal data have been scrambled to prevent identification of any individual patients. The Longitudinal Health Insurance Database 2000 (LHID2000) contains the claims filed by 1 million randomized individual patients. The diagnoses were classified by ICD-9-CM. This study was approved by the Institutional Review Board of China Medical University, Taiwan (CMUH104-REC2-115).
All cases diagnosed with ureteral stone(s) (ICD-9-CM: 592.1) from January 2001 to December 2011 were enrolled. The study included all patients aged ≥20 years. Total case number was 28 513. We recorded the treatment methods and related costs from the day of initial intervention to 45 days after the initial treatment. The “cost” mentioned hereafter included that of admission, primary intervention, salvage treatment, and outpatient department follow-up. Baseline comorbidities were recorded as well, including hypertension (HTN; ICD-9-CM: 401-405), diabetes mellitus (DM; ICD-9-CM: 250), and chronic kidney disease (CKD; ICD-9-CM: 585) that might affect the cost ureteral stones. We included a comorbidity code only if the diagnosis appeared in at least 2 separate claims in the patient’s record to avoid inclusion of false diagnoses. Treatment modalities (codes) included SWL (98.51), URSL (56.31), PNL (55.04), ureterolithotomy (56.2), and laparoscopy (54.21). All costs were recorded in United States Dollar (USD; 1 USD ≅ 0.03 New Taiwan Dollar).
Statistical Analyses
All costs were expressed as mean ± standard deviation. A chi-square test was carried out to examine the differences of costs and comorbidities among different groups. A linear regression model was used to examine the costs of treatments, and 95% confidence interval (95% CI) of the variables was calculated for each cohort. Analysis of data was performed by the SAS statistical package (SAS System for Windows; version 9.4). The adopted level of statistical significance was P < .05.
