
Abstract
The complexity of chronic kidney disease (CKD) and its treatments have made self-management behaviors inevitably challenging. However, supplementing education with self-management skills may improve numerous health outcomes in people with nondialysis CKD. This study protocol describes a randomized controlled trial (RCT) aimed to evaluate the effects of a nurse-led self-management support program as an intervention for kidney disease knowledge and CKD self-management behaviors among people with pre-dialysis CKD. In Phase 1, people with CKD stage 3–4 and their family members are involved in co-designing, development and pilot testing of a theory-based self-management intervention. In Phase 2, we perform a cross-cultural adaptation of the Kidney Disease Knowledge Survey, CKD Self-Management and Self-efficacy for Managing Chronic Disease questionnaires. In Phase 3, a parallel RCT will be conducted to evaluate the intervention where 154 participants with CKD stage 3–4 will be randomly assigned to either the intervention (n = 77) or control group (n = 77). The intervention group will receive 6-week self-management program from a nurse-coach in addition to standard usual care, while the control group will receive only standard usual care. Outcome measures include kidney disease knowledge, CKD self-management behavior, self-efficacy, quality of life, blood pressure control and adherence to CKD diet as indicated by 24-h urine urea nitrogen, 24-h urine sodium and net endogenous acid production. Data will be collected at baseline and 12-week post-baseline. The between- and within-group intervention effects will be estimated using the Generalized Estimating Equations. The self-management intervention offers strategies to delay CKD progression and to encourage motivation to better self-manage at home. This study integrates self-management education and psychosocial support with culturally relevant scenarios, and evaluates important self-reported and objective outcomes.
Clinical Trials Registration: www.ClinicalTrials.gov, identifier: NCT03974646.
Keywords
Introduction
Chronic kidney disease (CKD) is a highly distressing chronic disease as it complicates normal life routines, increases health risk, reduces the quality of life (QoL), and increases treatment cost. 1 The most widely used definition of CKD is decreased kidney function as indicated by glomerular filtration rate (eGFR) ≤60 mL/min per 1.73 m2, or the presence of kidney damage, or both, for at least 3 months, regardless of the underlying cause. 2 CKD is classified into Stages 1–5 according to the eGFR. Stage 5 CKD, also termed as end-stage kidney disease (ESKD), is when renal replacement therapy (RRT) is required to sustain life. 2
Globally, the prevalence of CKD is estimated to be 13.4% for Stages 1–5, in which as high as 10.6% are patients with Stages 3–5. 3 The risks for cardiovascular disease (CVD) morbidity and all-cause mortality are high across all stages of CKD. 4 With an increasing mortality rate, CKD was the thirteenth leading cause of death in 2013, a rise of 134% compared to its ranking of 27 in 1990. 5 Similarly, the Global Burden of Disease (GBD) reported that about 1.2 million people died from kidney failure in 2015; an increase of 32% compared to 2005. 6 Overall, an estimated of 5–10 million people die annually from kidney disease, 7 while another 2.3–7.1 million people with end-stage CKD (ESKD) are living without any access to chronic dialysis. 8 As diabetes is a common risk factor of CKD, up to 15%–20% and 30%–40% of people with type 1 and 2 diabetes have ESKD respectively. 9 In Malaysia, CKD is among the top ten causes of mortality. 10 The CKD prevalence in 2018 was 15.48%, 11 an increase from 9.07% in 2011. 12 Of the total number, approximately 3.85%, 4.82%, 6.48% of them suffer from CKD Stages 1, 2, and 3 respectively. Another 0.33% are in CKD Stages 4–5. 11 In 2015, the estimated dialysis cost for 38,000 people was RM1.5 billion (USD 281.43 million). With the increasing prevalence and severity of CKD, the cost is projected to increase to RM2 billion (USD 487.61 million) in 2025 and RM4 billion (USD 796.87 million) in 2040. 13
CKD is a progressive condition that can impact the patients’ physical, psychological, and social well-being. 14 Many people with CKD only have non-specific symptoms at the early stage of the disease. 2 Therefore, the diagnosis of CKD is frequently made late when symptoms caused by CKD complications, specifically anemia, fluid overload, and uremia appear at the later CKD stages, typically Stage 3b and beyond.15,16 The complexity of CKD and its treatments often involve behavioral self-management that can be challenging. People living with CKD need to manage multiple medications, adhere to diet and lifestyle modifications, negotiate psychosocial support, and navigate the challenging health systems.17,18 Studies have shown that besides timely clinical screening and treatment, the impact and risks of CKD can also be mitigated through lifestyle changes, effective self-management of symptoms, treatment compliance, and appropriate psychosocial and physical coping strategies.19,20
Based on the Social Cognitive Theory, any intervention strategies must first address potential limitations in the knowledge and self-efficacy among the target population. 21 Studies in the literature demonstrated that the Social Cognitive Theory is effective in enhancing CKD self-management by strengthening the knowledge and self-efficacy of the people.21,22 Therefore, it is likely that the empowerment of people with CKD by providing them with sufficient information can improve their disease-specific knowledge and confidence to better self-manage CKD. Subsequently, this will improve their overall health and well-being. Globally, self-management behaviors play a significant role in delaying the progression of CKD. 23 To achieve this, the needs of people with non-dialysis dependent CKD and their caregivers must be identified so that viable strategies can be developed to assist them in managing their health conditions to prevent worsening of CKD.
