
Abstract
This study aimed to investigate the association between males with psychosexual disorders (PSDs) and the risk of developing psychiatric disorders. A total of 34,972 enrolled patients, with 8,743 subjects who had suffered from PSD and 26,229 controls (1:3) matched for age and index year, from Taiwan’s Longitudinal Health Insurance Database (LHID) from 2000 to 2015, selected from the National Health Insurance Research Database (NHIRD). After adjusting all the confounding factors, the multivariate Cox regression model was used to compare the risk of developing psychiatric disorders, between the PSD and non-PSD groups, during the 15 years of follow-up. Of the all enrollees, 1,113 in the PSD cohort and 2,611 in the non-PSD cohort (1,180.96 vs. 954.68 per 100,000 person-year) developed psychiatric disorders. Multivariate Cox regression model survival analysis revealed that, after adjusting for gender, age, monthly income, urbanization level, geographic region, and comorbidities, the adjusted hazard ratio (HR) was 2.448 (95% CI [2.227, 2.633], p < .001). PSD has been associated with the increased risk in anxiety disorders, depressive disorders, bipolar disorders, sleep disorders, and psychotic disorders, respectively. Sexual dysfunctions, paraphilia, and gender identity disorders were associated with the overall psychiatric disorders with adjusted HRs as 1.990 (p < .001), 11.622 (p < .001), and 5.472 (p < .001), respectively. Male patients who suffered from PSD have a higher risk of developing psychiatric disorders, and this finding should be considered as a timely reminder for the clinicians to provide much more attention for these patients because of their mental health issues.
Keywords
Psychiatric, or mental disorders, are defined as clinically significant behavioral or psychological syndromes, which are associated with distress, disability, or increased risk of suffering death, pain, or disability, and subsequent behavioral, psychological, or biological dysfunctions (American Psychiatric Association, 1994; Stein et al., 2010). Previous researches have reported that psychiatric morbidity could be associated with other psychiatric disorders, such as neurodevelopmental disorders (Young et al., 2018), substance usage disorders (Cook et al., 2018; Gattamorta, Mena, Ainsley, & Santisteban, 2017), and/or physical diseases (Chien et al., 2017; Hesdorffer, 2016; Pompili et al., 2017; Tzeng, Chang, et al., 2017, 2018; Tzeng, Chung, et al., 2018).
Psychosexual disorders (PSDs) are defined as sexual problems that are psychological in origin and occur in the absence of any pathological disease, which might be categorized as sexual dysfunctions, paraphilias, and gender identity disorders; PSDs could be related to physical, environmental, or psychological factors (American Psychiatric Association, 1994, 2000; Narang, Garima, & Singh, 2016). Sexual dysfunctions, such as sexual pain or to a disturbance in one or more phases of the sexual-response cycle, could result in marked distress or interpersonal difficulty (American Psychiatric Association, 1994, 2000; Sungur & Gündüz, 2014). Paraphilias are recurrent, intense sexually arousing fantasies, sexual urges, or behaviors generally involving nonhuman objects, the suffering or humiliation of oneself or one’s partner, or children or other nonconsenting persons that occur over a period of at least 6 months (American Psychiatric Association, 1994, 2000; McManus, Hargreaves, Rainbow, & Alison, 2013). Gender identity disorder in males is strong and persistent cross-gender identification, with the repeatedly stated desire to be, or the insistence that he or she is the other sex in cross-dressing or simulating female attire (American Psychiatric Association, 1994, 2000; Bower, 2001). PSDs are mutually associated with other psychiatric disorders, for example, the newly diagnosed erectile dysfunction (ED), one of the sexual dysfunctions that has been associated with the risk of depression (P.-S. Chou et al., 2015), and a newly diagnosed major depressive disorder has also been associated with the risk of ED (Huang, Lin, Chan, Loh, & Lan, 2013). Psychiatric disorders could be a consequence of persistent distress in patients with PSD, such as sexual dysfunctions (Waldinger, 2015), paraphilias (McManus et al., 2013), and gender identity disorders (Haraldsen & Dahl, 2000; Smith, Cohen, & Cohen-Kettenis, 2002). Furthermore, psychiatric disorders seem to be important unfavorable prognostic factors for the long-term psychosocial adjustment in these disorders (Bodlund & Kullgren, 1996; McManus et al., 2013; Michel, Ansseau, Legros, Pitchot, & Mormont, 2002; Waldinger, 2015). Therefore, it is important to clarify as to whether PSDs are associated with a range of psychiatric disorders. However, the association between PSDs and a range of psychiatric disorders, including dementia, anxiety disorders, depressive disorders, bipolar disorders, eating disorders, sleep disorders, and psychotic disorders has not, as yet, been studied. A hypothesis was raised that there is an association between PSDs and the risk of psychiatric disorders, and the National Health Insurance Research Database (NHIRD) could be used to conduct a nationwide, population-based study on this topic.
