
Abstract
Objective
The aim of study is to investigate the safety and efficacy of preserving bilateral internal iliac arteries (IIAs) in patients with aortoiliac aneurysms using iliac branch stent grafts (IBSG).
Methods
From June 2019 to February 2024, a total of 265 patients with aortoiliac aneurysm from four tertiary hospitals in China were included. They were divided into 110 patients with bilateral iliac artery aneurysms and 155 patients with unilateral aneurysm. Based on whether the IIA were occluded, the patients with bilateral aneurysms were further divided into Group BB (bilateral aneurysms with bilateral IBSG) and Group BU (bilateral aneurysms with unilateral IBSG and contralateral IIA embolization), and the patients with unilateral aneurysm into Group UB (unilateral aneurysm and preserve bilateral IIA) and Group UU (unilateral aneurysm and preserve unilateral IIA). Group BB and Group BU, as well as Group UB and Group UU, were compared after propensity score matching. The primary endpoint was major adverse events, and the secondary endpoint was pelvic ischemia.
Results
After matching, there were 76 patients in the Group BB (38 patients) and the Group BU (38 patients), with an average follow-up of 24.0 ± 7.0 months. Among these patients, 3 patients (7.9%) in the Group BB and 2 patients (5.3%) in the Group BU experienced IBSG occlusion. In the Group BB, 1 patient (2.6%) had type IB endoleak, 1 patient (2.6%) had type III endoleak due to IBSG migration, and 1 patient (2.6%) in the Group BU had type I endoleak. The rate of IBSG-related interventions was similar between the two groups (13.2% vs. 7.9%, p > 0.05). Compared with the Group BB, patients with buttock claudication (1 vs. 10, p < 0.05) and decreased erection function (2 vs. 12, p < 0.05) were more common in the Group BU, and the Group BU also reported more new cases of erectile dysfunction (1 vs. 6, p < 0.05). After matching, there were 55 patients in the Group UB and 55 patients in the Group UU, with an average follow-up of 23.0 ± 6.0 months. One patient (1.8%) in the Group UB and 1 patient (1.8%) in the Group UU experienced type I endoleak. Four patients (7.3%) in the Group UB and 1 patient (1.8%) in the Group UU underwent reintervention (p > 0.05). One patient (1.8%) in the Group UB and 13 patients (23.6%) in the Group UU complained of buttock claudication, and more patients in the Group UU had decreased erection function (2 vs. 14, p < 0.05). Among these, 9 patients (16.4%) had newly developed erectile dysfunction (p < 0.05). During the study period, no patients experienced aneurysm-related mortality.
Conclusion
The complete preservation of bilateral IIAs using IBSG has shown satisfactory midterm results, which are associated with lower rates of occlusion and reintervention. Additionally, the strategy may effectively preserve the ambulation and sexual function of patients.
Keywords
Introduction
Adequate landing zones at both the proximal and distal ends of the aorta are crucial for achieving successful endovascular aortic aneurysm repair (EVAR). 1 In a substantial proportion of cases, approximately 43% of patients with abdominal aortic aneurysms exhibit concurrent iliac artery aneurysms. Among these cases, the common iliac artery is the primary site of aneurysm formation, accounting for 70–90% of occurrences.2,3 Insufficient distal sealing zone in the presence of iliac artery dilation may potentially result in type IB endoleak.4,5 Thus, aortoiliac aneurysms (AIAs) pose significant challenges during EVAR procedures.
The conventional approach to treating AIAs involves extending the stent graft into the external iliac artery, along with occlusion of the internal iliac artery (IIA). The occurrence of spinal cord and colonic ischemia is relatively low, though their clinical implications are significant. Consequently, the occlusion of bilateral IIAs is typically avoided. 6 Both ESVS and SVS guidelines recommend preserving at least one IIA when possible, while ensuring that aneurysm exclusion is not compromised.7,8 However, studies have shown that preserving a single IIA may still lead to a 20–30% incidence of buttock claudication and a 10% incidence of erectile dysfunction in patients.9,10 Several techniques are utilized to preserve IIA during EVAR, including the Bell-bottom, Crossover Chimney, Sandwich technique, and Iliac Branch Stent Graft (IBSG).11–14 The pELVIC registry study has confirmed the correlation between IBSG implantation and low rates of occlusion and type I endoleak, further substantiating its safety and effectiveness in clinical interventions. Given the high technical success rates and the low morbidity and mortality associated with IBSG techniques for preserving the IIA, a critical question emerges: Can maintaining bilateral blood supply to the IIAs in patients with AIAs leads to long-term preservation of postoperative walking and sexual function, and consequently, provide sustained clinical benefits? This is a pressing issue that warrants further investigation in the future of AIA repair.