Results
We included a total of 28 513 patients with ureteral stones (13 848 men and 14 665 women). The overall average cost was 526.4 ± 724.1 USD. There was no cost difference among different sex and age groups. The treatment costs were significantly increased in patients with comorbidities including DM, HTN, and CKD (Table 1).
Demography and the Corresponding Medical Costs Within 45 Days After the Primary Treating of Ureteral Stone(s).
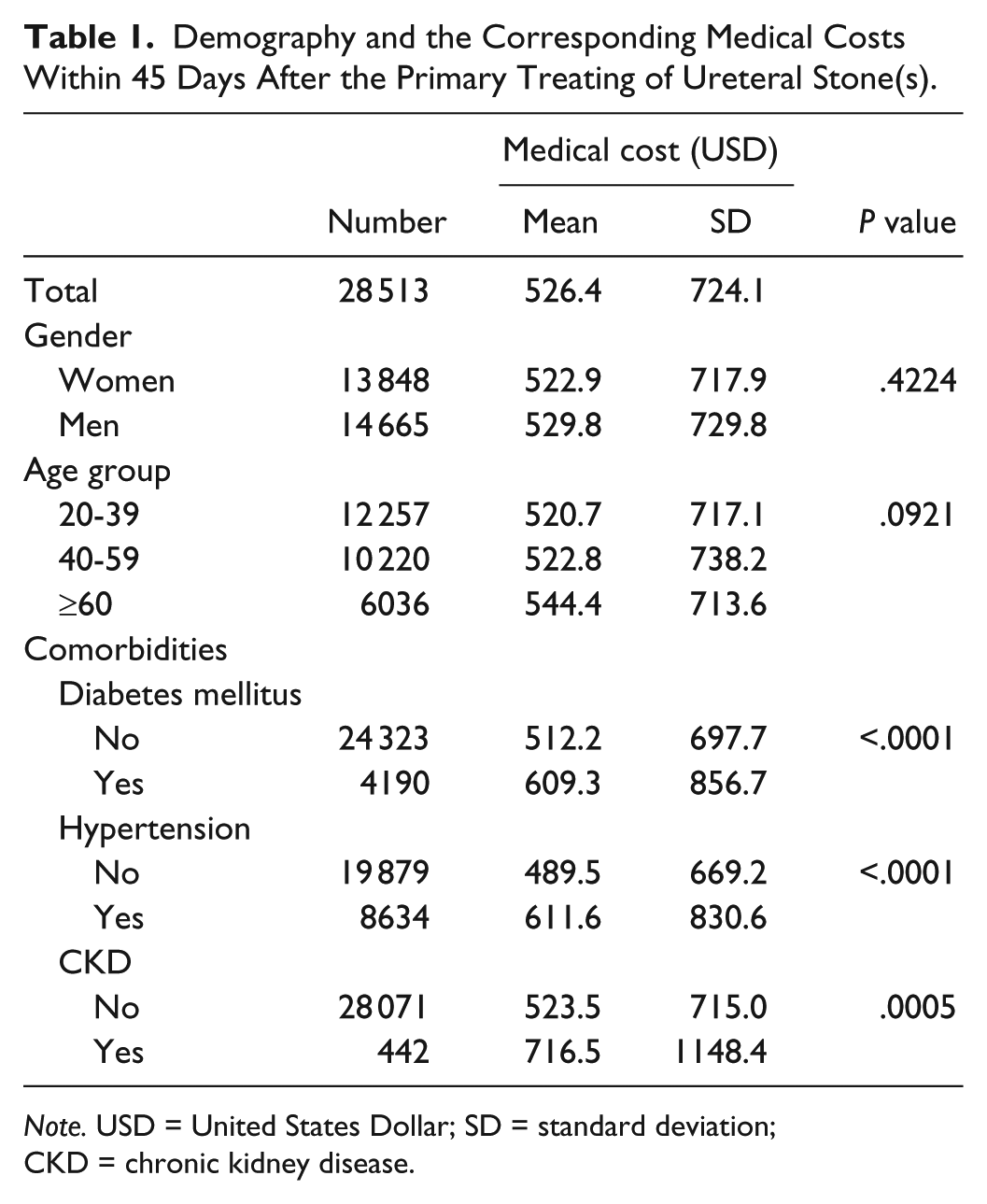
Note. USD = United States Dollar; SD = standard deviation; CKD = chronic kidney disease.
There were 7479 SWLs with an average cost of 1212.2 ± 627.3 USD. The average cost of URSL was 1146.7 ± 816.8 USD in 1374 patients. The average cost of SWL was significantly higher than that of URSL (P < .001). The patients who received URSL incurred the lowest average cost among all groups except conservative management (P < .001). The highest cost was incurred by laparoscopy in 8 patients with a mean of 2507.4 ± 1333.5 USD. Percutaneous nephrolithotripsy is the modality incurring the second highest mean cost of 1533.3 ± 1137.1 USD in 147 patients. Average cost of open ureterolithotomy was 2566.4 ± 2594.3 USD in 127 patients. In the 19 517 patients who did not receive surgery, medical expulsion therapy was most probably prescribed, and the mean cost was 209.8 ± 473.2 USD (Table 2).
The Medical Costs Within 45 Days of the Primary Treatment of Ureteral Stone(s) According to Different Treatment Modalities.