Due to the progressive nature of CKD, it is imperative to nip the problem at its bud. Studies in Australia and Vietnam have shown that self-management interventions during the early CKD stages can enhance self-efficacy, knowledge, self-management, health-related QoL (HRQoL),21,22,24 and physiological outcomes (eGFR and blood pressure [BP]). 22 Furthermore, pre-dialysis educational interventions for people to self-manage their CKD can slow the disease progression, delay the need for Renal Replacement Therapy (RRT) by a median of 17.0 months, and extend survival (median survival of pre-dialysis is 2.25 years) when compared to usual care.25,26 Systematic reviews have also reported that self-management support programs that aimed at improving kidney disease knowledge, modifying nutrition/diet, promoting lifestyle and symptoms management were effective in slowing the CKD progression.27–29 The programs were commonly delivered either face-to-face individually or in a group session, or via a combination of face-to-face and telephone sessions. All of these methods were found to be acceptable.27,30,31
A recent systemic review of 19 randomized controlled trials (RCTs) on self-management intervention in people with non-dialysis dependent CKD has reported that comprehensive intervention (lifestyle modifications combined with medical behavior changes) conducted by medical professionals such as dieticians, nurses, doctors, and certified exercise physiologists to be effective in improving exercise capacity, lowering BP, C-reactive protein levels, and urine protein. 32 However, there was heterogeneity in the included studies and the best health behaviors are still unclear. 32
Some evidence points out that theory-based interventions can be more effective than their non-theoretical counterparts. However, the limited literature on the self-management interventions for those with earlier stages of CKD suffers from significant methodological and theoretical limitations. In Malaysia, people who are at risk of developing CKD are not well informed on CKD and they also tend to have poor self-management behaviors.33,34 Besides, there is limited evidence to support the effectiveness of clinical practices in delivering nurse-led self-management support programs for people with earlier CKD stages as most of the published studies focused on patients receiving hemodialysis. In reality, the strategies used to improve self-management behavior are likely to vary in terms of the format, content, and delivery for different groups of patients.
This study aims to engage people with CKD and those involved in their care such as renal nurses, nephrologists, and family physicians to co-design a self-management intervention that incorporates both the patients’ cultural values and psychosocial needs based on the behavioral change theory. 28 Self-management is not merely an individual issue and should be considered in a broader context. Consistent with this, people with chronic diseases recognize the importance of educating their close ones (family and/or friends) regarding their disease and its treatment, and champion for their inclusion in medical appointments and other decision-making processes. 35 Thus, the involvement of family members as facilitators is beneficial in helping those with CKD to maintain a positive approach to self-management such as physical activity, diet, and medication. Useful resources such as printed materials must be made easily available to them to encourage their inclusion in self-management education sessions. With the support of their family members, people with CKD will be more motivated to participate in the self-management support program.
Conceptual framework