Methods
Data Sources
The present study used the NHIRD to identify the inpatients with a discharge diagnosis of PSD based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes, including sexual dysfunctions (ICD-9-CM codes: 302.7, 607.84), paraphilia (ICD-9-CM codes: 302.1–302.4, 302.8), and gender identity disorders (ICD-9-CM codes: 302.5, 302.6), during 2000–2015. The details of the program have been documented in previous studies (Chien et al., 2017; Tzeng, Chang, et al., 2017, 2018; Tzeng, Chung, et al., 2017, 2018).
In this database, all the personal identification data were encrypted, for the protection of privacy. The National Health Insurance (NHI) Administration randomly reviews the records of ambulatory care visits and inpatient claims periodically to verify the accuracy of the diagnoses (Ministry of Justice, 2014). This study was conducted in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Ethics
The Institutional Review Board of the Tri-Service General Hospital approved this study and waived the need for individual written informed consent since all the personal identification data were encrypted (No. 1-106-05-055).
Study Design and Sampled Participants
This study was of a population-based, matched-cohort design. Patients with newly diagnosed PSDs were selected from the two million Longitudinal Health Insurance Database (LHID) from the index year between January 1, 2000 and December 31, 2015, according to a diagnosis of PSDs, including sexual dysfunctions (ICD-9-CM codes: 302.7, 607.84), paraphilia (ICD-9-CM codes: 302.1–302.4, 302.8), and gender identity disorders (ICD-9-CM codes: 302.5, 302.6). Patients with PSDs before 2000 were excluded. In addition, patients diagnosed with dementia, depressive disorders, anxiety disorders, bipolar disorders, sleep disorders, and psychotic disorders before 2000, or before the first visit for any PSD treatment, were likewise excluded. All patients aged <20 were also excluded. A total of the patients that were enrolled, including 9,303 subjects with PSD and 27,909 controls without PSD, were (1:3) matched for age, gender, and index year, that is, each patient with PSD was randomly matched with three non-PSD controls with the exact age, gender, and the index year. In this study, the validity of several diagnoses in the NHIRD was confirmed (Cheng et al., 2014; I.-C. Chou, Lin, Lin, Sung, & Kao, 2013; Sung et al., 2016).
Covariates
The covariates included gender, age groups (20–49, ≥50 years), marital status, educational levels (<12 years, ≥12 years), seasons, geographical area of residence (north, center, south, and east of Taiwan), urbanization level of residence (levels 1 to 4), monthly income (in New Taiwan Dollars [NT$]; <18,000, 18,000–34,999, ≥35,000), and levels of medical care. The urbanization level of residence was defined according to the population and various indicators of the level of development. Level 1 was defined as a population of >1,250,000, and a specific designation as political, economic, cultural, and metropolitan development. Level 2 was defined as a population between 500,000 and 1,249,999, and as playing an important role in the politics, economy, and culture. Urbanization levels 3 and 4 were defined as a population between 149,999 and 499,999, and <149,999, respectively.
