
Abstract
Traditional Chinese herbal medicine (CHM), which is widely used to treat pain and urolithiasis, is a promising therapy for urinary stone prevention. This study investigated the clinical efficacy of a popular CHM, Wu-Ling-San (WLS), in Taiwan for the prophylaxis of recurrent nephrolithiasis as assessed by surgical stone treatment via a nationwide population-based cohort study. The National Health Insurance Research Database, 2000–2010, which included one million patient records. All patients diagnosed with stone disease at the beginning of the study. The matched controls (4-fold the number of WLS patients) were stone patients who did not take WLS. Data analysis included the stone surgeries following the first treatment. We enrolled 11 900 patients with stone disease, and the incidence of stone patients in this database was 1.19%. The prevalence of comorbidities such as benign prostate hyperplasia, chronic kidney disease, diabetes mellitus, and urinary tract infection, but not hypertension, was significantly higher in WLS users. Several patients in both groups were prescribed potassium citrate. The stone treatment rate was significantly higher in WLS users (17.85%) than in the non-WLS users (14.47%). WLS users with an associated comorbidity had a higher treatment rate than the non-WLS users: 21.05% versus 16.70%, respectively. The surgery rate for upper urinary tract stones was higher in WLS users than in the non-WLS users (adjusted hazard ratio, 1.28; 95% confidence interval, 1.08-1.52; P < .05). The stone treatment rate (52.79%) was significantly higher in patients who used a very high amount of WLS (adjusted hazard ratio, 3.02; 95% confidence interval, 2.30-3.98). Stone patients using a high amount of WLS use had a high stone surgical rate. Long-term therapy with WLS did not have a preventive effect on stone surgical treatment. Long-term potassium citrate therapy as a preventive measure appeared to be underutilized in this study.
Keywords
Introduction
Many complementary and alternative medicine (CAM) practices have emphasized health promotion; however, this has not been the focus of the bulk of CAM research.1,2 CAM practitioners could be seen as a public health resource to increase the population’s access to certain clinical preventive services.3-6 Urolithiasis is a common condition for which the prevalence varies according to sex and age.7-9 In the US population, the reported prevalence of a history of kidney stones is 10.6% in men and 7.1% in women.10,11 The overall prevalence has increased from 3.8% to 8.8% (in past three decades).10-12 Epidemiologically, urinary stone disease accounted for 9.6% of the total population of Taiwan in 2001. 13 Furthermore, this condition accounted for a high proportion of medical visits, with an overall age-adjusted prevalence of 7.35% (5.77% in women and 8.97% in men) in 2010. Huang et al 14 reported the overall recurrence rate (a new episode within a 180-day interval) at 1 and 5 years as 6.12% and 34.71%, respectively. Uribarri et al 15 reported a similar recurrence rate of 35% within 5 years. Therefore, medical treatments such as potassium citrate are provided to prevent the recurrence of urinary stones. 16
Traditional Chinese herbal medicine (CHM) is widely accepted by Taiwanese and Chinese societies and elsewhere. 17 In a previous laboratory and clinical study, we reported the effects of the Wu-Ling-San (WLS) formula on the prevention of recurrent calcium oxalate nephrolithiasis. The WLS formula effectively inhibited the process of calcium oxalate nucleation, crystallization, and aggregation in vitro and in vivo. In a small short-term randomized control trial, WLS increased urine output without serious adverse effects in comparison with a control group.18-20 However, long-term clinical experience with WLS use as a preventive formula is lacking. 21 The effectiveness of WLS should be further confirmed in a large population in a long-term clinical study. Recently, a nationwide population-based study that enrolled a large population of patients was conducted in Taiwan for stone disease, and this study enabled us to perform a survey to investigate the clinical usage of the WLS formula to prevent recurrent stone as assessed by stone surgery in Taiwan. 14 By utilizing these nationwide data, we were able to elucidate the clinical effect of the WLS formula in the prevention of stone recurrence.
Methods
Database
Claimed data from the National Health Insurance Research Database (NHIRD) were used in this study. The data were obtained from the health care information of > 96% of all medical claims in Taiwan since 1996. The medical services provided by the NHI program included both Western and traditional medicine as well as outpatient care, inpatient care, physical therapy, dental services, prescription drugs, medical institution services, and registration files with scrambled identifications.
Representative data between 2000 and 2010 were randomly obtained from the claims dataset of a sample of 1 million enrolled from the entire insured population in the NHI program base (Database, LHID2000). The diagnosis codes from the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) were used in the database. The NHIRD was previously described in detail. 22 This study was approved by the Institutional Review Board of China Medical University (CMUH104-REC2-115), Taiwan.
