
Abstract
Objective
To evaluate the mid-term outcomes of different treatment strategies for the internal iliac artery (IIA) during EVAR.
Methods
This was a retrospective study. All patients undergoing EVAR, who required treatment of at least one side of IIA from January 2013 to July 2022 in a single center, were included. According to the different treatment strategies for IIA, the patients were divided into UP (unilateral preservation), BP (bilateral preservation) and BE (bilateral embolization) groups. The primary outcomes included buttock claudication, bowel ischemia and iliac-related reintervention. Then patients who underwent IIA reconstruction were divided into IPG (iliac parallel stent graft) and IBG (iliac branch stent graft) groups according to the reconstruction technique. The primary outcomes included endoleak, iliac branch occlusion and iliac-related reintervention.
Results
A total of 237 patients were included, including 167 in the UP group, 9 in the BP group and 61 in the BE group. The mean follow-up time was 39.0 ± 27.7, 50.0 ± 22.1 and 25.8 ± 18.9 months in UP, BP and BE groups, respectively. Thirty cases (12.7%) of buttock claudication occurred, and it was significantly higher in the BE group than the UP group (26.2% vs. 7.8%, p < 0.001). There were no significant differences in the other follow-up outcomes among three groups. The K–M analysis indicated that the patients in the BE group had a lower survival rate than those in the other two groups (p = 0.024). 24 patients underwent IIA reconstruction, including 8 in the IPG group and 16 in the IBG group. The endoleak in the IBG group was significantly lower than that in the IPG group (0% vs. 25.0%, p = 0.041). The iliac-related reintervention, iliac occlusion and mortality were similar between the two groups.
Conclusion
Overall it is beneficial for patients to preserve at least one side of IIA during EVAR as much as possible. Compared with IPG, IBG might be more applicable for IIA reconstruction.
Keywords
Introduction
With the promotion of minimally invasive techniques, endovascular aneurysm repair (EVAR) has become widely used to treat abdominal aortic aneurysms (AAAs).1–3 Approximately 15–40% of patients with AAAs also have unilateral or bilateral common iliac artery aneurysms (CIAAs) and internal iliac artery aneurysms (IIAAs). 4 Anatomically, EVAR needs a suitable landing zone, that is, a nonaneurysmal, flat area of the arterial wall, to achieve a good sealing effect. 5 In the absence of a suitable distal landing zone in the common iliac artery (CIA), it is often necessary to extend the iliac branch stent to the external iliac artery (EIA), which needs to cover the internal iliac artery (IIA).6,7 When the stent extends beyond the IIA, without action, it could lead to endoleak within the stent, resulting in adverse outcomes. Therefore, it is particularly important to deal with the IIA. 8 Typically, proximal embolization of the IIA is selected to block blood flow prior to stent placement, and it can also be preserved with other endovascular techniques.
IIA embolization is one of the most commonly used methods for EVAR, but ischemic complications can limit the functional recovery and quality of life of patients.9,10 Approximately 30% of patients are complicated with buttock claudication, 11 10% of male patients are complicated with erectile dysfunction, and fewer than 1% of patients are complicated with other severe ischemic complications (gluteal/intestinal/spinal cord ischemia).12,13 Therefore, to preserve the blood supply to the IIA as much as possible, a more advanced method of IIA reconstruction has become popular in recent years, and an increasing number of clinicians are recommending and applying IIA reconstruction. 14 The main methods of IIA reconstruction include internal-external iliac artery bypass, the iliac parallel stent graft technique and the iliac branch stent graft technique. 15 Parallel stent graft technique include sandwich technique, crossover chimney technique, etc. The former is that the IIA and EIA parallel kissing stents are inserted into the iliac branch of the main stent, the latter relies on the chimney stent to connect the target IIA with the contralateral EIA.
Although IIA reconstruction is currently considered to be the most ideal treatment, 16 not all patients can undergo IIA reconstruction. Some case reports have shown that some patients have difficulty reconstructing IIA due to the limitations of their own anatomical conditions and the nature of their aneurysms. Therefore, for various reasons, IIA embolization should still be used when needed. The selection of the right strategy for the treatment of the IIA and the advantages of the different reconstruction techniques are the focus of this study. We analyzed and compared the medium-term outcomes of different treatments of the IIA in EVAR to provide a reference for future clinical treatment.