Comorbidity
Comorbidities were assessed using the Charlson Comorbidity Index (CCI), which categorizes comorbidities using the ICD-9-CM codes, scores each comorbidity category (McGrogan, Madle, Seaman, & de Vries, 2009; Sandoglobulin Guillain-Barre Syndrome Trial Group, 1997; van den Berg et al., 2014), and combines all the scores to calculate a single comorbidity score. A score of zero indicates that no comorbidities were found, and higher scores indicate higher comorbidity burdens (Needham, Scales, Laupacis, & Pronovost, 2005).
Outcome Measures
All of the study participants were followed from the index date until the onset of dementia (ICD-9-CM codes: 290.0, 290.10, 290.11, 290.12, 290.13, 290.20, 290.21, 290.3, 290.41, 290.42, 290.43, 290.8, 290.9, and 331.0), anxiety disorders (ICD-9-CM codes: 300), depressive disorders (ICD-9-CM codes: 296.2, 296.3, 300.4, and 311), bipolar disorders (ICD-9-CM codes: 296.0, 296.4–296.8), eating disorders (ICD-9-CM codes: 307.5, anorexia nervosa: 307.1, bulimia nervosa: 307.51; other eating disorders:307.59), sleep disorders (ICD-9-CM codes: 307.4, 780.5), and psychotic disorders (ICD-9-CM codes: 295, 297–298), withdrawal from the NHI program, or the end of 2015.
Statistical Analysis
All statistical analyses were performed using the SPSS for Windows, version 22.0 (IBM Corp., Armonk, NY). Chi-square and t tests were used to evaluate the association between categorical and continuous variables, respectively. Multivariate Cox regression model competing risk analysis was used to determine the risk of psychiatric disorders. The results were presented as a hazard ratio (HR) with a 95% confidence interval (CI). Differences in the risk of psychiatric disorders between the study and control groups were estimated using the Kaplan–Meier method with the log-rank test. A two-tailed p value <.05 was considered to indicate a statistical significance.
Results
Sample Characteristics
There were 8,743 who were diagnosed with PSD, and 26,229 patients without PSD in the control group were included. Demographic statistics and comorbidities are as reported in Table 1, which shows that there was no difference between the PSD and non-PSD cohorts in age, marital status, education, and insured monthly premiums. The PSD cohort had a lower CCI and higher medical visits in summer and autumn than the non-PSD cohort. The PSD cohort also tended to search for medical help in Taiwan during the season of autumn, live in the north, and reside more in the regions of urbanization levels 1 and 2. The PSD group received their medical treatments more in medical centers.
Characteristics of Study at the Baseline.

Note. p = χ2 on category variables and t test on continue variables. Without married = unmarried, divorce, death of spouse, and unknown. CCI_R = Charlson comorbidity index removed dementia.
Table 2 presents the distributions of the sexual dysfunctions, paraphilias, and gender identity disorders, and among these disorders, sexual dysfunctions were more than the other two groups of psychosexual disorders.
Distribution of Psychosexual Disorders.

Kaplan–Meier Model for the Cumulative Risk of Psychiatric Disorders
Of the study subjects, 1,113 in the PSD cohort and 2,611 in the non-PSD cohort (1180.96 vs. 954.68 per 100,000 person-year) developed psychiatric disorders, and the difference was statistically significant in the Kaplan–Meier survival analysis. The Kaplan–Meier analysis revealed that the PSD cohort had a significantly higher 15-year psychiatric disorders cumulative incidence rate than the controls. (log-rank, p < .001, Figure 1).