Study Sample
For the study cohort, we selected patients newly diagnosed with a urinary tract stone (ICD-9-CM codes 592 and 59 993) between January 1, 2000, and December 31, 2010. Patients who were aged ≤ 20 years (n = 1391), received WLS before the renal stone (n = 3046), had a history of malignancy (986, ICD-9-CM 140-208), or had undergone surgery (n = 15 158) were excluded. In this case-control study, the case group patients received WLS and the treatment date was defined as the index date. In the control group, 4 controls each are frequency matched with each individual case patient according to age (every 5 years), gender, study-year, and index-year. Finally, we identified a total of 11 900 patients with stone disease. Patients who took WLS were further divided into low (<5 g/y), medium (5-11 g/y), high (11-43 g/y), and very high (≥44 g/y) users to compare the dose effect. Furthermore, we evaluated comorbidities (might affect the incidence of urethral stones) such as hypertension, 23 benign prostate hyperplasia, 24 gout, chronic kidney disease, urinary tract infection, and diabetes mellitus 25 as well as patients who took potassium citrate as a preventive treatment in both groups.
Surgery following stone disease was defined as any surgery for a stone 180 days after the first diagnosis of stone disease. The surgery codes were 55.0, 56, 57, 58, and 98.51 (Table 1). Both study cohorts were followed up until the last date in the database (the end of 2010). We searched the database for stone treatment and calculated the total treatments in each patient.
ICD-9 Codes for Stone Surgeries.

Source. 2014 ICD-9-CM.
Note. ICD-9 = International Classification of Diseases, Ninth Revision.
Statistical Analyses
Chi-square test was used to examine the differences in the distribution of sociodemographic factors and comorbidities between the cohorts with and without WLS use. Person-years of follow-up duration were calculated for each individual until the end of the database period. A Poisson regression model was used to examine the incidence of following stone treatment, and the 95% confidence interval (CI) of stone treatment with categorical variables was calculated for each cohort. Multivariate Cox proportional hazard models were used to estimate the hazard ratio (HR) and 95% CI for factors associated with comorbidity such as age, gender, hypertension, diabetes mellitus (DM), gout, chronic kidney disease (CKD), benign prostatic hyperplasia (BPH), and urinary tract infection (UTI). All analyses were performed by using the SAS statistical package (SAS System for Windows, Version 9.4) with the statistical significance level set at .05.
Results
We identified 2382 patients who used WLS and 9518 patients for the non-WLS group. Therefore, the incidence of stone patients in this database was 1.19% (11 900/1 000 000). The demographic analysis between WLS users and the non-WLS users revealed no significant difference in gender and age. The mean age was 49.1 years in both groups. The WLS-user group comprised 1213 men and 1169 women and the non-WLS users comprised 4846 men and 4672 women. The ratios of the following comorbidities were significantly higher in WLS users: benign prostate hyperplasia, chronic kidney disease, diabetes mellitus, and urinary tract infection (P < .0001). Urinary tract infection was the most common comorbidity in the WLS group, occurring in 1031 patients. The comorbidity of hypertension was not significantly different between the 2 groups (Table 2). Few stone patients were prescribed potassium citrate in both groups. Although WLS users had a higher ratio of potassium citrate use than the non-WLS users, only 1.22% potassium citrate users were identified in the population.
Demographics Between WLS Users and Non-WLS Users.

Note. Chi-square test and at test. WLS = Wu-Ling-San; BPH = benign prostatic hyperplasia; CKD = chronic kidney disease; UTI = urinary tract infection; DM = diabetes mellitus.
The incidence of stone treatments used in both groups during the follow-up period is shown in Table 3. Overall, the incidence of stone treatment was higher in WLS users (17.85%) than in the non-WLS users (14.47%) during the follow-up period (crude HR, 1.23; 95% CI, 1.04-1.46; P < .05). Men had a higher stone treatment rate than women, regardless of grouping (585 vs 179 patients, respectively). Stone surgery was higher in patients with a comorbidity overall in both groups. The treatment rate in patients with an associated comorbidity was higher in WLS users (21.05%) than in the non-WLS users (16.70%) (adjusted HR, 1.25; 95% CI, 1.03-1.52; P < .01). However, this difference was not significant after adjusting for several factors (age, gender, hypertension, DM, BPH, gout, CKD, UTI, and potassium citrate user; HR, 1.25; 95% CI, 1.03-1.52). A weak association of increasing stone treatment in stone patients who used WLS was observed in the age distribution. Surgery for upper urinary tract stones was higher in WLS users than in the non-WLS users (adjusted HR, 1.28; 95% CI, 1.08-1.52; P < .05). In contrast, WLS users had a lower incidence of operations when the stone was located in the lower urinary tract (7.29 vs 13.53%, respectively). However, the number of cases was limited to 474 in WLS users (Table 4).
