
Abstract
Objective
Peripancreatic arterial aneurysms (PAAs) are rare but associated with a high risk of rupture and significant mortality. This study aims to evaluate the safety and efficacy of endovascular management for PAAs, focusing on technical strategies and midterm outcomes.
Methods
A single-center retrospective analysis was conducted on a study cohort of 26 patients with PAAs treated consecutively between June 2014 and March 2025. Endovascular therapy was prioritized, with open repair reserved for anatomically complex cases. Technical success, procedural details, and follow-up outcomes were analyzed.
Results
Among 29 aneurysms in 26 patients, 15 were located at the gastroduodenal artery–superior pancreaticoduodenal artery (GDA-SPDA) and 14 were at the superior mesenteric artery–inferior pancreaticoduodenal artery (SMA-IPDA). Endovascular therapy achieved primary technical success in 88.5% of cases. Two patients failed endovascular access via both the CA and SMA. Another had a vascular variant creating a high risk of splenic ischemia upon embolization, and a fourth had an aneurysm involving critical duodenal branches. Three of these four patients underwent successful open surgical repair. Sac-only embolization was performed in 63.6% of cases to preserve collateral flow. Access routes were largely determined by aneurysm location, with SMA for SMA-IPDA aneurysms and celiac artery (CA) for GDA-SPDA aneurysms (p < 0.001). Concomitant celiac revascularization was avoided in most cases. At a median follow-up of 48 months, aneurysm recurrence and restenosis rates were 4.0% each, with no coil migrations or ischemic complications.
Conclusion
Tailored endovascular strategies guided by aneurysm anatomy and collateral circulation yield high technical success and favorable midterm outcomes without routine celiac revascularization. Endovascular therapy is a safe and effective first-line approach for PAAs, with open repair reserved for complex anatomies.
Keywords
Introduction
Peripancreatic arterial aneurysms (PAAs), mostly including pancreaticoduodenal (PDA) and gastroduodenal artery (GDA) aneurysms, are rare but clinically significant vascular lesions, accounting for 2%–3% of all visceral artery aneurysms.1,2 Despite their low incidence, PAAs carry a substantial risk of rupture, with reported mortality rates ranging from 20% to 50%.3,4 Unlike other visceral aneurysms, PAAs exhibit a size-independent rupture risk, with documented cases of rupture occurring even in aneurysms smaller than 10 mm.5,6 This unpredictable behavior underscores the importance of early intervention, as emphasized by the recent European Society for Vascular Surgery (ESVS) guidelines, which recommend treatment of PAA with a diameter more than 15 mm. 7
Pseudoaneurysms are associated mostly with pancreatitis and pancreatic surgery. 8 The etiology of true PAAs is closely linked to hemodynamic stress secondary to celiac axis stenosis or occlusion (i.e. the Sutton-Kadir syndrome), often caused by median arcuate ligament compression, atherosclerotic stenosis, fibromuscular dysplasia, or other etiologies.9,10 In these cases, increased collateral flow through the pancreaticoduodenal arcades leads to altered wall shear level, arterial wall degeneration and aneurysm formation.11,12 Endovascular therapy has emerged as the preferred treatment due to its minimally invasive nature and lower morbidity compared to open surgery. Nevertheless the need for concomitant celiac trunk revascularization remains a subject of debate.13,14 Some advocate for flow restoration to reduce collateral stress, 15 whereas others argue that embolization alone suffices given the robust collateral network.15,16
Recent studies have demonstrated high technical success rates with endovascular management, especially trans arterial embolization (TAE) of the aneurysm.6,16,17 However, questions remain about long-term durability, particularly regarding aneurysm recurrence or the development of new aneurysms in untreated high-flow collateral systems.13,18 Additionally, the optimal embolization technique—whether sac packing, proximal-distal occlusion (“sandwich” technique), or a combination—requires further refinement to balance efficacy and procedural complexity. Open surgical repair provides an alternative approach for anatomically complex cases such as hypoplastic CA, multiple aneurysms, or cases with challenging endovascular access (e.g. tortuous branch anatomy or combined severe CA and SMA stenosis).13,19,20
This study presents our single-center experience with management of PAAs, focusing on clinical outcomes, technical strategies, and the role of selective embolization without routine celiac revascularization. By analyzing a cohort of patients treated over 10 years, we aim to contribute to the growing evidence supporting endovascular therapy as a safe and effective first-line approach for PAAs, while highlighting the importance of individualized treatment based on aneurysm anatomy and collateral circulation.