Methods
Study design
This was a retrospective, single center study of patients who underwent EVAR and operation on the IIA. The study was approved by the ethics committee of Tianjin Medical University General Hospital (IRB2022-YX-1110-01) on June 30, 2022, and was conducted in accordance with the Helsinki Declaration for research involving human subjects of 1975 as revised in 2013. Informed consent was waived because of the retrospective nature of our study. The study anonymized the personal or identifying data of the patients involved in the study. No personal or identifying information was collected. The reporting of this study conforms to STROBE guidelines. 17
A total of consecutive 237 patients who underwent EVAR and operation on the IIA in a single center from January 2013 to July 2022 were retrospectively analyzed. According to the treatment strategy for the preservation of IIA blood supply, they were divided into three groups: unilateral preservation group (UP group), bilateral preservation group (BP group) and bilateral embolization group (BE group). The UP group included patients with unilateral IIA embolization and a normal contralateral IIA or with unilateral IIA reconstruction and contralateral IIA embolization. The BP group included patients with bilateral reconstruction of the IIA or with a reconstructed IIA on one side and a normal IIA on the other. The BE group included patients with bilateral embolism of IIA. Patients undergoing IIA reconstruction were divided into an IPG group and an IBG group according to the iliac parallel stent graft (IPG) and iliac branch stent graft (IBG) reconstruction techniques. Among them, the IPG technique is the main sandwich technology, and the IBG technique includes an iliac branch device (IBD) and an iliac branch endoprosthesis (IBE).
Inclusion criteria: patients who underwent EVAR and surgery on the IIA in the department of vascular surgery of our hospital, with complete clinical data and at least one follow-up. A total of 259 patients completed the operation, but 22 patients were excluded from the study because of incomplete data or lack of follow-up. Exclusion criteria: (1) EVAR with a distal landing zone in the CIA; (2) patients with isolated CIAAs or IIAAs who did not need EVAR because the proximal and distal landing zones were sufficient; (3) patients who underwent open surgery under general anesthesia; (4) patients with severe congenital anatomical malformations of the iliac arteries; (5) patients with long-term and severe occlusion of an IIA.
Procedure
Procedural details are shown in Figure 1. In the following description of the specific operation steps, we omit the description of EVAR. All procedures were performed using local anesthesia. Unilateral embolization of the IIA (Figure 1A and B) involved placing one or more coils in the target IIA so that no blood could flow through it. Bilateral embolization (Figure 1C and D) was performed in stages in all elective operations; that is, one IIA was embolized in the same way as for unilateral embolization, and the other IIA was embolized one week later. The types of coils used included Interlock (Boston Scientific), Nester (Cook) and Phoenix (Zylox). The diameter and length of coils are selected by the clinician, based on the diameter of the patient's IIA. All coils were placed in the proximal IIA trunk.

Intraoperative angiography for internal iliac artery surgery. Unilateral embolization of the IIA (A); Post-embolization image of the left IIA, with the red arrow showing the coil placed in the left IIA (B); Bilateral embolization of the IIAs (C); Postembolization image of the bilateral IIAs, with the red arrows showing the coils placed in the bilateral IIAs (D); Reconstruction of the IIA by IPG technique (E); Postreconstruction image of the right IIA by IPG technique, with the red arrow showing the iliac artery stent placed in the right iliac artery (F); Reconstruction of the IIA by IBG technique (G); Postreconstruction image of bilateral IIAs by IBG technique, with the red arrows showing the iliac artery stents placed in the bilateral iliac arteries (H).
The IIA was reconstructed mainly by the IPG technique or the IBG technique. The IPG technique (Figure 1E and F) concurrently released two stents in the EIA and IIA by the kiss technique in the main stent located above the opening of the IIA. The IBG technique (Figure 1G and H) aligned the marker of the main stent at the IIA entrance, released part of the main stent below the marker, and then completely released the main stent after placing an IIA stent in the marker. Finally, the balloon dilated the distal and proximal ends of the stent and the stent junction, respectively.