Self-management involves an understanding of the self-management strategies and having the confidence (self-efficacy) in applying these strategies to manage the disease. The Social Cognitive Theory (SCT), also known as the self-efficacy theory, 36 will be used to guide the development of the study intervention to fit in with the local context in Malaysia (Figure 1). 36 As self-efficacy may influence behavioral change, the Social Cognitive Theory has been used extensively to understand CKD self-management behaviors.21,22 The term ‘self-efficacy’ denotes a person’s faith in their ability to achieve a goal such as managing their health effectively. It is not static and can be enhanced in four main ways via self-appraisal, vicarious experience, performance accomplishment, and verbal persuasion. Firstly, self-efficacy can also be modified via self-appraisal. Self-appraisal refers to the self-evaluation of one’s physiological and emotional states and his or her abilities to perform certain behaviors. 36 Self-efficacy can also be attained via vicarious experience that involves the observation of how people similar to themselves perform the tasks successfully. Observing a role model who successfully performs a difficult behavior can enhance another person’s level of self-efficacy. Next, performance accomplishment serves as an effective strategy that comes from within a person who has mastered that behavior (or experience) and felt a sense of success. 36 Self-efficacy can also be modified via verbal persuasion. This is frequently achieved by providing verbal instructions, suggestions, and advice that can convince a person to perform new (or modified) behaviors. 36
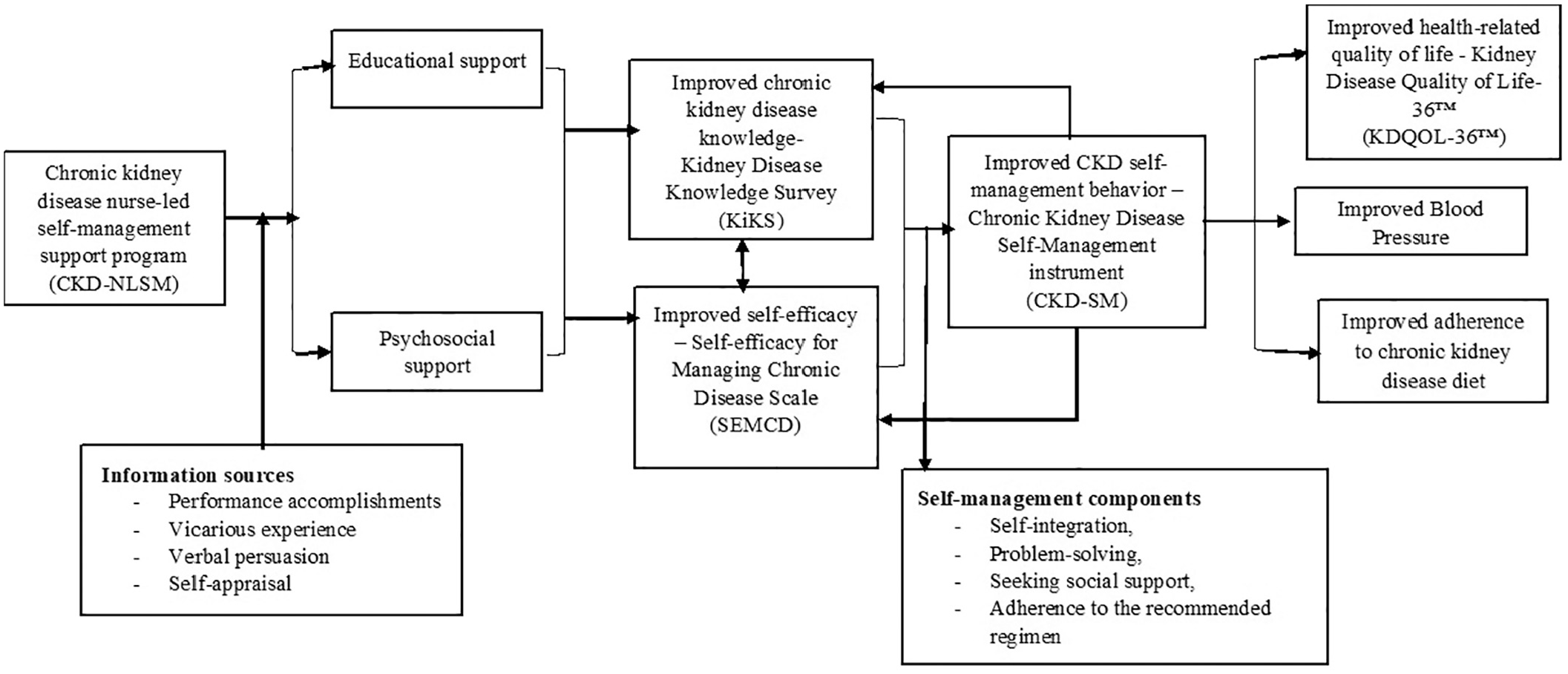
Conceptual framework.
This study intends to examine the effects of a 12-week structured nurse-led educational program for people with CKD Stages 3–4 in improving kidney disease knowledge and self-efficacy, self-management behavior, QoL, BP control, and adherence to CKD diet. Therefore, this protocol set out to describe the design, setting, intervention, and outcomes of the study.
Materials and methods
Overall research design and phases
This study applies a multi-phase development, implementation, and evaluation design. Three phases are planned to achieve the study aims. Phase 1 involved people with CKD Stage 3–4 and their family members in the co-designing, development, and pilot testing of the theory-based self-management intervention to be used in this study. These patients and their accompanying family members were engaged in informal meetings at the clinics or wards, and formally during the face and content validity testing of the questionnaires. In Phase 2, a cross-cultural adaptation of the three instruments will be done, including the Kidney Disease Knowledge Survey (KiKS), 37 the CKD Self-Management (CKD-SM), 38 and the Self-efficacy for Managing Chronic Disease (SEMCD). 39 For this, the content validity was first tested by a committee of experts consisting of a nephrologist, two family medicine specialists, two nursing academicians, three renal nurses, and three people with CKD. Forward and backward translations was done for the three questionnaires (Figure 2). After that, the psychometric property of the questionnaires will be tested for their internal consistency, construct validity, test-retest ability, and responsiveness according to the COSMIN taxonomy of measurement properties. 40 In Phase 3, a parallel RCT will be conducted to evaluate the intervention developed from Phase 1 to determine the effectiveness of a theory-driven, nurse-led self-management support program for people with CKD Stages 3–4 (the CKD-NLSM) compared to standard usual care. In addition, the data from the baseline and the first session in the RCT will be used for reliability testing whereas the data from the baseline and the final outcome evaluation will be used to test the responsiveness of the questionnaires. This approach of combining the questionnaire validation process in the RCT is appropriate as there are no relevant validated tools available in the Malay language. The study protocol adheres to the Standard Protocol Items: Recommendations for Intervention Trials (SPIRIT) reporting guidelines. 41 A checklist for SPIRIT is provided as supplemental material.

Translation and validation process.