Incidence for Operation Between WLS Users and Non-WLS Users.
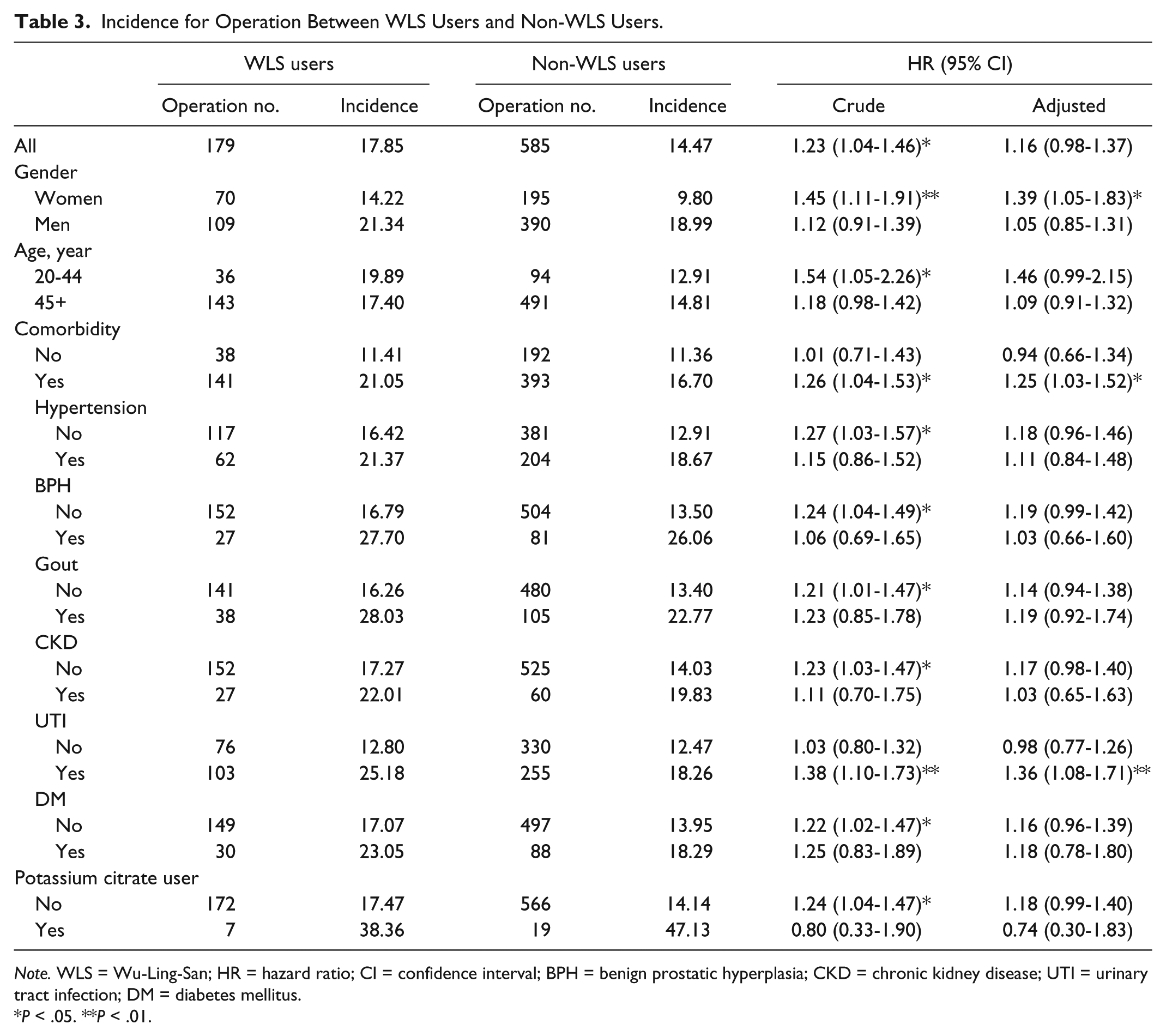
Note. WLS = Wu-Ling-San; HR = hazard ratio; CI = confidence interval; BPH = benign prostatic hyperplasia; CKD = chronic kidney disease; UTI = urinary tract infection; DM = diabetes mellitus.