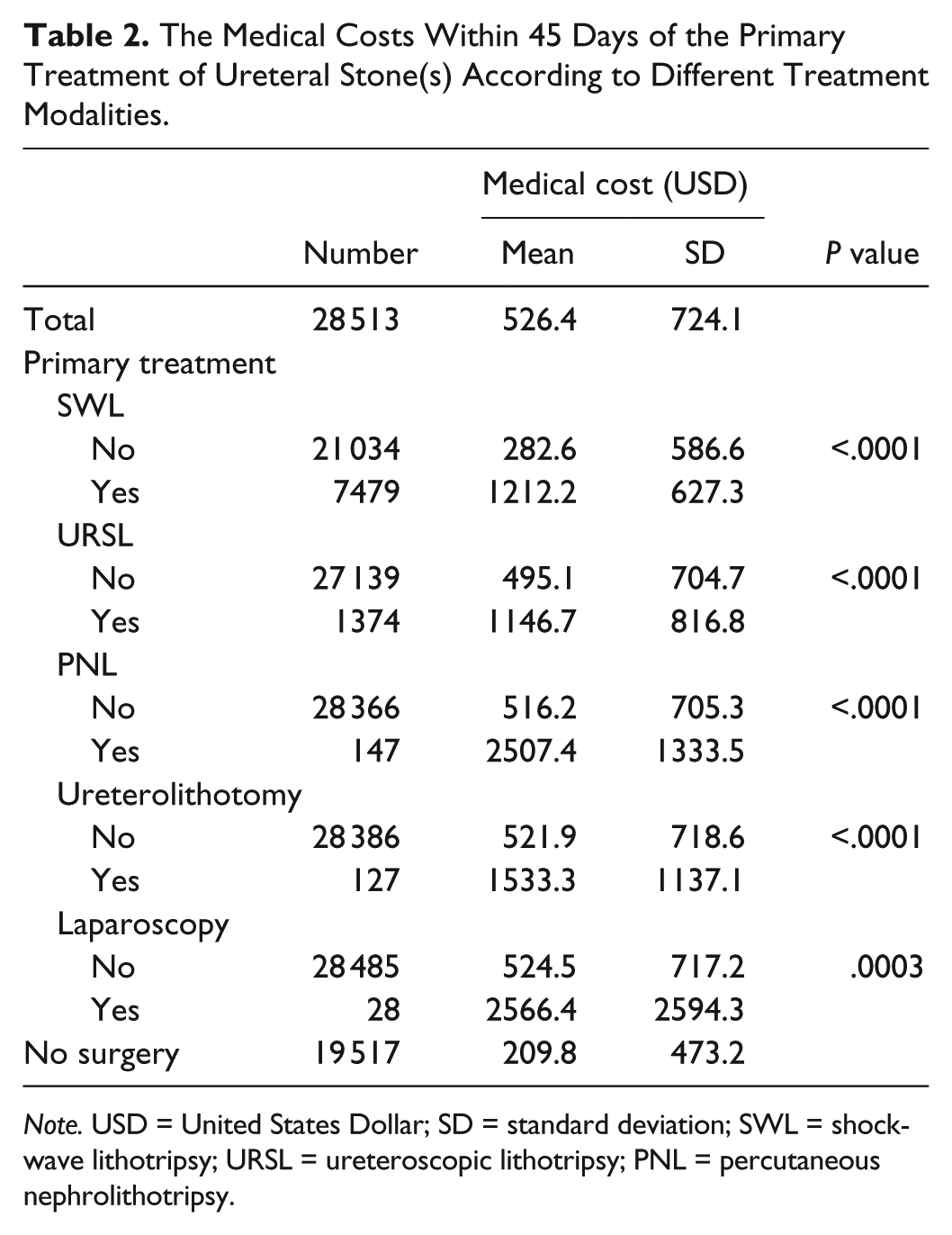
Note. USD = United States Dollar; SD = standard deviation; SWL = shock-wave lithotripsy; URSL = ureteroscopic lithotripsy; PNL = percutaneous nephrolithotripsy.
By comparing the deviation of mean cost from controls between respective comorbidities, we found that DM lead to an increased treatment cost of 36.7 (95% CI, 17.8-55.6) USD when compared with patients without DM. Hypertension increased the mean cost by 68.6 (95% CI, 54.0-83.3) USD. Chronic kidney disease led to an increased cost of 171.8 (95% CI, 120.5-223.0) USD (Table 3). When the group without definite intervention was used as a reference point, the additional medical costs within 45 days of the primary treatment of a ureteral stone by different treatment modalities are shown in Table 4. The additional cost incurred by SWL was 986.9 (95% CI, 972.6-1001.2) USD, whereas that of URSL was 812.3 (95% CI, 782.9-841.7) USD (P < .001).
The Medical Costs Within 45 Days of the Primary Treatment of Ureteral Stone(s) According to Age, Sex, and Comorbidity.

Note. USD = United States Dollar; CI = confidence interval; CKD = chronic kidney disease.
The Additional Medical Costs Within 45 Days of the Primary Treatment of a Ureteral Stone by Different Treatment Modalities Using the Group Without Treatment as a Control Group.