Phase 1: Co-design of the CKD-NLSM support program intervention with patients
Phase 1 aims to investigate the desires of people with CKD in receiving self-management support and the best manner to incorporate them in the co-design and development of a new intervention to improve self-management based on the behavior-change theory. In other words, what are the strategies and topics identified by people with CKD to be important elements in an intervention that aims at effectively support them to engage in self-management? How and when would people with CKD prefer a self-management intervention to be implemented (e.g. format, educator, location, time, etc.)? Before obtaining the input from people with CKD, the literature review was conducted to identify the important aspects of self-management deemed to be needing more support by people with CKD.24,42 Previously identified aspects include obtaining disease-specific knowledge, managing medication, engaging and sustaining social support, maintaining social and occupational roles, modifying lifestyle, developing and sustaining a positive attitude, caring for mental and physical wellbeing, building and sustaining effective relationships with healthcare providers, establishing a routine and planning, actively participating in healthcare services, as well as recognizing and effectively responding to symptoms. 42
A formal group-based session and feedback survey to assess the preferences among the target population was conducted in February 2020. Ten potential participants who met the study inclusion criteria were included in the group-based session and completed the feedback survey. They found the CKD-NLSM support program to help provide support in terms of disease symptoms, prognosis, medications, and diets. The findings in this phase are useful to guide the implementation of the self-management program with regard to the format, mode, timing, and educator. In the pilot study, participants have indicated that their preferred mode of delivery is a face-to-face program (with follow-up phone calls) whereas Internet-based delivery would be their last preference. In addition to the interactive sessions, they also desire printed take-home materials that they can later refer to. Some participants reported that they learn to self-manage with others’ experiences, so there may be value in group-based learning. In terms of timing, participants who are working desire evening sessions while those who are not working prefer daytime sessions. Overall, they would prefer to receive self-management support from a nurse’s educators.
Phase 2: Translation and validation of the outcome measures
KiKS, CKD-SM, and SEMCD were subjected to forward and backward translation. After culturally adapted, they will be examined on their psychometric properties.
Outcome measures
Kidney Disease Knowledge Survey (KiKS)
The KiKS is a self-administered tool to measure the knowledge of people with kidney disease who do not require RRT. 37 There are 28 items in the three domains that measure the general knowledge regarding kidney disease, knowledge of kidney functions, knowledge of symptoms of progression. A correct response will be given a score of 1 and an incorrect response will be given a score of 0. The total score ranges between 0 and 28. A higher score represents a higher level of kidney disease knowledge.
Chronic Kidney Disease Self-Management (CKD-SM)
CKD-SM is a self-administered tool that is used to examine the self-management behavior in people with CKD. 38 It has 29 items with four domains, namely self-integration, problem-solving, seeking social support, and adherence to the recommended regimen. The first domain of self-integration has 11 items reflecting on how a person may attain a balanced life through lifestyle adjustment by embedding the prescribed self-management activities and treatment regimens. Next, the domain of problem-solving includes nine items that examine a person’s ability to search resources and obtain information on the disease to address their disease-related issues. Thirdly, under the domain of seeking support, five items assess a person’s ability to seek support from significant others to overcome disease-related issues. Lastly, the domain of adherence to recommended regimens includes four items to determine if a person adheres to the prescribed treatment regimens. A four-point Likert scale is used for each item, ranging between 1 (never) and 4 (always). The total scores for self-integration, problem-solving, seeking social support, and adherence to recommended regimen range from 11 to 44, 9 to 36, 5 to 20, and 4 to 16, respectively. The overall score ranges from 29 to 116 whereby a high score indicates better self-management behavior in managing CKD.
Self-efficacy for managing chronic disease (SEMCD)
The SEMCD is a self-administered instrument that measures the self-efficacy of people diagnosed with chronic disease. 39 The tool has four domains, that is, symptom control, role function, emotional functioning, and communication with doctors. 39 There are six items, each measured on a 10-point Likert scale from 1 (not at all confident) to 10 (totally confident). Hence, the total score for each domain ranges from 6 to 60. Higher scores signify higher self-efficacy.
Procedure for translation, cultural adaptation, and validation of the KiKS, CKD-SM, and SEMCD
Permission to use the KiKS, CKD-SM, and SEMCD was obtained from the respective developers. The translation of the English version to Malay was performed in a four-step process according to international guidelines43,44 (Figure 2). First, the original version of the questionnaires is forward translated from English to Malay independently by two professional bilingual native Malay speakers from the Faculty of Languages and Linguistics, University Malaya. The two initial forward translations were then merged to form the Malay version questionnaire that was subsequently evaluated by a panel of ten experts for semantic, idiomatic, and conceptual equivalence. 45 The panel consists of a nephrologist, two family medicine specialists, two nursing academicians with experience in the validation of instruments, two renal nurses, and three people with CKD. They reviewed both translations before discussing in iteration and reaching a consensus on a single version of the Malay questionnaire. In KiKS, for question number 4 (Select the one medication from the list below that a person with chronic kidney disease should avoid), the expert committee proposed that Lisinopril and Tylenol in the answer option should be replaced by Perindopril and Panadol whereas the Motrin/Ibuprofen option should be replaced by Voltaren because patients would be more familiar with these drug names.
Back translation from Malay into English was performed for all questionnaires by another two qualified local bilingual translators from non-medical backgrounds who are blinded to the original English versions. The translation is again discussed by the expert panel to ensure that it is essentially similar to the original questionnaire. Furthermore, the Malay version of the questionnaires are subjected to a cognitive debriefing among ten Malay people with the same eligibility criteria as the RCT participants (see further below). They completed the self-administered questionnaires within 15–30 min. After that, they were asked to comment on the clarity of the words and sentences in the questionnaires, as well as whether it is easily understood and covers all important aspects of kidney disease knowledge, CKD-self-management, and self-efficacy for managing chronic disease. Lastly, the final version of the questionnaires will undergo consistency and validation analysis based on the COSMIN (COnsensus-based Standards for the selection of health Measurement INstruments) approaches, 40 include factor analysis, estimating the internal consistency, intra-rater test-retest reliability, hypothesis testing, and responsiveness.