Comparative studies evaluating IIA perfusion preservation remain relatively scarce, with a notable paucity of high-quality randomized controlled trials. 15 This study aims to explore the safety and efficacy of preserving bilateral IIAs in patients with AIAs through the utilization of IBSGs. The study focuses on analyzing the midterm clinical outcomes and assessing the impact of comprehensive preservation of bilateral IIAs using IBSG on postoperative pelvic ischemia.
Patients and methods
Study design and population
This multicenter retrospective study consecutively enrolled 273 patients with AIAs who underwent endovascular treatment at four tertiary medical centers in China (The Affiliated Hospital of Qingdao University; Qingdao Hiser Hospital Affiliated of Qingdao University; Beijing Friendship Hospital; Linyi Peoples’ Hospital) from June 2019 to February 2024. Figure 1 summarizes the research process of this retrospective study. The inclusion criteria were: 1. patients with AIA who underwent EVAR with preservation of the IIA or occlusion of the IIA. The exclusion criteria were: 1 Patients transferred to open surgery. 2. Patients who preserved the IIA using other techniques. 3. Patients who covered the entrance of the IIA with the stent graft without occluding it. 4. The use of multiple stents to facilitate extension to a major branch of the IIA, such as the superior gluteal artery patients undergoing emergency surgery. This study included a total of 265 patients, with 63 enrolled between 2019 and 2021 and 202 enrolled between 2022 and 2024. This distribution was primarily attributed to the impact of the COVID-19 pandemic and the procedural learning curve. Among them, 110 patients had bilateral iliac artery aneurysms, and 155 had unilateral involvement. Patient data, including demographic characteristics, anatomical features, and clinical information, were retrospectively collected and analyzed. The patients were divided into four groups: Group BB, Group BU, Group UB, and Group UU.

Study flowchart.
Figure 2 summarizes the treatment strategies for the IIAs in all patients included in this study. In Group BB, bilateral iliac artery aneurysms were treated with bilateral implantation of IBSG, thereby preserving both IIAs. In Group BU, patients with bilateral aneurysms underwent coil or plug occlusion of one IIA, while the other was preserved using an IBSG. In Group UB, patients with unilateral iliac artery aneurysms received IBSG implantation to preserve the IIA on the affected side. In Group UU, patients with unilateral aneurysms underwent coil or plug occlusion of the IIA on the affected side.

Treatment approaches for the internal iliac artery in patient sample.
To minimize confounding factors, propensity score matching was used to match the preoperative demographic, comorbidity, and aneurysm anatomical characteristics of patients in Group BB with those in Group BU, and Group UB with those in Group UU. The follow-up outcomes of Group BB versus Group BU and Group UB versus Group UU were evaluated and compared. This study was conducted in full compliance with the ethical principles of the Declaration of Helsinki (1975) and its subsequent amendments through 2024. The study reporting adheres to and conforms to STROBE guidelines. 16 The institutional review board at the Affiliated Hospital of Qingdao University approved all study procedures (IRB Approval QYFYWZLL29555). This retrospective study used fully anonymized patient data with all identifiers removed. Verbal consent was obtained where possible, with written consent waived per IRB approval given the study's retrospective nature and complete de-identification.
Treatment and follow-up
In this study, the types of IBSGs used by the enrolled patients were the Cook Zenith® Iliac Branch Device (Cook Medical Inc., Bloomington, IN, USA) and the GORE® EXCLUDER® Iliac Branch Endoprosthesis (W.L. Gore & Associates, Flagstaff, AZ, USA). The bridging stents used in this study included the GORE VIABAHN VBX Balloon-Expandable Endoprosthesis, the GORE® EXCLUDER® Internal Iliac Component (specifically the self-expanding endograft designed for the GORE® EXCLUDER® Iliac Branch Endoprosthesis), and the Zenith Branch Endovascular Graft-Iliac Bifurcation. Both devices were used in strict accordance with their respective Instructions for Use. Postoperatively, patients received antiplatelet monotherapy with aspirin and lipid-lowering therapy with statins.