Methods
Study design and population
This retrospective cohort study included patients consecutively admitted to the Department of Vascular Surgery at Peking Union Medical College Hospital from June 2014 to March 2025 who were diagnosed with peripancreatic arterial aneurysms (PAAs) and planned for surgical intervention. The peripancreatic vascular network includes the pancreaticoduodenal arcades and dorsal pancreatic artery (DPA). 21 Patients were identified through our institutional database using ICD codes for visceral aneurysms and procedural records. Inclusion criteria comprised radiologically confirmed PAAs via computed tomography angiography (CTA) and planned endovascular or open repair. Exclusion criteria were: conservative management of asymptomatic small aneurysms, incomplete medical records, or loss to follow-up (defined as no follow-up imaging after initial diagnosis). We confirmed that all patients received at least one pre-operative standardized high-resolute CTA imaging (slice thickness ≤0.5 mm) at our hospital. The study was approved by the institutional review board at Peking Union Medical College Hospital (protocol number: JS2629, date of approval: 2022-11-11), and informed consent was obtained from all participants. All procedures were in accordance with the 1964 Helsinki declaration and its later amendments. All patient details have been de-identified. Written informed consent was obtained from all individual participants included in the study. The reporting of this study conforms to STROBE guidelines. 22
Data collection
Demographic data (age, sex), comorbidities (hypertension, diabetes, smoking status), and clinical presentation were extracted from electronic medical records. Aneurysm characteristics (size, location, etiology, presence of collateral circulation) were assessed using preoperative imaging. Collateral branches were categorized (invisible, visible, and prominent) as previously reported. 23 Procedural details, including access route (femoral, brachial), embolization or open technique, and adjunctive interventions, were recorded from operative reports. CTA or ultrasound imaging follow up was conducted at 1 month, 6 months, and yearly after. Each patient would receive at least one post-operative CTA examination. Outcomes were evaluated at 30 days and during midterm follow-up. primary outcomes included 30-day morbidity or mortality, re-intervention, and aneurysm relapse during surveillance. Secondary outcome was long-term survival.
Operation technique
Endovascular repair was chosen as first-line treatment for PAAs, and open surgery was selected for patients with complicated anatomy or failed endovascular procedure. All endovascular procedures were performed in a hybrid operating room by experienced vascular surgeons. Under local anesthesia, femoral or brachial access was obtained based on aneurysm anatomy. Aortic and selective visceral angiography was performed to delineate aneurysm morphology and collateral pathways. For embolization, microcatheters were advanced into the aneurysm sac or parent vessels under fluoroscopic guidance. Coil embolization with detachable or non-detachable coils was the primary modality. Notably, since most aneurysms were located near a vessel bifurcation and lack sufficient either entering or run-offing parent vessels, the “sandwich” technique (occlusion of both run-in and run-off vessels) was intentionally avoided to preserve collateral flow. Technical success was defined as complete aneurysm exclusion on final angiography with little (expected to self-thrombosis) or no residual flow and patent collateral arteries.
For patients undergoing open repair, aneurysmectomy or aneurysmorrhaphy was chosen based on patients’ vessel anatomy, and endoscopic approach or laparotomy was selected. Intraoperative findings and surgical techniques were documented. Technical success was defined as complete aneurysm removal and preservation of visceral organ blood flow.
Statistical analysis
Continuous variables were reported as mean ± standard deviation or median (interquartile range [IQR]) and categorical variables were reported as frequencies. Comparisons between groups used Fisher's exact test for categorical data and unpaired Student's t-test or Wilcoxon test for continuous variables. A p value <0.05 was considered significant. Analyses were performed using SPSS v26 (IBM Corp.).
Results
Patient demographics and clinical characteristics
This study included 26 patients with PAAs (Table 1). The cohort had a mean age of 56.2 ± 12.9 years and 42.3% was male. Comorbidities included hypertension (42.3%), smoking (23.1%), and coronary artery disease (15.4%). Notably, only 30.8% of patients presented with symptoms (e.g. abdominal pain), while the majority were diagnosed incidentally during imaging for other conditions. Two (7.7%) patients were presented with a ruptured aneurysm and underwent emergent operation.
Patient clinical demographics.

BMI: body mass index; IQR: interquartile range; ASA: American Society of Anesthesiologists.