The sample size will be based on the ratio of 1:10 (10 respondents for every item).45,46 With 29 items in the longest questionnaire CKD-SM, a minimum of 290 participants will be needed. Taking into account a 20% refusal rate and incomplete responses, we plan to approach a total of 363 respondents. Additionally, for the 2-week intra-rater test-retest testing, a sample size of at least 50 participants will be re-invited. 40
A list of eligible patients scheduled for nephrology clinic follow-up at a tertiary hospital in Kuala Lumpur will be first identified from the electronic medical records. The CKD stages are determined by reviewing their most recent eGFR results in the electronic laboratory report. Patients are approached while waiting to see the doctors and those who agree to participate, written informed consent is obtained before answering the questionnaires.
Internal consistency is assessed using Cronbach’s α and the KR-20 coefficient. A coefficient of 0.7–0.9 indicates good internal consistency of the questionnaire. 47 Intra-rater test-retest reliability is performed by estimating the ICC.48,49 Exploratory factor analysis (EFA) will be conducted using principal component analysis and varimax rotation. Items are then screened to identify those with factor loading >0.4. 50 The associations between patient-reported outcome variables will be examined using correlation analysis. 51
Phase 3: RCT evaluating the CKD-NLSM support program effectiveness
Study setting and design
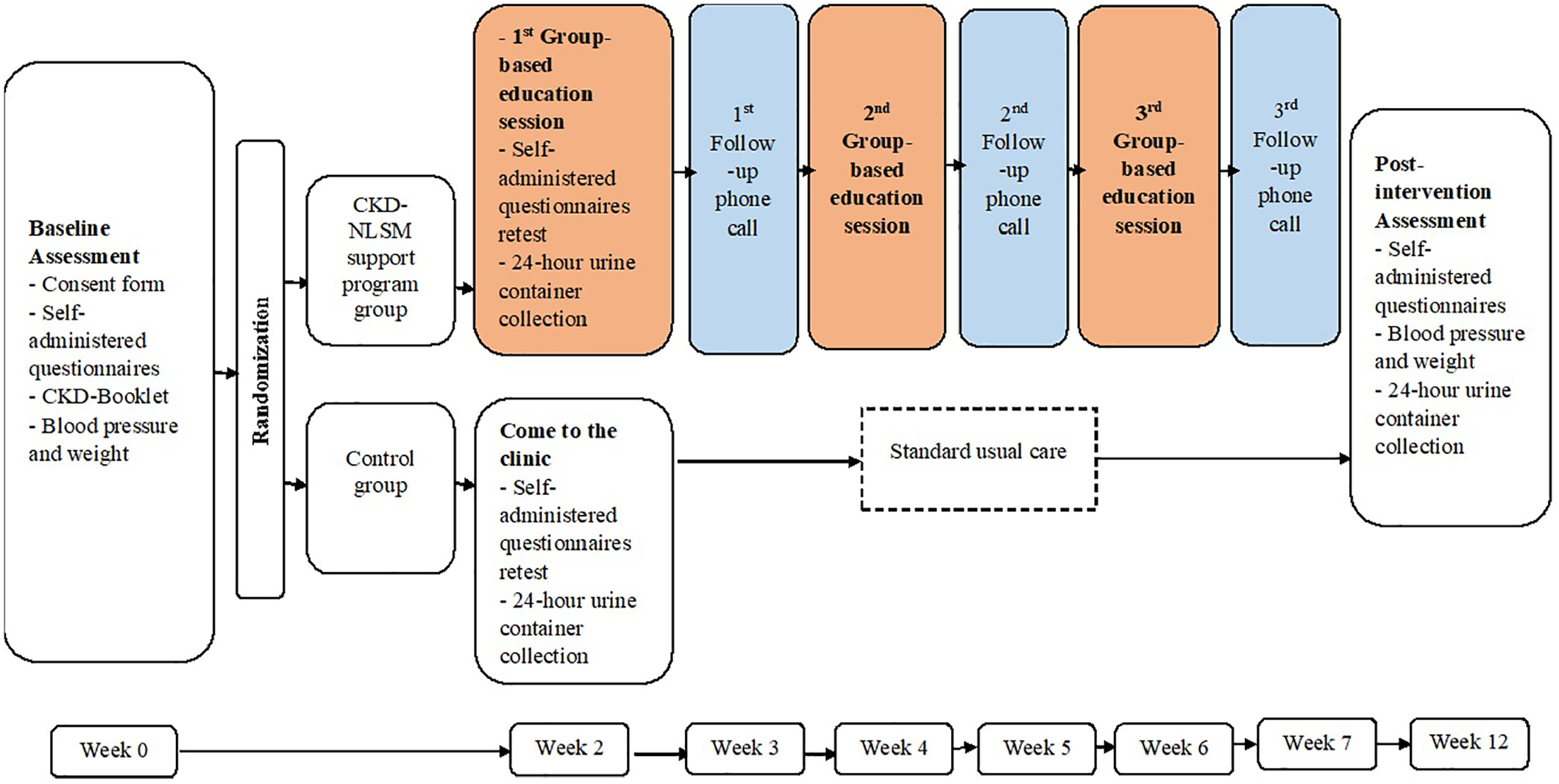
The single-center RCT will be conducted in a tertiary hospital in Kuala Lumpur with a one-to-one allocation into two parallel groups with repeated measures. This study will incorporate an active 6-week CKD-NLSM support program delivered by trained CKD nurse-educators as compared to standard usual care (Figures 3 and 4).