Follow-up
All patients underwent follow-up CT angiography at the outpatient clinic at 1, 6 and 12 months after the procedure and then once a year thereafter, with regular telephone follow-up. The primary outcomes at follow-up for the UP group, BP group and BE group were the incidences of buttock claudication, bowel ischemia and iliac-related reintervention. The secondary outcomes for the three groups were the endoleak rate, iliac branch occlusion rate and mortality. The primary outcomes at follow-up for the patients who underwent IPG and IBG included the endoleak rate, the iliac branch occlusion rate and the iliac-related reintervention rate. The secondary outcome for the two groups was mortality.
Statistical analysis
SPSS statistics software was used for the statistical analysis. Continuous variables are presented as mean ± standard deviation, and categorical values are presented as percentages. Normality was determined using the independent samples t-test for comparison between two groups, and analysis of variance (ANOVA) was used for comparison between more than two groups. If continuous variables were non-normally distributed, the Wilcoxon Mann‒Whitney U rank test was used for comparisons between two groups, and the Kruskal‒Wallis H rank test was used for comparisons between more than two groups. Differences in categorical variables were assessed by the chi-square test or Wilcoxon–Mann–Whitney U test. In the comparison of baseline data, all patients enrolled in the study were compared. In the analysis of follow-up data, patients who were lost to follow-up were excluded. With death and intervention as the endpoints, Kaplan–Meier (K–M) analysis was done to compare the cumulative survival rate and freedom from reintervention rate and evaluate the prognostic value. Differences were defined as significant at p < 0.05.
Results
Outcomes of different treatment strategies
A total of 237 patients were included in the current study, including 167 patients in the UP group, 9 patients in the BP group and 61 patients in the BE group. Among them, 13 patients were isolated iliac aneurysms and 224 patients were AAAs, of which 148 patients had unilateral or bilateral iliac aneurysms. In the UP group, 152 patients underwent unilateral embolization of an IIA, while the other 15 underwent unilateral reconstruction and embolization of the contralateral artery. In the BP group, 8 patients underwent unilateral reconstruction, and only one patient underwent bilateral reconstruction. In the BE group, all 61 patients underwent bilateral embolization. In summary, 314 IIAs were treated in the study, of which 25 were reconstructed and 289 were embolized. The baseline characteristics of the three groups are shown in Table 1. There were no statistically significant differences among the three groups in terms of baseline characteristics such as sex, smoking history, comorbidities and maximum diameter of aneurysm (all p > 0.05). The BE group was significantly older than the UP group (74.0 ± 6.9 years vs. 69.6 ± 7.9 years, p = 0.001).
Baseline characteristics of the 237 patients in three groups.

Continuous variables are presented as mean ± standard deviation, categorical values as n (%).
UP: unilateral preservation; BP: bilateral preservation; BE: bilateral embolization; AAA: abdominal aortic aneurysm; CIAA: common iliac artery aneurysm; IIAA: internal iliac artery aneurysm.
Comparison between UP group and BP group, p > 0.999. Comparison between UP group and BE group, p = 0.001. Comparison between BP group and BE group, p = 0.076.
All 237 patients successfully underwent IIA-related operations. Of these, 11 were admitted to emergency care for symptomatic or ruptured AAA, and the rest were elective. The procedural success rate was 100%. Of all patients, 91.6% of the patients underwent standard EVAR, and the rest underwent chimney, fenestrated or branched EVAR. Four patients died during the perioperative period: two died of excessive ischemia caused by ruptured aneurysms (one each in the UP and BE groups), and two were due to non-operation-related deaths (both in the BE group). There was no significant difference in the perioperative complication rate or perioperative mortality among the three groups (all p > 0.05) (Table 2). Since our surgical records in the past focused on the operation process and stent information, we only began to record the detailed use of coils (including manufacturer and quantity) in 2019. As a result, we only collected data on coil implantation in 142 patients. Of these patients, 69% used Interlock coils from Boston Scientific, 34.5% used Nester coils from Cook Medical and 12% used Phoenix coils from Zylox Medical.
Perioperative outcomes of the 237 patients in three groups.