All four participating vascular surgery centers implemented standardized postoperative surveillance protocols. Patients underwent computed tomography angiography (CTA) at 1, 3, 6, and 12 months postoperatively, with annual CTA examinations thereafter. For low-risk patients, annual duplex ultrasound surveillance was alternatively employed. All imaging studies were systematically reviewed by senior vascular surgeons with >10 years of clinical experience. During scheduled outpatient visits, comprehensive clinical evaluations were performed for all patients, irrespective of IIA preservation status. Systematic assessments documented new-onset symptoms, including buttock claudication, sexual dysfunction, colonic ischemia, and spinal cord ischemia. Patient demographic characteristics and comorbidities were extracted from electronic medical records and hospitalization data. Additionally, structured telephone follow-ups were conducted with all patients or their designated family members to systematically record symptom progression using standardized questionnaires. To accurately assess sexual dysfunction, all male patients in this study were asked to complete the International Index of Erectile Function-5 (IIEF-5), 17 a five-question questionnaire; each item is scored on a 5-point ordinal scale, with the lower value representing poorer sexual function. The possible scores on the IIEF-5 range from 5 to 25 (with a one-question score ranging from 1 to 5), with scores higher than 22 considered normal erectile function. Erectile function at or below this threshold is considered ED. According to the scale, ED is categorized into four categories based on IIEF-5 scores: severe (5–7), moderate (8–11), mild to moderate (12–16), mild (17–21), and no ED (22–25). 18 Questionnaires were administered to all patients during both preoperative and final postoperative follow-up visits, conducted through outpatient clinics and telephone interviews. Throughout this process, all patients’ personal information remained strictly confidential.
Endpoints and definitions
This study was conducted in strict accordance with the reporting standards for endovascular aortic repair. 19 The primary endpoint was major adverse events, which included type I and type III endoleaks, stent migration, aneurysm sac dilation, aneurysm rupture, and aneurysm-related death. The secondary endpoint was the occurrence of postoperative incidence of pelvic ischemia, including buttock claudication, sexual dysfunction, colonic ischemia, or spinal cord ischemia. Technical success was defined as successful implantation of the stent graft without any unplanned procedures or additional interventions, with immediate postoperative angiography showing no endoleak and patent IIAs. Internal iliac artery occlusion is defined as the absence of antegrade flow distal to embolic material in the IIA on postoperative imaging. Buttock claudication is defined as walking-induced hip pain that forces the patient to stop for a specific distance and time and excludes intermittent claudication due to neurological, lower extremity vascular, as well as cardiopulmonary conditions. Sexual dysfunction was defined as an IIEF-5 questionnaire score <22 and decreased erectile function was defined as a decrease from the postoperative IIEF-5 ratings, for example, mild erectile dysfunction preoperatively (17–21) versus mild-to-moderate erectile dysfunction postoperatively (12–16). Spinal cord ischemia was defined as sciatic nerve palsy or paraplegia of more than 24 h excluding lumbar spine causes. Reintervention refers to any subsequent surgical or endovascular procedure performed after the initial surgery to improve clinical outcomes or manage complications related to the stent or aneurysm. Stent migration was defined as a longitudinal movement of the stent graft ≥5 mm relative to the anatomical markers. Aneurysm dilation was defined as an increase in the aneurysm diameter ≥5 mm.
Statistical analysis and propensity score matching
Categorical variables are presented as numbers (%) and continuous variables as mean ± standard deviation. Chi-square test and Fisher's exact test were used for comparing categorical variables, while Mann–Whitney U test was used for comparing continuous variables. Kaplan–Meier analysis was used to estimate freedom from endoleak, secondary interventions, buttock claudication, and erectile dysfunction. Statistical analysis was performed using SPSS 26 software (IBM Corporation, New York), with a matching tolerance (caliper) of 0.02. The propensity score matching plugin in SPSS 26 was used to match the preoperative demographic, comorbidity, and aneurysm anatomical characteristics of Group BB with Group BU, and Group UU with Group UB. Two-tailed tests were used for significance testing, and statistical significance was defined as p < 0.05. The prematching demographic characteristics, comorbidities, and aneurysm morphology of Group BB versus Group BU, and Group UB versus Group UU are summarized in Table 1. Variables with p < 0.05 in the preliminary statistical tests were considered as confounding factors. In Groups BB and BU, chronic obstructive pulmonary disease (p = 0.014) and heart disease (p = 0.015) were considered confounding factors. In Groups UB and UU, hyperlipidemia (p = 0.019), diabetes (p = 0.027), left common iliac artery diameter (p = 0.010), and right common iliac artery diameter (p = 0.045) were defined as confounding factors. After propensity score matching, 38 patients in Group BB were successfully matched with 38 patients in Group BU, and 55 patients in Group UB were successfully matched with 55 patients in Group UU. Table 2 summarizes the postmatching demographic characteristics, comorbidities, and aneurysm morphology.