P < .05. **P < .01.
Incidence for Operation Between WLS Users and Non-WLS Users by Stone Location.
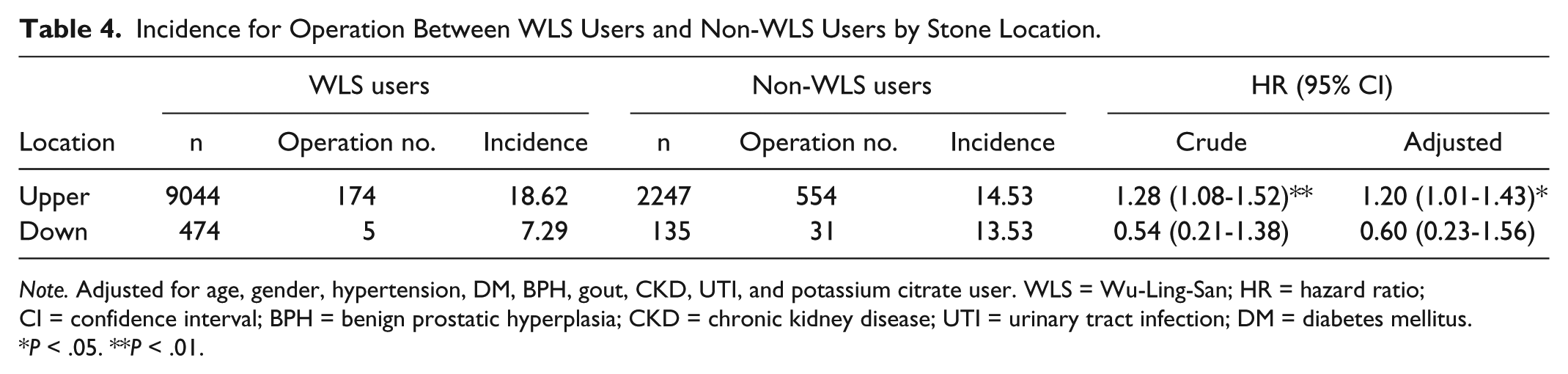
Note. Adjusted for age, gender, hypertension, DM, BPH, gout, CKD, UTI, and potassium citrate user. WLS = Wu-Ling-San; HR = hazard ratio; CI = confidence interval; BPH = benign prostatic hyperplasia; CKD = chronic kidney disease; UTI = urinary tract infection; DM = diabetes mellitus.
P < .05. **P < .01.
As shown in Table 5, patients in the very high WLS group had a significantly higher stone treatment rate (52.79%; adjusted HR, 3.02; 95% CI, 2.30-3.98; P < .0001).
Incidence for Operation Among WLS Usage.
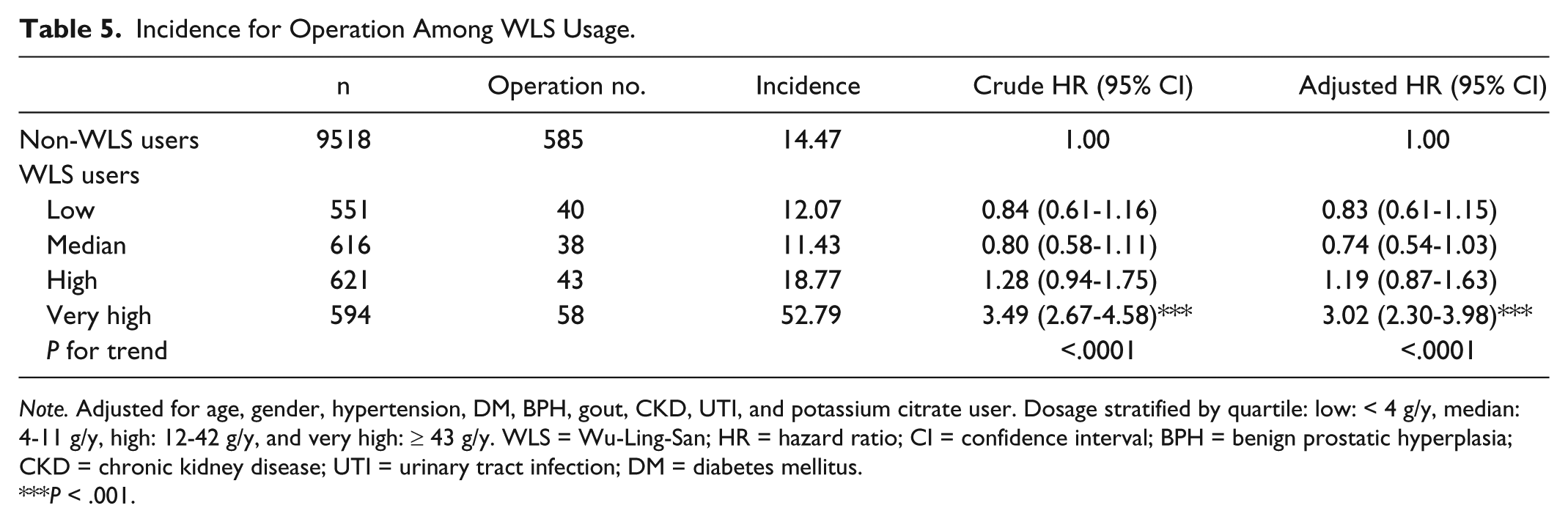
Note. Adjusted for age, gender, hypertension, DM, BPH, gout, CKD, UTI, and potassium citrate user. Dosage stratified by quartile: low: < 4 g/y, median: 4-11 g/y, high: 12-42 g/y, and very high: ≥ 43 g/y. WLS = Wu-Ling-San; HR = hazard ratio; CI = confidence interval; BPH = benign prostatic hyperplasia; CKD = chronic kidney disease; UTI = urinary tract infection; DM = diabetes mellitus.
P < .001.
Discussion
The comparison between WLS users and non-WLS users revealed that long-term WLS use in stone patients did not have a preventive effect on subsequent stone surgery in this study. No difference was observed between WLS users and the non-WLS users among stone patients without comorbidities. Increased stone treatment was observed in stone patients who used WLS compared with non-users, but this difference was not significant if the WLS user took less than 43 g of WLS per year. The stone treatment rate was notably increased in very high WLS users regardless of the clinical comorbidity. The effect of stone expulsion was not included in this study.
Several comorbidities were found to be associated with stone disease in this study. Patients with comorbidities such as hypertension, gout, benign prostate hyperplasia, chronic kidney disease, diabetes mellitus, and urinary tract infection were enrolled. Overall, the ratio of stone patients with comorbidities was significantly