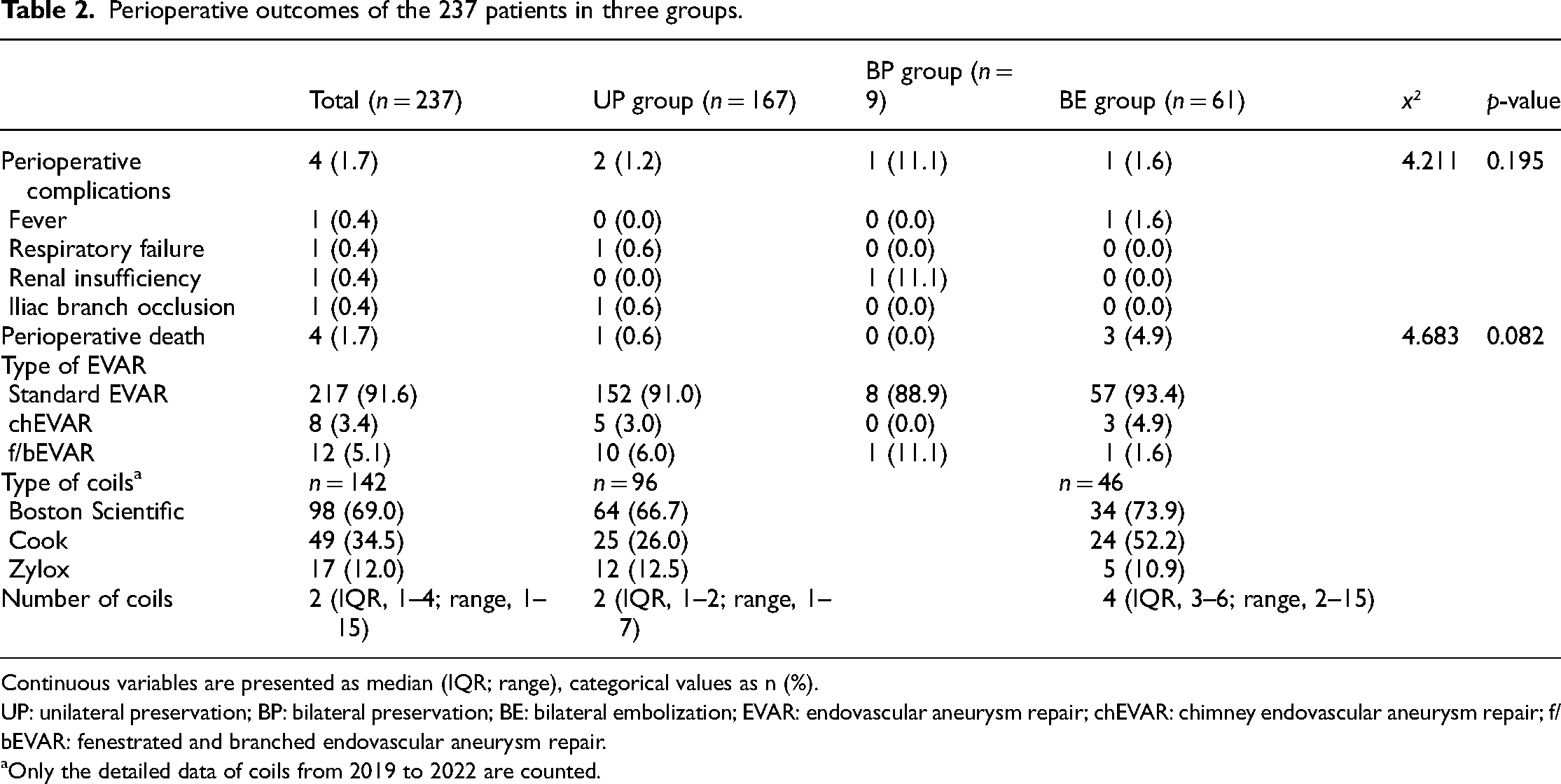
Continuous variables are presented as median (IQR; range), categorical values as n (%).
UP: unilateral preservation; BP: bilateral preservation; BE: bilateral embolization; EVAR: endovascular aneurysm repair; chEVAR: chimney endovascular aneurysm repair; f/bEVAR: fenestrated and branched endovascular aneurysm repair.
Only the detailed data of coils from 2019 to 2022 are counted.