Demographic, comorbidity, and aneurysm morphology before propensity score matching.

Comorbidities are defined based on the patient's examination and laboratory results at admission, as well as history inquiries.
COPD: chronic obstructive pulmonary disease; PAOD: peripheral arterial occlusive disease; CIA: common iliac artery.
Demographic, comorbidity, and aneurysm morphology after propensity score matching.

Comorbidities are defined based on the patient's examination and laboratory results at admission, as well as history inquiries.
COPD: chronic obstructive pulmonary disease; PAOD: peripheral arterial occlusive disease; CIA: common iliac artery.
Results
After propensity score matching, 38 patients were included in each of Group BB and Group BU, with a mean follow-up of 24.0 ± 7.0 months. In Group BB, patients had a mean age of 63.37 ± 8.43 years, including 34 males (89.5%), with 76 IBSGs implanted. Group BU patients had a mean age of 65.18 ± 8.00 years, including 36 males (89.5%), with 38 stent grafts implanted.
In Group UB, 55 patients were matched with 55 Group UU patients (mean follow-up 23.0 ± 6.0 months). Group UB had a mean age of 65.62 ± 10.56 years with 51 males (92.7%) and 55 IBSGs implanted. Group UU patients averaged 66.18 ± 9.53 years with 50 males (90.9%).
Overall, 131 patients received 169 IBSGs for IIA preservation, including 162 GORE EXCLUDER Iliac Branch Endoprostheses and 7 Cook Zenith Iliac Branch Devices. Bilateral IBSG implantation (Group BB) showed significantly longer operative duration (p < 0.05), with 10.4 min increased fluoroscopy time versus Group BU. Group UB and UU showed no significant differences in procedural time metrics. Procedural details are presented in Table 3. Figure 3 demonstrated an IBSG patency rate of 93.89% per patient (123/131) and 95.27% per implanted stent grafts (161/169).

Kaplan–Meier curve of iliac branch stent graft patency.
Procedural characteristics by treatment group.

Primary endpoint
Group BB versus Group BU (with an average follow-up of 24.0 ± 7.0 months)
Patients in both Group BB and Group BU had abdominal aortic aneurysms with bilateral iliac artery involvement. During the study period, five cases of IBSG occlusion were observed in both groups, as revealed by CT angiography, all of which were caused by thrombosis formation. Three cases (7.9%) occurred in the BB group (all unilateral occlusions), while two cases (5.3%) occurred in the BU group (Table 4). Notably, in the BB group, one patient experienced IBSG occlusion and sought medical attention due to buttock claudication. All occluded patients underwent endovascular reintervention.
Comparison of major adverse events and target organ ischemia between Group BB and Group BU, as well as between Group UB and Group UU.

In Group BB, two patients (5.3%) experienced type IB and type III endoleaks within one year postoperatively. In these cases, one patient experienced a type IB endoleak due to inadequate sealing of the IIA section of the branch stent graft, while the other patient experienced a type III endoleak due to stent graft migration. Both patients showed good treatment response after reintervention. The incidence of endoleaks in Group BU was lower, with one patient (2.6%) identified with type IA endoleak during the 12-month CTA follow-up. The difference in endoleak between Groups BB and BU was not statistically significant (Figure 4A, log-rank p = 0.553). One patient (2.6%) in Group BB and 1 patient (2.6%) in Group BU had stent migration during the one-year follow-up (Table 4, p > 0.05). In the Group BB, stent migration occurred with disconnection of the short limb of the IBSG from the bridging stent, associated with a type III endoleak. In the Group BU, proximal landing zone migration resulted in a type IA endoleak. In Group BB, two patients (5.3%) showed aneurysm dilation (>5 mm), while in Group BU, three patients (7.9%) experienced aneurysm dilation (Table 4, p > 0.05). During the entire follow-up period, no cases of aneurysm rupture or patient deaths were observed in either the BB or BU group. Kaplan–Meier analysis (Figure 4B) revealed no statistically significant difference in reintervention between the study groups (log-rank p = 0.438). Five patients (13.2%) in Group BB and three patients (7.9%) in Group BU received additional treatment due to IBSG occlusion, endoleak, and stent migration, respectively.