Note. Adjusted R2 = .4466 (the adjusted R2 compares the explanatory power of regression models that contain different numbers of predictors). Estimated mean cost of ESWL = USD 1155.8. Estimated mean cost of URSL = USD 981.2. USD = United States Dollar; CI = confidence interval; SWL = shock-wave lithotripsy; URSL = ureteroscopic lithotripsy; PNL = percutaneous nephrolithotripsy; ESWL = extracorporeal shock-wave lithotripsy.
Discussion
The introduction of SWL decades ago provided urologists and patients with an option to avoid invasive intervention even if a ureter stone would not be able to pass spontaneously. Three decades later, the urologist still has to decide whether to proceed with SWL or URSL when the probability of spontaneous stone passage is low. 6 The European Association of Urology guidelines included both SWL and URSL as standard treatment modalities for ureteral stones, but SWL was favored for proximal stones <10 mm and URSL was favored for distal stones >10 mm. It does acknowledge that whether to proceed with SWL or URSL is not a simple decision, and many factors must be considered. 3 Studies to aid the urologist to make this decision have been performed over the past 20 years.
Earlier retrospective single-center studies compared the cost between SWL and URSL in the treatment of distal ureteral stones and concluded that URSL was more cost-efficient.5,7,8 A retrospective single-centered study of proximal upper urinary tract stones suggested that SWL seemed to be reasonable for renal calculi, but URSL remained the treatment of choice for proximal ureteral stones in terms of cost-effectiveness. 9 In another retrospective single-centered study of patients with proximal ureteral stones, the cost and stone-free rate (SFR) were compared between those who received SWL and URSL with holmium:yttrium-aluminum-garnet (YAG) laser, and concluded that even when the stone burden was larger in the URSL group, URSL proved to be more cost-effective and provided a better SFR than SWL. 5 A more recent study from a regional hospital in Taipei arrived at a similar conclusion, but a pneumatic lithotripter (Swiss LithoClast; EMS, Nyon, Switzerland) was used instead of holmium: YAG laser. 9
Lotan et al 10 reviewed the costs and success rates of observation, URSL and SWL in the treatment of ureteral stones described in the literature, and then constructed a decision tree model using computer software to compare the cost, and found that URSL was more cost-effective than SWL. Matlaga et al 11 reviewed 8 studies that compared the SFR and cost-effectiveness between SWL and URSL for ureteral stones, and showed that URSL was better than SWL in both SFR and cost-effectiveness; however, the review was biased by small study number, heterogeneous data, and research methods. A recent meta-analysis of 10 articles on the treatment of proximal ureteral stones >10 mm concluded that URSL was more clinically effective than SWL, and the associated risks were not significantly higher; however, cost-effectiveness was not included as a variable. 12 Cochrane database published their findings in 2012, stating that URSL achieved a higher SFR but with the cost of increased complication rates and hospital stay. 13 The cost of lithotripters may not differ between studies because of the oligopoly of the international market by a handful of specialized manufacturers, but the financial cost of hospital days may differ greatly among countries.
A prospective randomized study from eastern China found that despite having a higher SFR in treating distal ureteral stones, URSL brought upon more complications than SWL and was associated with a higher cost; however, it is worth noting that the average hospital stays of patients in the SWL and URSL groups were 5.4 and 6.6 days, respectively. 14 The admission days in this study were astonishingly longer than that reported in other countries and may cause discrepancies in cost evaluation. In contrast, another randomized study on proximal ureteral stones compared the SFR and complication rate of laparoscopic ureterolithotomy, SWL, and URSL, and concluded that URSL has a lower complication rate than SWL. 15 The aforementioned study did not evaluate cost-effectiveness.