In the end, the follow-up rate was 100%. The mean follow-up time was 39.0 ± 27.7 months in the UP group, 50.0 ± 22.1 months in the BP group, and 26.0 ± 21.0 months in the BE group. The follow-up outcomes of the three groups are shown in Table 3. There was a statistically significant difference in the incidence of buttock claudication among the three groups (p = 0.001). Further pairwise comparison showed that the incidence of buttock claudication in the BE group was significantly higher than that in the UP group (26.2% vs. 7.8%, p < 0.001). A total of 8 patients (3.7%) had complications of bowel ischemia, but all were mild symptoms that could be effectively alleviated by drugs. No major ischemic events were noted. The differences in the bowel ischemia rate, iliac-related reintervention rate, endoleak rate, iliac branch occlusion rate, aneurysm-related mortality and all-cause mortality among the three groups were not significant (all p > 0.05). The patients in the BE group showed significantly lower survival rate than those in the other two groups (p = 0.024, Figure 2A). And according to the K–M curves, the patients among the three groups showed no significant differences in the freedom from reintervention rate (p > 0.05, Figure 2B).
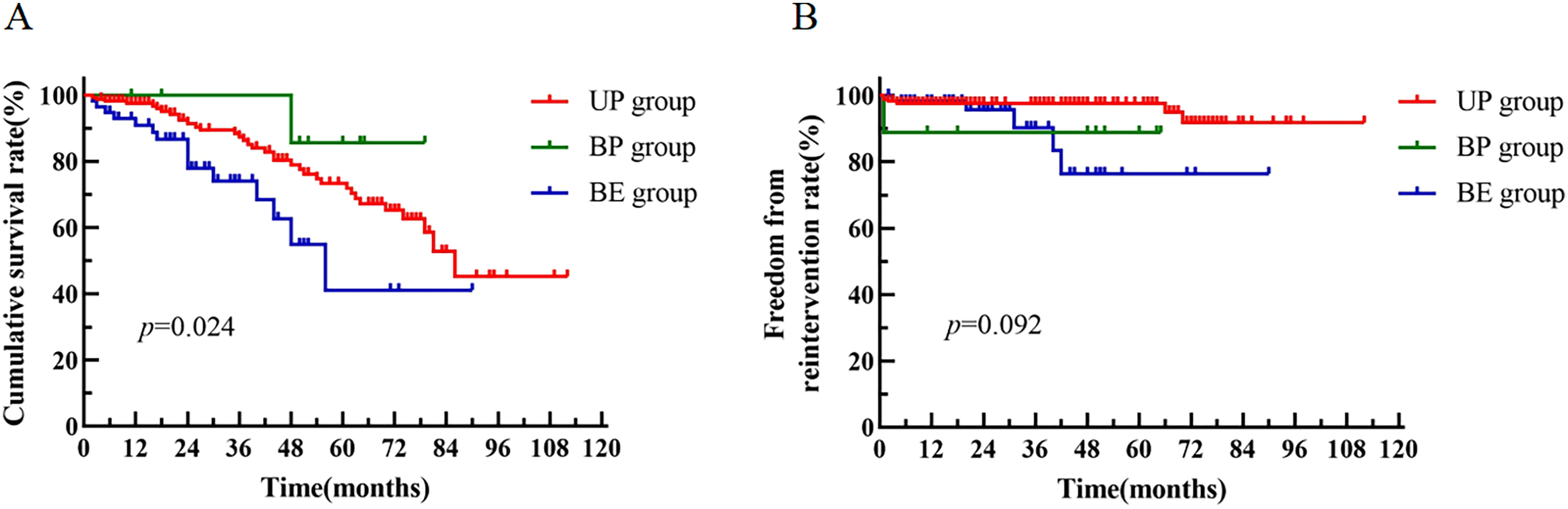
K–M curve with death and intervention as the endpoint of the UP group, BP group and BE group. K–M survival curves of the three groups (A); K–M curves free from intervention of the three groups (B).
Follow-up outcomes of the 237 patients in three groups.

Continuous variables are presented as mean ± standard deviation, categorical values as n (%).
UP: unilateral preservation; BP: bilateral preservation; BE: bilateral embolization.
Comparison between the UP and BP group, p = 0.538. Comparison between the UP and BE group, p < 0.001. Comparison between the BP and BE group, p = 0.502.