Aneurysm morphology and anatomical features
As shown in Table 2, there were 3 patients with multiple aneurysms. Aneurysm characteristics revealed a mean diameter of 21.7 ± 8.2 mm, with the majority located at the gastroduodenal artery–superior pancreaticoduodenal artery (GDA-SPDA, 57.7%) and the superior mesenteric artery–inferior pancreaticoduodenal artery (SMA-IPDA, 53.8%). Totally 23 (88.5%) patients had an aneurysm diameter of more than 15 mm. Etiologically, atherosclerosis (34.6%) and median arcuate ligament compression (30.8%) could be the leading causes. Isolated CA stenosis or occlusion was present in 16 patients (61.5%), including 7 with CA occlusion and 7 with >90% stenosis. Isolated SMA stenosis or occlusion was found in 2 patients (7.7%), comprising one with occlusion and one with >90% stenosis. Combined CA and SMA disease was present in 1 patient (3.8%), who had a > 90% CA stenosis and an SMA occlusion. Collateral circulation was prominent in 42.3% (11), visible in 34.6% (9), and absent in 23.1% (6) of cases.
Aneurysm characteristics.
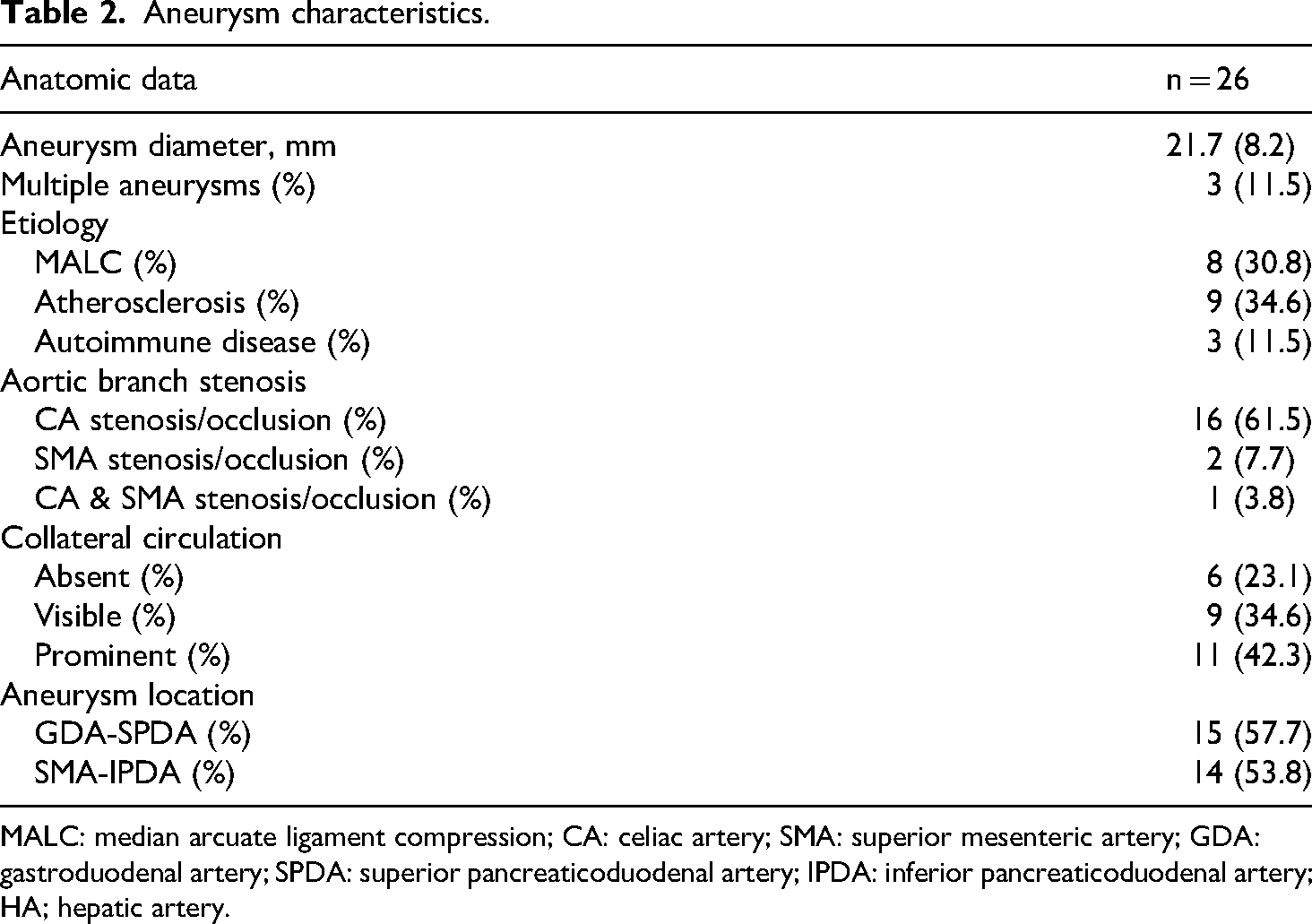
MALC: median arcuate ligament compression; CA: celiac artery; SMA: superior mesenteric artery; GDA: gastroduodenal artery; SPDA: superior pancreaticoduodenal artery; IPDA: inferior pancreaticoduodenal artery; HA; hepatic artery.