higher in WLS users (22.7%) than in the non-WLS users. We propose that stone patients with comorbidities may be more likely to seek further treatment, or that these patients may have taken WLS for other conditions in addition to stone disease. However, no statistically significant difference in the rate of further stone treatment was observed between the 2 groups without comorbidities. Therefore, WLS might not have a preventive effect in patients without comorbidity.
The WLS formula is mainly used to treat uremia and dropsy and to promote urination in traditional Chinese medicine. According to the first recorded use of WLS “Shang Han Lun” (Treatise of Cold-induced Disorders), written by Zhong-Jing Zhang, WLS was commonly used for the treatment of urinary tract disorders. Therefore, it is understandable that we found a high rate of this comorbidity in the group of WLS users. Based on this information, we presume that the original use of WLS was not for the treatment of stone disease. The first recorded use of WLS to treat stone disease was found in the book of “Zheng Zhi Zhun Sheng” (Standards of Patterns and Treatment), written by Ken-Tang Wang in the Ming Dynasty (later 16th century). However, we could not elucidate the number of WLS users who were prescribed this agent for the treatment of stone disease in the current database.
Recently, Siener et al 26 investigated oxalate content in herbal remedies and dietary supplements based on plant extracts. Urinary oxalate excretion is directly related to the amount of oral intake and intestinal absorption rate of oxalate. They evaluated the possibility of increasing oxalate ingestion, which could lead to secondary hyperoxaluria, associated with the intake of herbal remedies and dietary supplements containing plant extracts. Their results showed remarkable differences in oxalate contents of the extracts. The selected herbal remedies and dietary supplements containing plant extracts represent only a low risk for calcium oxalate stone formers, if the recommended daily dose is not exceeded.