Outcomes of different reconstruction techniques
A total of 24 patients underwent IIA reconstruction, including 8 in the IPG group and 16 in the IBG group. One of them underwent bilateral reconstruction; consequently, a total of 25 IIAs were reconstructed. The comparison of baseline characteristics is shown in Table 4. There were no significant differences between the two groups in terms of baseline characteristics such as age, sex, smoking history and comorbidities (all p > 0.05).
Baseline characteristics of the 24 patients in two groups.

Continuous variables are presented as mean ± standard deviation, categorical values as n (%).
IPG: iliac parallel stent graft; IBG: iliac branch stent graft; AAA: abdominal aortic aneurysm; CIAA: common iliac artery aneurysm; IIAA: internal iliac artery aneurysm.
All 24 IIA reconstructions were successful, with a procedural success rate of 100%. All patients in the IPG group used sandwich technique to reconstruct IIA, 14 patients in the IBG group used IBG technique and 2 patients used the IBE technique. One patient in the IBG group developed perioperative renal insufficiency, which improved after treatment.
The mean follow-up time was 55.9 ± 30.9 months in the IPG group and 37.6 ± 26.5 months in the IBG group. The follow-up outcomes in the two groups are shown in Table 5. Endoleak occurred in two patients in the IPG group. The endoleak rate in the IPG group was significantly higher than that in the IBG group (25.0% vs. 0%, p = 0.041). There were 4 patients with iliac-related secondary procedures, including three patients in the IPG group and only one in the IBG group. In the IPG group, two patients underwent catheter-directed thrombolysis and incisional thrombectomy due to iliac branch occlusion, and one patient underwent IIA embolization due to endoleak at the reconstruction site. In the IBG group, one patient underwent incisional embolization due to iliac branch occlusion. There were three patients who developed iliac branch occlusion (two in the IPG group and one in the IBG group). They had a 12.5% (3/24) rate of iliac branch occlusion, and all underwent secondary procedures. The differences in the incidence of iliac branch occlusion, iliac-related reintervention, aneurysm-related death and all-cause death between the two groups were not significant (all p > 0.05). In addition, the K–M survival curve showed no significant difference between the two groups (p > 0.05, Figure 3A). And the patients in the two groups showed no significant differences in the freedom from reintervention rate (p = 0.057, Figure 3B).
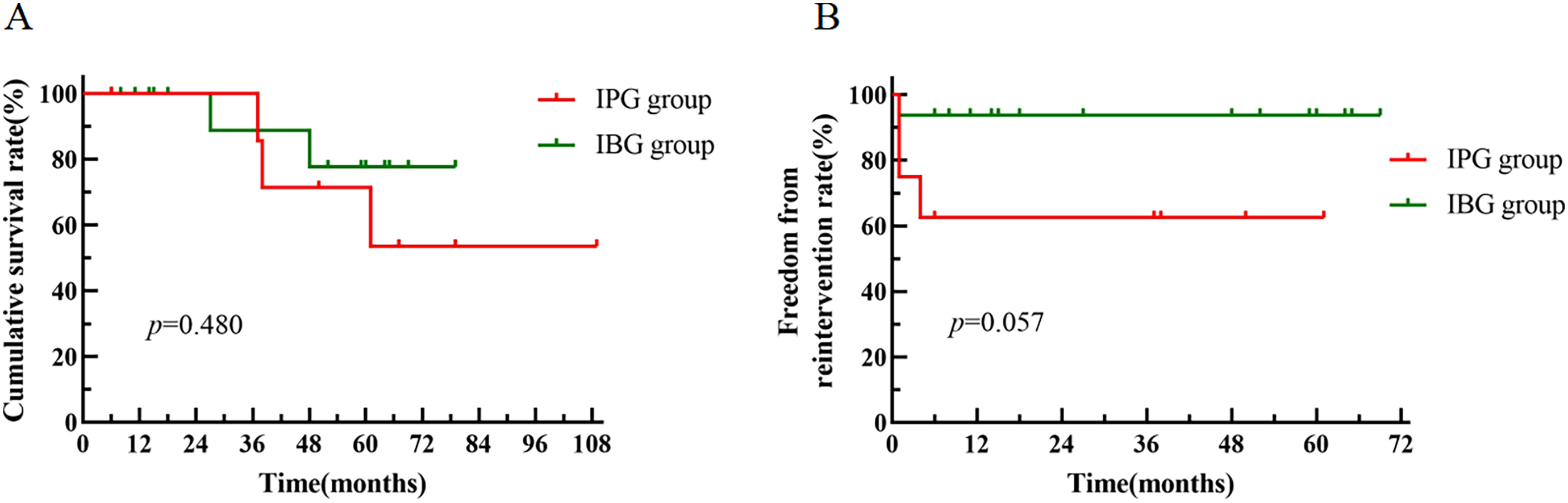
K–M curve with death and intervention as the endpoint of the IPG group and IBG group. K–M survival curves of the two groups (A); K–M curves free from intervention of the two groups (B).