CKD-NLSM support program trial flow chart.
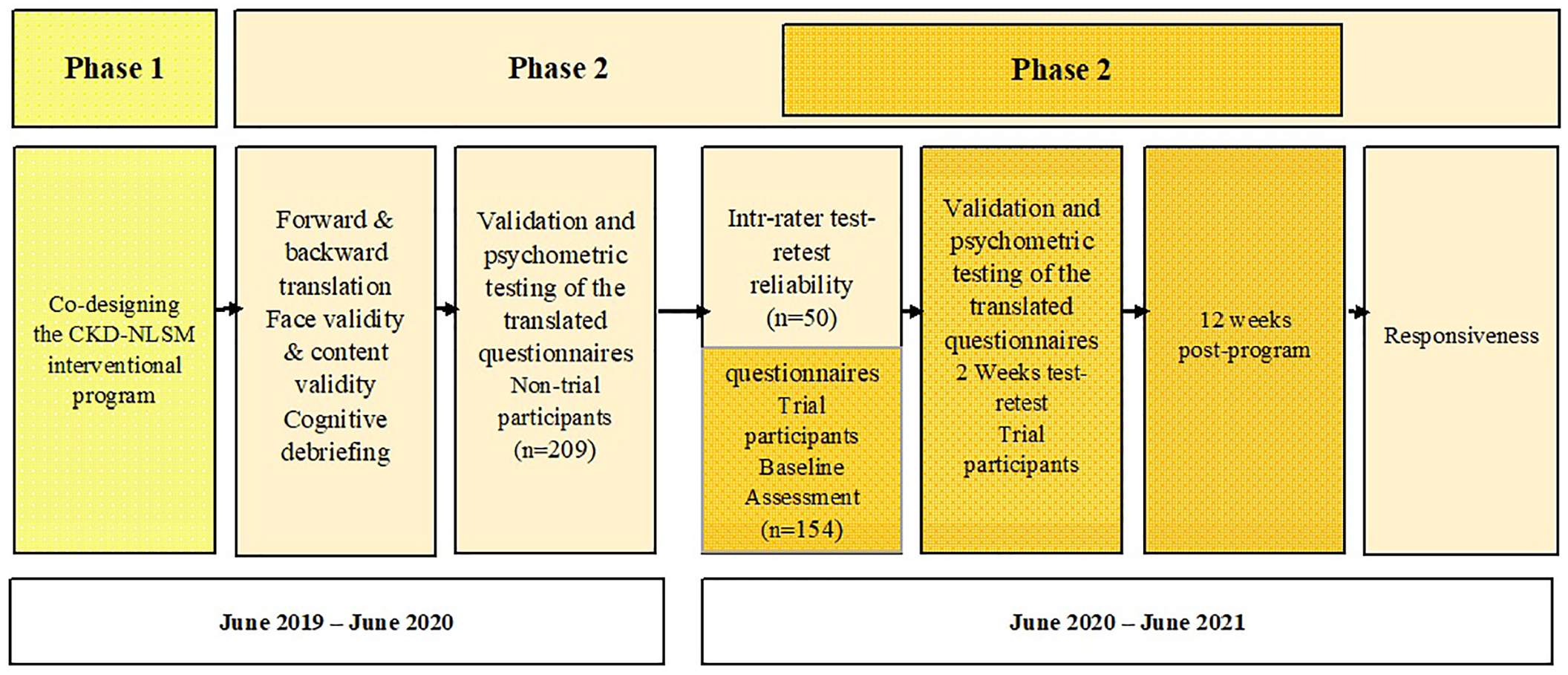
Study phases timeline.
The hypotheses are as follows:
The participants with CKD Stages 3–4 enrolled in the CKD-NLSM support program will demonstrate a significant improvement in their kidney disease knowledge, self-efficacy, CKD self-management behavior, and HRQoL compared to participants who receive the standard usual care.
The participants with CKD Stages 3–4 enrolled in the CKD-NLSM support program will demonstrate a significant improvement in their BP control and adherence to the CKD diet as compared to participants who receive the standard usual care.
Participant
The eligible participants are (a) adults with CKD Stages 3–4 (defined as eGFR of 15–59 mL/min/173 m2 with evidence of kidney damage); (b) age ≥ 18 years; and (c) can speak, read, and understand at least Malay. They should not have any pre-existing cognitive or vision impairment (prohibiting them to see the materials) as well as serious illnesses such as cancer, stroke, and dementia diagnosed and recorded in the medical records. In addition, the participants should not have participated in any structured education program before. Ethical approval was obtained from the Medical Research Ethics Committee of the University Malaya Medical Centre.
Sample size estimation
Sample size calculation was performed using G*Power 3.1 based on the main outcome of improved CKD self-management behavior after 12 weeks of the CKD-NLSM support program. With an effect size of Cohen’s d = 0.5,21,22 a two-tailed alpha value of 0.05, a beta of 0.8, and an attrition rate of 20%, at least 154 patients will be needed (77 patients per group).