A number of herbal extracts and remedies have been tested in vitro or in preclinical in vivo models to assess their activity as chemolytic agents, or as agents preventing new stone formation. A number of clinical studies have also been performed to investigate the efficacy of various herbal remedies in the primary/secondary management of urolithiasis. More recently, Monti et al analyzed the clinical evidence on the efficacy of phytotherapy in the treatment of calculi in the urinary tract. They found that citrate is more effective than phytotherapy in decreasing the size of existing calculi in the urinary tract and in decreasing the urinary excretion rate of uric acid. 27 We previously conducted a pilot study on the use of WLS for calcium oxalate stone prevention. 20 The urine amount was increased slightly in this study, which included a small number of cases with short-term follow-up. However, these results could not predict its long-term effect on stone recurrence.
The incidence of stone patients in this case-control study was 1.19%, which is very similar to the rate of 1.2% to 1.3% reported in a previous population-based study by Huang et al. 14 Our value might have been lower than that of the previous study because of our exclusion criteria. We excluded patients who were less than 20 years of age, who had previously used WLS, and who had a malignancy, whereas Huang et al did not exclude any comorbidity. Therefore, this may explain the differences in the incidence between these 2 studies.
Potassium citrate has a well-known and documented role as a major preventive drug.28-30 In a retrospective cohort study of long-term potassium citrate use in stone patients by Robinson et al, 30 the stone formation rate was significantly (93%) decreased after the initiation of potassium citrate therapy. Potassium citrate may produce a short-term high citraturic state and a long-term change in urinary metabolic profiles.31,32 These authors confirmed that potassium citrate therapy for as long as 14 years was useful in patients with recurrent nephrolithiasis. However, few patients took potassium citrate as a preventive measure against stone recurrence in both groups in this study. In addition, the finding of increased medical demands in the analysis of Huang et al 14 indicated that stone recurrence was increased in their analyzed patients. Therefore, medical treatments for stone recurrence were not decreased in their report. The long-term use of oral drugs is inconvenient for patients and carries the risk of potential side effects. Therefore, recurrence of stone disease is likely in these patients, necessitating treatment and resulting in increased medical costs.33-35 We could not determine the benefit of potassium citrate in this study because of the small numbers of patients and prescriptions for this therapy.
This study had several limitations. First, the information regarding risk factors for recurrence was not clear for the patients in this study. The recurrence rate may be higher for patients with risks factors such as metabolic disorders, positive family history, or hyperuricosuria and hypercalcemia.36,37 Therefore, patients with a higher recurrent rate may have a stronger desire to seek preventive treatment than would patients with a lower recurrent rate. Second, we studied the code only for invasive treatment of stone patients as a surrogate for stone recurrence. Third, our results disagree with previous in vitro and in vivo studies for WLS. The explanations for these differences include the use of different species in various studies, the difference between the well-controlled atmosphere of the laboratory versus a population-based study, the fact that this was a short-term trial that excluded other systemic disorders, the fact that nationwide data are obtained from various doctors ranging from medical centers to local clinics, and the fact that patients may have been treated with WLS for other chronic illness such as chronic kidney disease and lower urinary tract symptoms rather than for stones. Fourth, we were not able to assess whether the long-term use of WLS has a preventive effect on stone recurrence because we had a small number of cases and this was a short-term randomized control trial. Finally, the stone expulsion effect of WLS was not considered in this study.
Conclusions
In traditional CHM, the WLS formula is widely used to treat several disorders such as stone disease, hypertension, gout, chronic kidney disease, urinary tract infection, and diabetes mellitus. The stone surgical rate was high in stone patients who used a high amount of WLS. No statistical difference was observed between WLS users and the non-WLS users in stone patients without comorbidities. Nevertheless, long-term therapy with WLS did not have a preventive effect on the stone surgical treatment in stone patients. A large-scale clinical study of WLS is warranted to elucidate the confounding factors.
Footnotes
Authors’ Note
The design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, and approval of the manuscript were the sole responsibility of the authors listed and were not influenced by the research’s sponsor. Yung-Hsiang Chen and Wen-Chi Chen contributed equally to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by China Medical University (CMU) Hospital (DMR-106-064); CMU under the Aim for Top University Plan of the Taiwan Ministry of Education; Taiwan Ministry of Science and Technology (MOST104-2320-B-039-016-MY3); Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW105-TDU-B-212-133019); China Medical University Hospital, Academia Sinica Taiwan Biobank, Stroke Biosignature Project (BM10501010037); National Research Program for Biopharmaceuticals Stroke Clinical Trial Consortium (MOST105-2325-B-039-003); Tseng-Lien Lin Foundation; Taiwan Brain Disease Foundation; and Katsuzo and Kiyo Aoshima Memorial Funds, Japan.