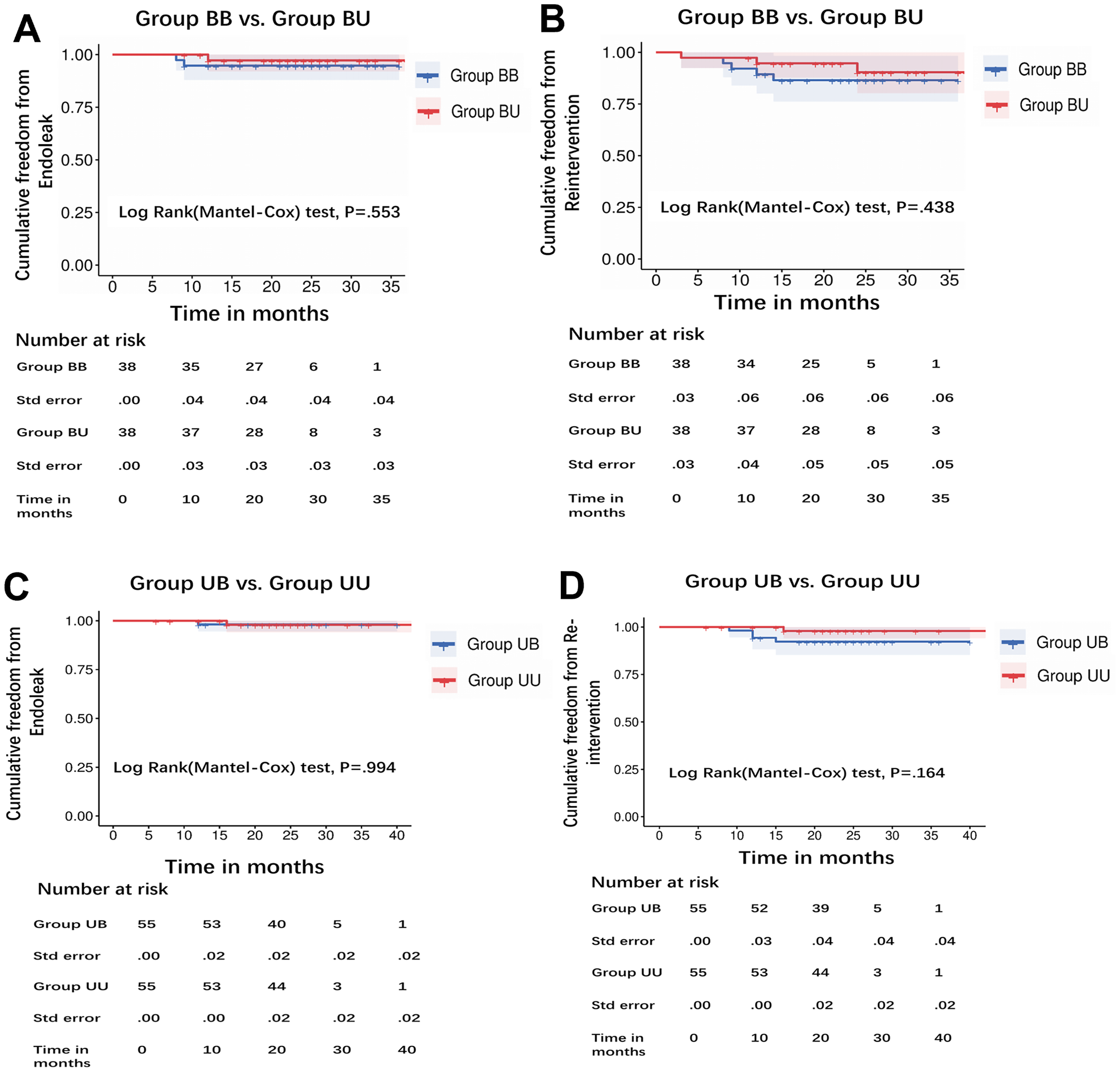
Kaplan–Meier analysis comparing cumulative endoleak incidence and cumulative reintervention rates in Group BB versus Group BU, Group UB versus Group UU.