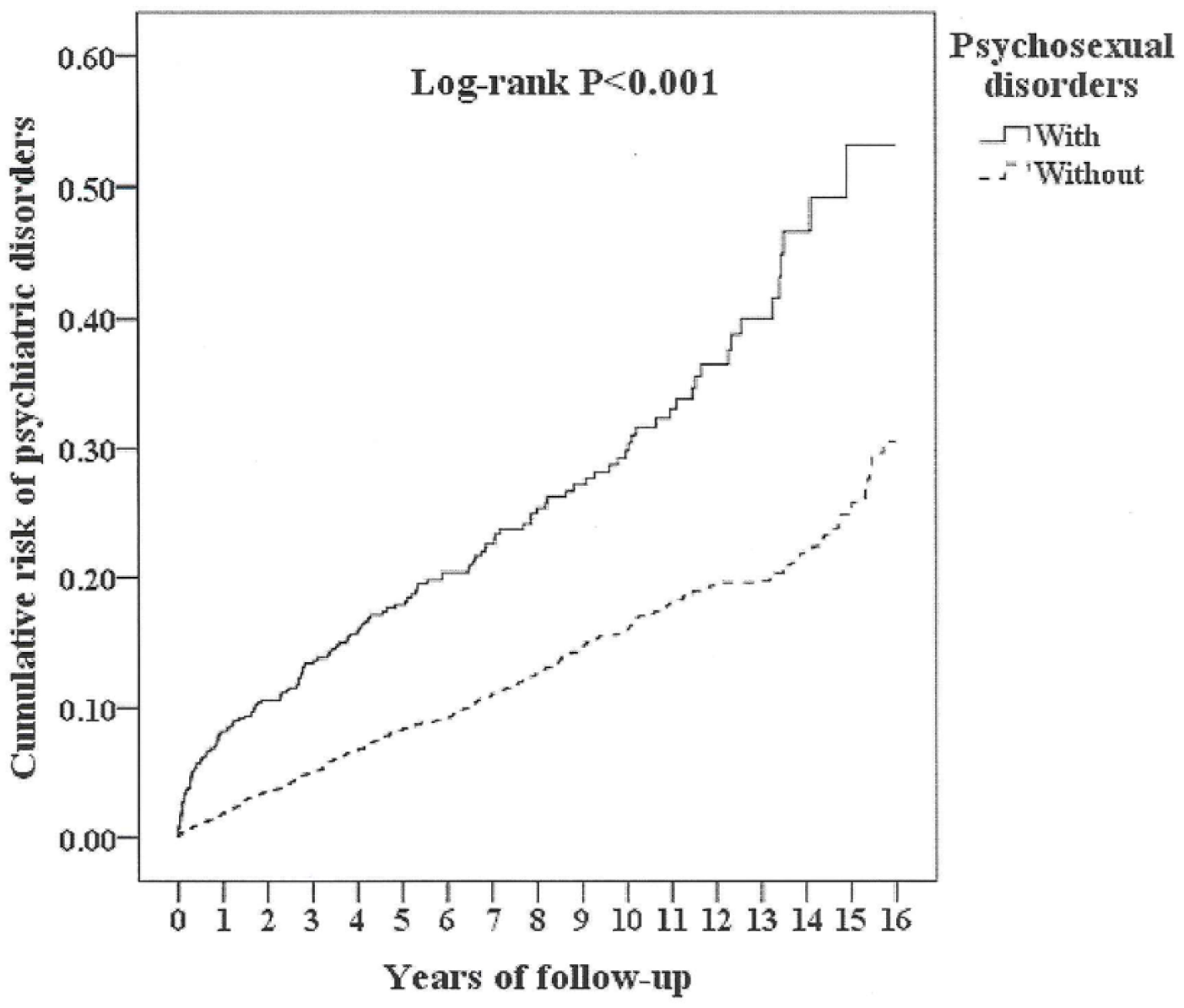
Kaplan–Meier for cumulative incidence of psychiatric disorders aged 20 and over stratified by psychosexual disorders with log-rank test.