Recruitment
The principal investigator and the trained research assistants will review the diagnosis in the medical records to identify the potentially eligible patients scheduled for follow-up at the nephrology clinic. If the diagnosis is unclear, then they will check the laboratory results sections. In addition, they will also determine the CKD stages by reviewing the most recent eGFR result in the electronic laboratory report. All the eligible patients will be approached when attending the nephrology clinic. Patients who agree to participate will receive a patient information sheet containing a full description of the study and be invited to a baseline meeting organized by the CKD nurse-educators. Participants are encouraged to bring along family members or friends if desired. They are reminded that their participation is voluntary and they can withdraw from the study at any time without giving reasons.
Data collection
At the baseline meeting, a detailed briefing on the study will be provided. Patients who agree to participate will provide written consent, complete the demography questionnaire, Malay KiKS, CKD-SM, SEMCD, and Malay Kidney Disease Quality of Life (KDQOL-36™) (see further). 52 Their BP and weight will be measured. Other data including their comorbidities and number of hypertensive medications will be retrieved from the electronic medical records and recorded in the participant’s data collection sheet. The participants will also be given instructions on the collection of 24-h urine to determine the levels of creatinine, urea, protein, sodium, and potassium 2 weeks later. The participants will then be randomly allocated to either the CKD-NLSM support program or the standard usual care group, and the follow-up schedules will be provided. After 2 weeks, when they attend the first group-based education session (intervention group) and return their urine sample (both groups) to the researchers at the hospital, the participants in both groups will again answer the Malay-version of KiKS, CKD-SM and SEMCD for the purpose of intra-rater test-retest reliability testing.
Randomization
Eligible participants will be randomized into two groups using opaque sealed envelopes. All investigators and participants will be blinded to group allocation until after recruitment, consent, and baseline data are collected. The principal investigator will place the code into the envelopes before sealing before confirming that the envelopes are fully opaque to ensure that the codes cannot be seen through the envelopes even when held to the light. The research assistant will shuffle the envelopes before opening to reveal the codes to see if the study participant is allocated either to the control or intervention group. The envelopes are stacked and maintained till the end of randomization.
Blinding
This RCT is an unblinded study due to the nature of the intervention. Neither the researcher nor the participants can be blinded. However, the nurses responsible for taking BP and the laboratory staff will be blinded.
Study intervention
Intervention/issue of interest (exposure)
Participants allocated to the CKD-NLSM group will receive standard usual care, CKD-Booklet, and a 6-week CKD-NLSM support program delivered by two trained CKD nurse-educators (see further below). The CKD-Booklet is translated and adapted with permission from the ‘Living with Reduced Kidney Function’ handbook published by Kidney Health Australia. 53 The CKD-Booklet explains kidney functions, common causes of CKD, and strategies for managing and delaying CKD progression such as adherence to medication, healthy eating, and the benefits of maintaining a healthy lifestyle. The CKD-Booklet also has a diary and note-taking space for participants to record their problems and goals.
The participants in the intervention group will be engaged in three group-based sessions on weeks 2, 4, and 6 from the baseline assessment. Each group-based session will last about 60 min. To ensure the consistency of content delivery, standardized slides are prepared and presented by the CKD nurse-educators. The family members or friends can co-participate in the group-based session. Every session can accommodate about 15 people, including family members and friends. This is the optimal number of participants to allow better opportunities for interactions between CKD nurse-educators and participants, as well as among the participants.
During the first group-based session, a brief explanation of the basic anatomy of the kidney and its functions will be provided, followed by an introduction on the importance of self-management strategies on supporting patients in their applications, which is essential to improve self-efficacy, through the approaches suggested in the Social Cognitive Theory. The second session will focus on the importance of self-management strategies and reinforcement of successful self-management behaviors by providing the necessary support for them to improve self-efficacy. The session will also include the management of medications, diet, and nutrition for kidney health as well as how to live well with reduced kidney function. The CKD nurse-educators will also share the common practices that affect kidney problems to motivate the participants to understand the essential tasks in CKD self-management and to encourage them to focus on achievable tasks. The last group-based session focuses on reinforcing successful self-management behaviors, encouraging participants to continue problem-solving and future planning, as well as discussing myths and facts about CKD. Additional time will be allocated for inquiries about any particular issues that the participants intend to discuss and clarify.
On top of the group sessions, the intervention also includes three individual follow-up phone calls lasting 20–30 min each about a week after each group-based session. In total, there will be three phone calls on alternate weeks. The phone calls will be made by the same CKD nurse-educator who leads the group-based sessions. These phone calls aim at enhancing self-efficacy, monitoring the patients’ self-management, and addressing their problems. The full content of the CKD-NLSM support program is available in the supplemental file.
Comparison
Participants in the control group will receive standard usual care given to people with CKD Stages 3–4 as routinely practiced by the nephrologists at the clinic. The care provided is in accordance with the national clinical practice guidelines, 54 consisting of and is not limited to brief verbal information (2–5 min) on the importance of adherence to medications, dietary restrictions, and lifestyle modifications. As with the intervention group, the participants in the control group will be offered a CKD-Booklet and they are encouraged to read it.