Group UB versus Group UU (with an average follow-up of 23.0 ± 6.0 months)
Group UB and Group UU consisted of patients with abdominal aortic aneurysms concomitant with unilateral iliac artery aneurysms. Three patients (5.5%) in the UB group experienced IBSG occlusion (Table 4). Thrombolytic therapy restored stent patency. Survival analysis (Figure 4C) demonstrated no statistically significant difference in type I and III endoleaks between Group UB and Group UU (log-rank p = 0.994). In Group UB, one patient (1.8%) was found to have a type IA endoleak during the 1-year follow-up, caused by inadequate sealing at the proximal end of the stent graft. Additionally, expansion of the aneurysmal sac was observed. In Group UU, one patient (1.8%) experienced stent displacement and concomitant type IA endoleak during the 16-month follow-up period after surgery. The endoleak resolved after implanting a CUFF. During the follow-up period, no cases of type III endoleak were observed in any of the patients. Two patients (3.6%) in Group UB developed aneurysmal sac dilation, one of whom had previously experienced an endoleak (p > 0.05). The reintervention rate was higher in Group UB compared to Group UU (4, 7.3% vs. 1, 1.8%), but the difference was not statistically significant (log-rank p = 0.164, Figure 4D). No aneurysm ruptures or aneurysm-related deaths were reported in either group.
Secondary endpoint
Group BB versus Group BU
Regarding buttock claudication, one patient (2.6%) in Group BB and ten patients (26.3%) in Group BU reported symptoms (Figure 5A, log-rank p = 0.003). It is worth noting that the patient in Group BB who experienced buttock claudication had occlusion of the IIA of the IBSG due to thrombosis. During the study period, two patients (5.3%) in Group BB showed a decrease in IIEF-5 classification, while a total of 12 patients (31.6%) in Group BU showed a decrease (Table 4, p < 0.05). Among the twelve patients with decreased sexual function, six (15.8%) developed new-onset erectile dysfunction (Figure 5B, log-rank p = 0.029). No cases of spinal cord ischemia or ischemic colitis were reported in either group.

Kaplan–Meier curves of cumulative incidence of buttock claudication and cumulative erectile dysfunction.
Group UB versus Group UU
During the follow-up period, one patient (1.8%) in Group UB complained of buttock claudication, with thrombosis of the IBSG. In contrast, 13 patients (23.6%) in Group UU reported buttock claudication, and a significant difference in buttock claudication was observed between the groups (Figure 5C, p = 0.001). Regarding sexual dysfunction, two patients (5.3%) in Group UB showed a reduction in IIEF-5 classification, with one patient (1.8%) reporting new erectile dysfunction after surgery. Additionally, 14 patients (25.5%) in Group UU showed a reduction in IIEF-5 classification during the follow-up period (Table 4, p < 0.05). Among these 14 patients with decreased sexual function, nine (16.4%) experienced new erectile dysfunction. Survival analysis (Figure 5D) demonstrated a statistically significant difference between the two groups (log-rank p = 0.007). No cases of colonic ischemia or spinal cord ischemia were reported in either Group UB or Group UU.
Discussion
In recent years, the use of IBSGs has emerged as an important method for preserving the IIA in the treatment of iliac artery aneurysms. 20 Compared to other techniques, IBSGs offer a favorable freedom-from-reintervention rate and superior durability. 21 Van der Veen et al. reported 12-month follow-up results from 100 patients treated with the Gore Excluder IBE, demonstrating a patency rate of 91.3% and an IBE-related reintervention rate of 7%. 22 In our study, we observed a patency rate of 93.89% for the IBSG during midterm follow-up (Figure 3). No significant differences were found in major adverse events, including endoleaks, stent migration, and reintervention, between Group BB and Group BU, or between Group UB and Group UU. These findings suggest that the use of IBSGs to preserve the IIA is both safe and effective.