Even for renal stones, SWL may be less cost-effective than URSL when the stone is less than 15 mm in the greatest length. 16 Cone et al 16 published an article showed the cost-effectiveness comparison of ureteral calculi treated with URSL versus SWL. This retrospective study revealed superior SFR for ureteral stones less than 1.5 cm treated with URSL compared with SWL. Their decision analysis model demonstrated that when SFR for SWL is less than 60% to 64% or is greater than 57% to 76% for URSL, SWL is not a cost-effective treatment option. Based on these findings, they suggested that careful stratification and selection of stone patients may enable surgeons to increase the cost-effectiveness of SWL. To avoid the inclusion of patients without ureteral stones into the study population due to input of incorrect ICD codes, our inclusion criteria included a treatment code that confirms the original diagnosis of ureteral stone in each entry. We calculated the costs of treatment within 45 days instead of documenting a single procedural fee, because secondary procedures may follow an unsatisfactory primary procedure, which may lead to increased costs within that period.
Our study showed that URSL was the most cost-effective treatment of choice for ureteral stones if the calculation included the cost incurred by additional treatment up to 45 days postoperatively. Our results supported the previous study by Huang et al 5 that compared the overall treatment cost during admission among stone treatment modalities, but that study did not include the costs of additional treatment after primary intervention. Huang et al found that the overall treatment cost was higher in the SWL group without reaching statistical significance (USD 627.1 ± 267.3 vs 596.3 ± 143.5). After stratification by the location of the stone(s), the overall treatment cost was significantly higher in the extracorporeal SWL group than in the URSL group for patients with upper-third ureteral stones, irrespective of stone size. Our data also revealed that the cost of SWL is significantly higher than that of URSL (USD 1212.2 ± 627.3 vs 1146.7 ± 816.8) when the costs incurred by postoperative treatment within 45 days of primary intervention were included. In fact, URSL was the least costly primary intervention modality among all the treatment groups when postoperative treatment costs were included in the calculation.
The management of ureteral calculi has evolved over the past decades with the advent of new surgical and medical treatments. The current guidelines support conservative management as a possible approach for ureteral stones sized 10 mm. More recently, Alevizopoulos et al 17 showed that conservative management is clinically effective with a significant cost-benefit, particularly for the subgroup of stones sized 0 to 4 mm, where a need for follow-up scans is in dispute. We separately investigated whether the presence of comorbidities increased the medical costs in patients who received lithotripsy, and the results were significantly positive. Patients with comorbidities have higher medical costs in our study. More complications related to underlying comorbidities may increase cost, but this relationship is more established for PNL.18,19
This is a nation-wide study comprising of data contributed by various health care providers, from clinics to tertiary referral medical centers, unlike the traditional multicenter or multinational study, 20 which limits the number of institutions involved. The sample size is 28 513 patients, larger than previous studies. However, there are several limitations of this study. National Health Insurance Research Database could not provide certain details, such as stone size, location, or stone quantity. The increase in cost may be related to usage of chronic medications but not necessarily complications related to surgery. Therefore, this may be the causes of higher cost in PNL and laparoscopy. However, SWL and URSL might be in a same condition of choice which can be compared. A similar limitation applies to the comparison of treatment modality for different stone sizes.
Conclusions
In conclusion, SWL as the primary treatment for ureter stone was associated with a higher cost when compared with URSL. In terms of cost-effectiveness, URSL is superior to SWL and PNL. Underlying comorbidities increases the overall medical cost during the treatment of ureter stones. More data are needed to delineate the specific parameters that may affect the cost at a national level.
Footnotes
Authors’ Note
The design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, and approval of the manuscript were the sole responsibility of the authors listed and were not influenced by the research’s sponsor. Yung-Hsiang Chen and Wen-Chi Chen contributed equally to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by China Medical University (CMU) Hospital (DMR-105-048); CMU under the Aim for Top University Plan of the Taiwan Ministry of Education (A-5-2-A); Taiwan Ministry of Science and Technology (MOST 104-2320-B-039-016-MY3); Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW105-TDU-B-212-133019); China Medical University Hospital, Academia Sinica Taiwan Biobank, Stroke Biosignature Project (BM10501010037); National Research Program for Biopharmaceuticals Stroke Clinical Trial Consortium (MOST 104-2325-B-039 -005); Tseng-Lien Lin Foundation; Taiwan Brain Disease Foundation; and Katsuzo and Kiyo Aoshima Memorial Funds, Japan.