Perioperative and follow-up outcomes of the 24 patients in two groups.

Continuous variables are presented as mean ± standard deviation, categorical values as n (%).
IPG: iliac parallel stent graft; IBG: iliac branch stent graft; IBD: iliac branch device; IBE: iliac branch endoprosthesis; IIA: internal iliac artery.
Discussion
In many patients with AAAs combined with iliac aneurysms, EVAR requires distal extension of the stent to the EIA and coil embolization of the IIA. 7 However, ischemic complications due to embolization can seriously worsen the functional recovery and quality of life of the patients. 10 Therefore, IIA reconstruction has become a more popular strategy in recent years. In the current study, we compared different treatment strategies for IIA in EVAR and made an important finding in the comparison of the IIA-associated tissue ischemia rate. The incidence of buttock claudication reached 26.2% when there was no blood supply to both IIAs, while in patients with a unilateral blood supply, the incidence of buttock claudication was only 7.8%. It is clear that the application of bilateral embolization without preserving the IIA blood supply can, to some extent, lead to a higher probability of complications. Reportedly, buttock claudication stands as the most common complication for IIA embolization, affecting approximately 28% of patients. 18 In addition, many studies have shown that the complication of male sexual dysfunction due to IIA embolization can be as high as 10%. 12 However, meaningful data were not available in this study due to the limitations in the follow-up.
Yamashita et al. 19 reported that unilateral IIA embolization was not related to gluteal muscle atrophy after EVAR. In another clinical study, 91 patients who underwent open or endovascular repair were reported. It was also suggested that patients without IIA preserved had a higher incidence of bowel ischemia, buttock claudication and perioperative mortality. 20 Similarly, in our study, we found an enhanced risk for buttock claudication in the BE group, but no significant difference was seen in follow-up complications between the UP and BP groups. Therefore, it is beneficial to selectively preserve at least one side of the IIA in EVAR. Whether IIA reconstruction should completely replace unilateral embolization needs to be further explored, but the preservation of at least one IIA is imperative for full functional recovery when both IIAs need to be addressed.
Despite research suggesting a heightened risk of complications from IIA embolization, many patients opt for this procedure. The main reason is the patient's own financial situation. EVAR is costly, particularly for those with complex abdominal aortic aneurysms with iliac aneurysms who might require multiple stents. Given these factors, concerns about preserving the IIA seem relatively low compared to life-threatening aneurysms. Furthermore, considering some elderly patients already experience limited mobility or reduced sex function from other conditions, preserving the IIA loses its significance for such individuals. In addition, due to anatomical structural limitations, including sharp bifurcation, iliac artery distortion and inadequate CIA length, it may be difficult to place IIA reconstruction stents.
In terms of surgical procedures, we also want to reduce the risk of embolization as much as possible. We usually choose to place the coils at the proximal portion of the IIA trunk to facilitate the establishment of collateral circulation in the distal portion and staged bilateral embolization to provide time for collateral vessels to develop, although its effect remains open to question.12,21,22 Indeed, during IIA embolization, preserving distal blood flow by first targeting the proximal end can enhance collateral circulation received from the contralateral IIA, mesenteric and femoral arteries. Although the vast majority of ischemic adverse events caused by IIA embolism are not fatal complications, their impact on quality of life cannot be ignored. Adequate assessment should be made to determine whether there is an opportunity to preserve the blood supply of the IIA, especially if one side is to be interrupted, and more attention should be paid to the preservation of the other side.