Changes of PSD in Male Patients in the Follow-Up Period, 2000–2015
Figure 2 shows the changes of the overall PSD, sexual dysfunctions, paraphilias, and gender identity disorders in males between 2000 and 2015. There was no significance of differences between the beginning and the end point of the follow-up in all these PSD disorders.

Rate and subgroup proportions of psychosexual disorders in study period.
Hazard Ratios Analysis of Psychiatric Disorders in Patients With PSD
Table 3 shows that in the multivariate Cox regression model, the hazard ratio of the PSD cohort in the development of psychiatric disorders was 2.448 (95% CI [2.227, 2.633], p < .001), in comparison to the control group, after adjustment for age, marital status, education, comorbidity (CCI scores), urbanizations/areas of residence, insurance premiums, seasons of visits, and levels of medical facilities. PSD patients aged 20–49 (with the reference of those aged ≥50) and the residence of urbanization levels 1 to 3 (with the reference of level 4) were associated with increased risk of psychiatric disorders. PSD patients who received medical care from the medical centers and regional hospitals were associated with decreased risk of psychiatric disorders, with the reference of patients who received medical care from local hospitals.
Factors of Psychiatric Disorders Stratified by Variables Listed in the Table by Using Cox Regression Model.
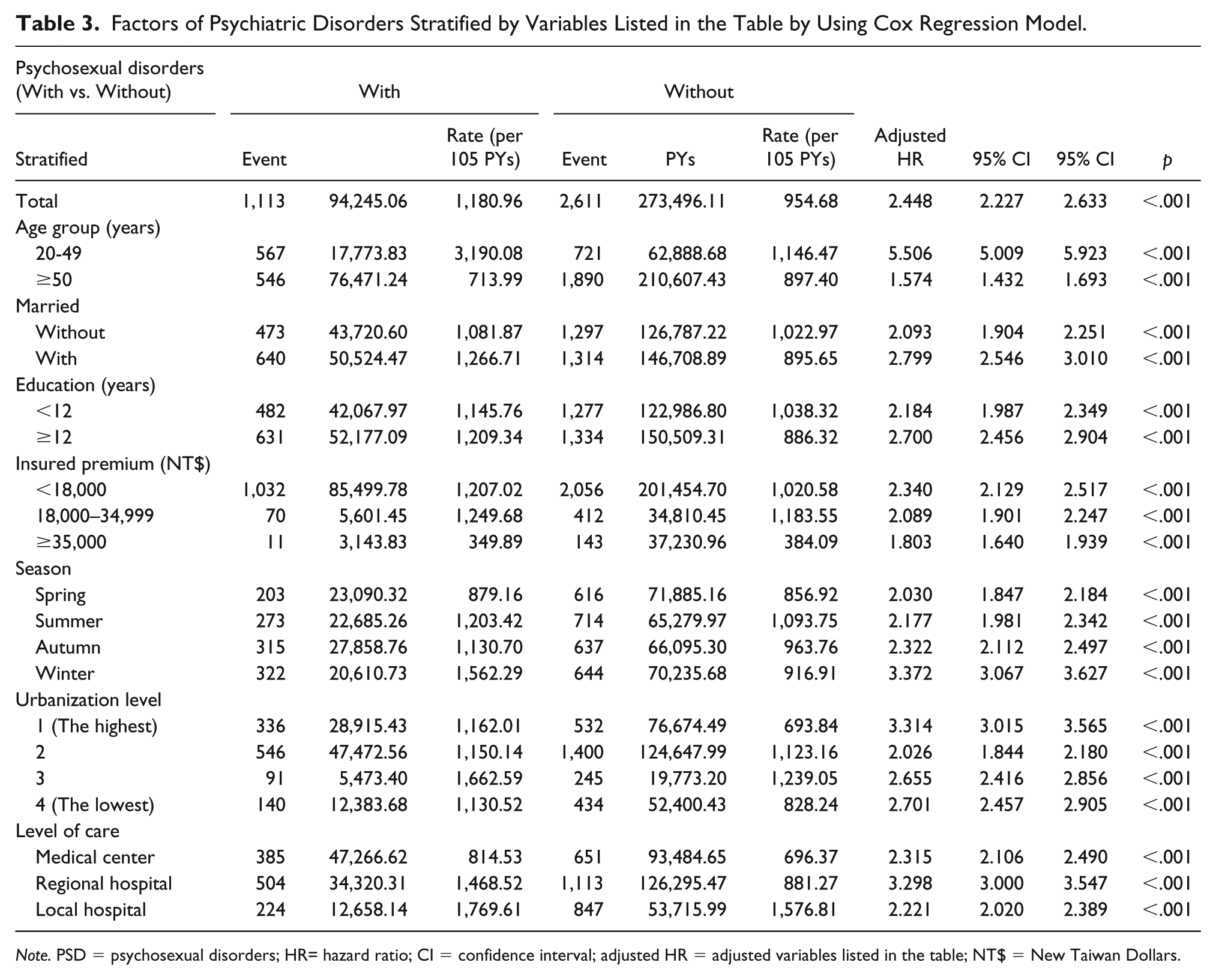
Note. PSD = psychosexual disorders; HR= hazard ratio; CI = confidence interval; adjusted HR = adjusted variables listed in the table; NT$ = New Taiwan Dollars.
Types of Psychiatric Disorders in PSD
Table 4 reveals that the male patients with overall PSD, sexual dysfunction, and paraphilias were associated with an increased risk of developing dementia, anxiety disorders, depressive disorders, bipolar disorders, sleep disorders, and psychotic disorders. Meanwhile, gender identity disorders were associated with anxiety disorders, depressive disorders, bipolar disorders, sleep disorders, and psychotic disorders, but not associated with the risk of dementia. Among the psychiatric disorders, bipolar disorders were at the highest risk in overall PSD, sexual dysfunction, paraphilias, and gender identity disorders.