Procedural characteristics and technical outcomes
As illustrated in Table 3, endovascular repair achieved primary technical success in 88.5% (23) of cases and increased to 96.2% (25) with secondary interventions (i.e. open repair). One patient had an anatomical variation in which the aneurysm was located at the ostium of the right gastroepiploic artery, which provided compensatory blood supply to the spleen due to an occluded splenic artery. Given the high risk of splenic ischemia with embolization, open surgery was selected. One patient had a GDA-SPDA aneurysm with severe CA stenosis exceeding 95%. Endovascular access to the aneurysm failed via both the CA and SMA routes. The patient was converted to open surgery, during which adjunctive branch intervention for the CA stenosis was performed. The patient underwent laparoscopic aneurysmectomy of aneurysm and end-to-end artery anastomosis was performed. Another patient had a SMA-IPDA aneurysm with a concomitant 3 cm occlusion of the SMA. Endovascular access to the aneurysm was unsuccessful. As the patient declined open surgical repair, they were placed under annual surveillance to monitor for aneurysm growth. For endovascular details (Table 4), femoral access was utilized in 81.8% of endovascular procedures, while brachial access (18.2%) was reserved for anatomically challenging cases where femoral access had failed or was considered difficult for the visceral branch access. Notably, we observed significant differences in visceral branch access based on aneurysm location: celiac artery access predominated for GDA-SPDA aneurysms (66.7%), while SMA access was exclusively used for SMA-IPDA cases (p < 0.001). Figure 1 demonstrated one case with two aneurysms that were embolized through the CA and SMA access. Sac-only embolization was performed in 63.6% of cases, and selective occlusion of either the run-in or run-off was performed in 9.1% and 27.3% of cases, respectively. The mean procedure time was 2 h. Embolization was primarily performed using detachable coils (Interlock, Boston Scientific), while non-detachable coils (MWCE, Cook) were selectively used to pack larger aneurysms. The median number of coils used per procedure was five.

Pre- and peri-operative imaging of one patient with two PAAs. (a) Present of celiac axis stenosis (red arrow). (b) The patients had aneurysms located at the superior anterior PDA and inferior posterior PDA. (c)–(e) Three collateral pathways including the anterior PDA-GDA, posterior PDA-GDA, and the arc of Buhler pathway. (f) Selection and embolization of the superior aneurysm through CA. (g) Selection and embolization of the inferior aneurysm through SMA. (h) Final angiogram showed absence of flow in the aneurysms.
Peri-operative results and parameters.

Endovascular details.

CA: celiac artery; SMA: superior mesenteric artery.
Midterm follow-up and durability assessment
As listed in Table 5, at a median follow-up of 48 months (IQR 74), outcomes remained favorable, with only one case each of aneurysm relapse (remained stable after 1 year follow-up) and in-stent restenosis (in patients receiving CA stenting). No coil migrations, vessel occlusion, or major ischemic events occurred both based on clinical observation and imaging results. No patients had unresolved or new symptoms.
Midterm follow-up results.

IQR: interquartile range.
Discussion
The present study evaluated the safety and efficacy of endovascular management for peripancreatic arterial aneurysms (PAAs). Our findings demonstrate that endovascular repair achieves high technical success and favorable midterm outcomes, with low aneurysm recurrence and minimal ischemic complications. These results support endovascular therapy as a first-line approach for PAAs, particularly in anatomically suitable cases. Regarding threshold for intervention, although the current guideline recommends treating PAAs with a diameter greater than 15 mm—a criterion met by 23 of our 26 patients—it also notes that there is no clear association between PDAA diameter and rupture. 7 This underscores the need for more evidence to validate this specific treatment threshold.