Bilateral IIA occlusion can lead to a higher incidence of buttock claudication and more severe ischemic symptoms. Previous studies have suggested that sacrificing one side of the IIA is relatively safe. 23 However, from an anatomical perspective, the IIA is the main blood supply to the pelvic organs, and the gluteal muscles primarily receive their blood supply from the ipsilateral IIA. Occlusion of either side carries the risk of ipsilateral gluteal muscle atrophy or even necrosis, significantly compromising the postoperative quality of life for patients. A previous meta-analysis showed that approximately 27% of patients with unilateral IIA flow interruption experienced buttock claudication.10,24 A prospective comparative study by Rafael de Athayde Soares et al. demonstrated that preservation of bilateral IIAs significantly reduces pelvic ischemic complications and improves survival rates following EVAR. 25 In our study, unilateral IIA occlusion was still associated with a considerable risk of buttock claudication, with 26.3% and 23.6% of patients in Groups BU and UU, respectively, reporting symptoms. In contrast, preservation of bilateral IIAs (Groups BB and UB) significantly reduced the incidence of buttock claudication (p < 0.05). These findings are consistent with the conclusions of Taudorf et al. and Verzini et al., whose comparative studies also suggested that preserving the IIA using IBSGs can effectively prevent ischemia-induced buttock claudication.26,27 For patients with bilateral iliac artery aneurysms, midterm follow-up results demonstrated comparable safety profiles between unilateral and bilateral IBSGs implantation in Groups BB and BU, with no significant differences in major adverse events. This finding is supported by the pELVIS international multicenter registry study, which confirmed that simultaneous bilateral IBSG implantation represents a safe and feasible technique with reduced IBSG-related adverse events during midterm follow-up. 28 Further validation comes from the single-center study by D'Oria et al., which established the safety and feasibility of IBSG implantation while reporting comparable reintervention rates between bilateral and unilateral approaches. 29 Based on these collective findings, current evidence strongly supports preserving bilateral IIA perfusion whenever possible to optimize postoperative mobility and quality of life.
Recent evidence has established percutaneous endovascular angioplasty as an effective intervention for vasculogenic erectile dysfunction.30,31 The primary vascular supply to the penis typically originates from the internal pudendal artery, a branch derived from the IIA. The utilization of IBSG for preserving the IIA follows a similar principle, with the goal of preserving sufficient blood supply to the genital organs and enhancing patient satisfaction with their sexual life. Among the patients in the BU and UU groups, we noted a higher proportion experiencing a pronounced reduction in erectile function following surgery (BU group: 12/38, 31.6%; UU group: 14/55, 25.5%). This functional decline was objectively assessed using the IIEF-5 questionnaire, which provides validated quantification of postoperative changes. Among patients with preserved bilateral IIA perfusion, only two cases of erectile dysfunction were documented. Furthermore, among patients with unilateral occlusion of the IIA, 15.8% of those (6/38) with bilateral aneurysms and 16.4% of those (9/55) with unilateral aneurysms experienced newly developed erectile dysfunction. These findings underscore the critical importance of maintaining bilateral IIA perfusion in AIA repair to ensure adequate genital organ blood flow and preserve postoperative sexual function. While current sexual dysfunction assessments primarily evaluate male patients, emerging evidence suggests that IIA preservation in female patients may prevent complications such as vaginal dryness. 32
Although unilateral IIA occlusion resulting in colonic ischemia represents a relatively uncommon complication, it is associated with disproportionately severe clinical outcomes following endovascular aortic repair. This is exemplified by the two fatal cases of pelvic ischemia complications post-EVAR reported by Elixène Jean-Baptiste et al. 33 Anatomically, the IIA serves not only as the primary vascular supply to pelvic organs but also constitutes a critical component of the spinal cord collateral circulation network. This dual vascular function assumes particular significance in patients with concurrent thoracoabdominal aortic aneurysms undergoing thoracic endovascular aortic repair, where maintaining IIA patency has been demonstrated to substantially reduce spinal cord ischemia risk. 34 In cases of preexisting severe IIA stenosis or occlusion, preservation of the contralateral IIA provides vital collateral flow pathways, thereby mitigating risks of both colonic ischemia and spinal cord injury while significantly improving long-term patient prognosis.
Limitations of the study
The evidence strength of retrospective nonrandomized studies is weaker than that of randomized controlled trials. The midterm follow-up period in our study provides only midterm evidence. Although propensity score matching and stratified analysis provide more direct evidence, they may result in loss of patient samples.
Conclusion
In the management of AIAs, the IBSG technique has demonstrated excellent midterm patency rates when bilateral IIA preservation is achieved. Clinical evidence suggests this approach not only maintains pelvic perfusion but also significantly preserves both lower limb functionality and sexual function postintervention. For patients meeting appropriate anatomical criteria, complete bilateral IIA preservation should be considered the preferred therapeutic strategy whenever technically feasible.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Deidentified data supporting findings are available from corresponding author upon reasonable request, subject to institutional approvals.