Factors of Psychiatric Disorders Subgroup Stratified by Psychosexual Disorders Subgroup by Using Cox Regression Model.

Note. Adjusted HR = adjusted hazard ratio: adjusted for the variables listed in Table 1; CI = confidence interval; (No significant association with eating disorders).
Discussion
Association Between PSD and the Risk of Psychiatric Disorders
Even after adjusting for the covariates, the overall adjusted HR was 2.448 (95% CI [2.227, 2.633], p < .001). The male patients with PSD had a nearly 2.4-fold increased risk of developing psychiatric disorders. The Kaplan–Meier analysis revealed that the study subjects had a significantly higher 15-year cumulative risk in the psychiatric disorders rate than the controls. To the best of the authors’ knowledge, this is the first study on the topic of an association between overall PSD and the risk of psychiatric morbidity in male patients.
Comparison of This Study to Previous Literatures
By using this nationwide, population-based dataset, the present study depicted that there was an association between overall PSD and the increased risk in overall psychiatric disorders, dementia, anxiety disorders, depressive disorders, bipolar disorders, sleep disorders, and psychotic disorders. In comparison to the previous studies which found that different types of PSD were associated with the increased risk of different types of psychiatric disorders, such as the associations between ED and depression (P.-S. Chou et al., 2015) or dementia (C.-M. Yang, Shen, Weng, Wang, & Tien, 2015), the present study investigated the association between a range of PSD and psychiatric disorders. However, the present study did not find an association between ED and dementia, although another study has reported an increased risk of dementia in the patients with ED (C.-M. Yang et al., 2015), and further research is needed for clarification as to whether there is an association between PSD and dementia. The discrepancy among these studies, indeed, needs further research.