The high technical success rate aligns with recent literature advocating endovascular therapy as first-line treatment for PAAs.16,17,24,25 Notably, our preference for sac-only embolization in most cases (63.6%) did not compromise durability compared to prior reports using dual occlusion. 17 This suggested that dense coil packing within the sac alone may suffice to induce thrombosis, especially in saccular aneurysms or those with limited inflow. 26 Unlike the sandwich method, which risks branch vessel ischemia, 27 our selective embolization strategy preserved critical flow while achieving aneurysm exclusion. This is particularly relevant for PAAs near bifurcations of the pancreaticoduodenal arcades, where there was little space for embolization at both ends of the aneurysm and excessive occlusion might compromise visceral perfusion. At a median 48-month follow-up, our outcomes were better or comparable with prior studies.16,24,25 The absence of coil migrations in our cases further supported the stability of this strategy.
An important technical insight was the differential access route based on aneurysm location. GDA-SPDA aneurysms frequently required CA access (66.7%), while SMA-IPDA aneurysms universally necessitated SMA catheterization. This aligned with Jazzar et al., 16 who emphasized SMA catheterization for PDA aneurysms. Hofmann et al. proposed a classification system of visceral artery aneurysm based on the different combinations of stenoses and aneurysm positions. 10 Our results suggested that this classification could also optimize vascular access planning. The case in Figure 1 showed how two aneurysms in distinct locations required separate CA and SMA access to achieve complete embolization while preserving collateral flow. Additionally, our low complication rate contrasts with older surgical series,18,28 which reinforced the safety of endovascular repair when performed with careful attention to collateral pathways.
Previous study indicated that aneurysm presence was associated with pancreaticoduodenal arcade development. 29 Our experience suggested that in the absence of mesenteric ischemia symptoms, celiac stenosis could often be left untreated when treating PAAs, provided there was adequate collateral flow demonstrated on preoperative imaging. This approach simplified the procedure, reduced operative time, and avoided potential complications associated with celiac artery stenting or bypass, such as in our one case of CA stenting and restenosis. Results from a multicenter study also questioned the efficacy of CA stenting. 13 The absence of mesenteric ischemic complications during follow-up further supported the safety of this strategy.
Our series included three patients who ultimately underwent open surgical repair - two after failed endovascular attempts and one who was primarily selected for open surgery due to aneurysm anatomy. One of the converted cases had a visceral artery anatomical variation that posed a high risk of splenic ischemia if embolized, while the other had an aneurysm that was inaccessible via either the CA or SMA. The primarily open case had a complex saccular aneurysm with small critical branches directly supplying the duodenum. 30 These cases underscore the critical importance of individualized treatment planning based on careful assessment of aneurysm morphology, vascular anatomy, and collateral circulation patterns.31,32 The decision-making process should incorporate multiple factors including aneurysm size, location, branch vessel involvement, and the patient's overall surgical risk. 33 Our experience reinforces that while endovascular techniques are preferable for most PAAs, a subset of patients will benefit from open repair, and vascular surgeons should maintain proficiency with both approaches.20,34
This study has some limitations. Due to the disease rarity, a small sample size was retrospectively included. Heterogeneity in embolization and open techniques and follow-up duration may affect generalizability. Nonetheless, our protocol in embolization strategies could minimize variability. Future studies should evaluate long-term durability and optimal follow-up protocols.
Conclusion
Endovascular management of peripancreatic arterial aneurysms could achieve good technical success and midterm durability without routine celiac trunk revascularization. Tailored embolization strategies based on aneurysm location and collateral circulation optimize outcomes while minimizing ischemic risks, though complex anatomies may still require individualized surgical intervention.
Footnotes
Acknowledgments
None.
Ethical considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the institutional review board at Peking Union Medical College Hospital (protocol number: JS2629, date of approval: 2022-11-11).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Consent for publication was obtained for every individual person's data included in the study.
Author contributions
S.L., XN.S., and Y.Z. contributed to the study design. S.L. contributed to the data analysis. S.L., XN.S., and W.X. contributed to the manuscript writing and revision. R.Z., XT.S., and F.L. contribute to electronic image analysis. S.L., XN.S., R.Z., XT.S., F.L., Z.L, and Y.Z. contributed to operational performance and clinical data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Beijing Natural Science Foundation (grant number L246053), the Natural Science Foundation of China (grant number 82070492, 82100519, and 82470504), the Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (Grant No.2024-JKCS-21), the Peking Union Medical College Hospital Talent Cultivation Program (UHB11865), the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (Grant No.CIFMS2021-I2M-1-016), the Fundamental Research Funds for the Central Universities Peking Union Medical College (Grant No. 3332025183), and the National High Level Hospital Clinical Research Funding (Grant No. 2022-PUMCH-B-100, 2022-PUMCH-C-062, and 2025-PUMCH-A-180).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.