The methods used to reconstruct the IIA in our hospital are mainly the sandwich technique, IBD technique and IBE technique. The sandwich technique is an IPG technique, so it was included in the IPG group in our study. The IBE technique is a recent method used in international multicenter studies that has achieved a high technical success rate and a low mortality rate. 23 The domestic IBD and imported IBE both belong to the IBG category, so they were included in the IBG group in our study. To date, a direct comparison between the IBG and IPG techniques for reconstructing the IIA has rarely been reported. However, the IBG technique has been shown in most reports, the incidence of postoperative complications is reduced, and the safety and technical success rate are also improved.14,24–27 Therefore, it has become one of the more widely advocated techniques in recent years. In this study, the IBG and IPG techniques were investigated. We directly compared the postoperative follow-up after the IBG technique vs. the IPG technique. Only the endoleak rate in the IBG group was lower than that in the IPG group. The other result showed no significant difference between the two groups due to the limited sample size. Overall, the IBG technique is superior to the IPG technique. Cao et al. 16 also preferred the IBD technique for bilateral reconstruction when anatomical conditions allow because the IBD technique has a high surgical success rate and can effectively reduce the occurrence of ischemic complications.
In addition, of the 24 patients with IIA reconstruction, 3 had iliac branch occlusion. The potential risk of iliac branch occlusion after reconstructive surgery should not be overlooked. Lobato et al. 28 reported on 40 patients who underwent IIA reconstruction using the sandwich technique, and three patients developed iliac branch occlusion early in the study. Stern et al. 29 reported that three patients underwent a secondary procedure due to iliac branch occlusion among 59 patients treated for IBD (one EIA occlusion and two IIA occlusions). Whether iliac branch occlusion after reconstruction is related to different reconstruction techniques has not been confirmed. Although the problem of possible iliac branch occlusion after reconstruction needs to be further resolved, patients still achieved more satisfactory outcomes in terms of functional recovery and quality of life. IIA reconstruction is worthy of further promotion. So far, no comparison between bilateral IIA reconstruction vs unilateral reconstruction and contralateral embolization has been reported. In this study, there is no significant difference between UP and BP groups, and IIA reconstruction itself has the possibility of potential endoleak and iliac branch occlusion, so bilateral reconstruction may not be dominant. However, according to the current research results, there is a significant benefit of preserving at least one side of the IIA.
The first limitation of this study is its retrospective and nonrandomized design. All surgical treatments were tailored to the unique circumstances of each patient. We only summarized the actual situation of these patients retrospectively. Since this is a retrospective cohort study, sample selection is based on inclusion and exclusion criteria, and sample size and power analyses are not performed, which may lead to biased results. Another limitation of the current study is the wide variation in follow-up time. There were inevitable errors in postoperative follow-up, as some patients who had not yet developed distant complications may have been missed. In addition, in the comparison of the UP, BP and BE groups, baseline heterogeneity due to age differences may have affected the results. The relatively small sample size and the fact that the cases were from a single center also limited this study. Therefore, the findings of this study await further confirmation in a larger, longer, multicenter study.
Conclusions
Currently, preserving at least one IIA blood supply in EVAR helps to reduce the occurrence of ischemia complications. IIA reconstruction should replace bilateral embolization when systemic conditions and anatomic conditions are suitable. The IBG technique for reconstructing the IIA may lead to better outcomes than the IPG technique.
Footnotes
Acknowledgements
We thank editors for manuscript review, and the anonymous reviewers, who made significant and appreciated contributions to the final article.
Author contributions
This study was designed by JJ. The study selection was done by BJX, CYH, ZXX, ZB and DXC. Data collection was performed by BJX, CYH, and ZXX. Data analysis was performed by BJX, CYH, LH and FJB. The initial manuscript was written by JJ. DXC is the final arbitrator of this manuscript. The final version was read, corrected and approved by all the authors.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case series was obtained from the Ethics Committee of Tianjin Medical University General Hospital (IRB2022-YX-110-01) on June 30, 2022.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China projects (No. 82241207 and 82070489).
Informed consent
Informed consent for patient information to be published in this article was waived by Ethics Committee of Tianjin Medical University General Hospital because of the retrospective nature of our study.