In the present study, gender identity disorders were associated with the increased risk of overall psychiatric disorders, anxiety, depression, bipolar, sleep and psychotic disorders, respectively. The rates of psychiatric morbidity in the patients with gender identity disorders varied in previous studies: one review has reported that rates of associated psychopathology in children with gender identity disorders are comparable with those in children with other psychiatric disorders (Bradley & Zucker, 1997), and another study showed that a questionnaires survey among the Dutch board-certified psychiatrists revealed that the comorbid personality disorders were reported by 102 (79%) of the 129 psychiatrists, major mood disorders by 34 (26%), dissociative disorders by 34 (26%), and psychotic disorders by 31 (24%) in the patients with gender identity disorders (à Campo, Nijman, Merckelbach, & Evers, 2003; Bradley & Zucker, 1997).
The studies about the association between paraphilias and psychiatric disorders are limited as case reports (Haasen, 2010; Kamalzadeh, Alavi, & Salehi, 2015), and the present study might be the first study on the topic of the association between male paraphilias and the risk of overall psychiatric disorders, and dementia, anxiety, depression, bipolar, sleep and psychotic disorders, respectively.
Possible Mechanisms for the Increased Risk of Psychiatric Disorders in Patients With PSD
Patients with PSD face chronic and heavy stress, in sexual dysfunctions (Lenzi, Lombardo, Salacone, Gandini, & Jannini, 2003), paraphilias (Jahnke, Schmidt, Geradt, & Hoyer, 2015), or gender identity disorders (Gonzalez, Gallego, & Bockting, 2017). Furthermore, chronic stressors would precipitate anxiety disorders (Patriquin & Mathew, 2017), sleep disorders (Hall et al., 2015), and affective disorders (Mayer, Lopez-Duran, Sen, & Abelson, 2018). Besides, posttraumatic stress disorders were associated with sexual dysfunctions in both male and female combat stressed veterans (Breyer et al., 2014; Schnurr et al., 2009), and sexual problems were associated with plasma DHEA and cortisol, urinary catecholamines, and glucocorticoid sensitivity, even when controlling for the effects of comorbid depression (Lehrner et al., 2016). PSD, stress, and psychiatric morbidity might share some links. In the present study, the PSD patients in the residence of higher urbanization were associated with a higher risk of psychiatric disorders, and those that received their medical care from the medical centers and regional hospitals were associated with a lower risk of psychiatric disorders. The socioeconomic levels might also play an important role in the development of psychiatric disorders. For example, previous studies have reported that psychiatric disorders are more common and more complex in the more urbanized areas (Dekker, Peen, Koelen, Smit, & Schoevers, 2008; Peen et al., 2007). The underlying mechanisms between the association of PSD and the risk of psychiatric morbidity need more studies.
Limitations
The present study has several limitations that warrant consideration. First, similar to previous studies using the NHIRD on psychosexual disorders (Chen, Liang, Lin, Liao, & Kao, 2016; Hou et al., 2018; Liu, Lee, & Chung, 2015; Y.-J. Yang et al., 2018), not all of the data were recorded in the NHIRD, and it was unable to evaluate the severity, weakness severity, laboratory parameters, or psychological assessments in the PSD patients. Second, other factors, such as genetic, psychosocial, and environmental factors, were not included in the dataset.
Conclusion
Male patients who suffer from PSD have a higher risk of developing psychiatric disorders, and this finding should serve as a timely reminder for clinicians to provide much more attention for these patients because of their mental health issues.
Footnotes
Acknowledgements
The authors appreciate San-Yuan Huang, MD, PhD, Chin-Bin Yeh, MD, PhD, Ru-Band-Lu, MD, and Yu-Ching Chou, PhD, for their help in inspiration, guidance, and initial proofreading.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by The Program for Promoting Teaching Excellence Universities, the Ministry of Education (NDMC 104-106: I2-4), the Medical Affairs Bureau, Ministry of Defense (MAB-107-084), and the Tri-Service General Hospital Foundation (TSGH-C107-004, TSGH-C107-106, TSGH-C108-003, and TSGH-C108-151).