CKD-nurse educators and research assistants training
Two CKD nurse-educators with experience in managing CKD were trained to deliver the intervention. They were informed about the administration of study instruments, data collection methods, and ethical considerations. They are also trained to assist the participants in completing the questionnaires and facilitating the collection of the 24-h urine sample. The competency of the nurses was first tested through pilot testing to ensure their quality. In addition, they were received a printed study manual as the guideline for conducting the interventional program. The guideline provides an overall view of the interventional program, a planned timeline for follow-ups with the participants, and a detailed description of activities and strategies for effective behavioral changes. Moreover, a copy of PowerPoint slides for each group-based session, printed CKD-Booklet for participants, calendar, attendance sheet, and patients’ contact information were also shared with the CKD nurse-educators.
Two research assistants are trained to assist in the study, from patients’ recruitment, randomization, concealed allocation, group session arrangement, to follow-up evaluation. They are given a written manual that contains detailed description and explanation of the study phases including study purpose, method of each phase, the study outcomes, outcome measures, assessment timelines, attendance sheet, list of the participants’ names and their contact information, as well as forms to be completed accordingly.
Pilot study
Prior to the study, the feasibility of the CKD-NLSM support program was tested in a pilot study. Various processes including the recruitment process at the nephrology clinic, access to the electronic medical records, eligibility criteria assessment, patients’ identification at the waiting areas, approaching and conversing with the patients, self-administration of the questionnaires, logistics for safe-keeping of research materials, and feedback on the intervention program were obtained from the patients during the pilot study. Ten patients with similar inclusion and exclusion criteria were invited to the pilot test that consists of a one-day interventional program delivered by the CKD nurse-educators. The participants were engaged in three group-based sessions on the same day, with each session lasting about 60 min. Standardized content is presented by the trained CKD nurse-educators. The participants were invited to give their feedback on the program content and the performance of the nurse educators. They were asked about any improvement in their understanding of the self-management strategies of kidney disease and the ability to apply the strategies to self-manage their disease. Based on their feedback, changes were made in the intervention, such as modifications on the topics pertaining to the lifestyle (diet), medication, and timing to conduct a group-based session. After that, the CKD nurse-educators were trained again on the modified program content and materials before starting the group-based sessions.
Follow-up
The study duration is 12 weeks. After the baseline assessment (Week 0), there will be three group-based sessions on alternate weeks (Week 2, Week 4, and Week 6) as well as three individual follow-up phone calls on alternate weeks (Week 3, Week 5, and Week 7). Post-intervention assessment will be on the Week 6 post-group session or Week 5 after completion of the third follow-up phone call (Week 12 post-baseline meeting) (Figures 4 and 5).
CKD-NLSM support program trail timeline.
Participant program evaluation
The patients’ satisfaction with the CKD-NLSM support program will be evaluated at Week 12 during the T1 outcomes assessment (Figure 4) using a self-report evaluation form. We will investigate the extent to which the CKD-NLSM program helps people with CKD Stages 3–4 to understand their disease better and to formulate achievable goals. We will also look at whether the program content is useful and appropriate to the session; whether the length and schedule of the group-based sessions/follow-up phone calls are appropriate and convenient; whether the CKD nurse-educators are helpful; whether the CKD-Booklet is easy to read and understand; and also, whether the program is delivered in a culturally sensitive and understandable context. At the end of the evaluation form, patients will be asked to evaluate the program and give feedback on various aspects of the program.
Outcome measures
We hypothesize that, compared to standard usual care, the CKD-NLSM support program will significantly improve behavioral and clinical outcomes as well as increase the kidney disease knowledge (measured with KiKS), self-efficacy (SEMCD) and Self-Management (CKD-SM) in people with CKD Stages 3–4. Both groups will be assessed at two-time points: T0 (baseline) and T1 (Week 12).
Primary outcomes
The primary outcome is kidney disease knowledge as measured by the Malay-version KiKS. The co-primary outcome is CKD self-management that will be assessed using the Malay-version CKD-SM.
Secondary outcomes
The secondary outcomes are self-efficacy and HRQoL measured with the Malay-version SEMCD and KDQOL-36™, respectively. KDQOL-36™ is a self-administered questionnaire that assesses the HRQoL in the context of kidney disease. 52 This tool consists of 36 items under two sections, that is, the SF-12 that measures the generic QoL and the disease-specific core. The generic core has two domains with six items each that measure the physical component summary (PCS) and mental component summary (MCS). Meanwhile, the disease-specific core comprises 24 items with three domains, namely symptoms and problems (12 items), the burden of kidney disease (four items), and effects of kidney disease (eight items). However, two items on access (hemodialysis patients) and problems with the catheter (peritoneal dialysis patients) will be excluded as they do not apply to the participants of the present study. The scores will be transformed based on the scoring manual to a 0–100 range, whereby a higher score signifies better HRQoL.
Adherence to the CKD diet will be evaluated before and after the intervention through 24-h urinary protein, urea, creatinine, sodium, and potassium.
Other secondary outcomes
Blood Pressure (BP) control
BP will be assessed using the validated CARESCAPE V100 digital BP monitor that uses DINAMAP technology. BP measurement is taken after the participant sits and rests quietly for 5 min. Three BP measures will be taken on the right arm and the average of the three readings will be recorded. 55
Adherence to dietary protein
24-h urine protein is measured to quantify the daily urinary protein loss, a marker that indicates CKD prognosis. Protein restriction in people with CKD has led to reduced proteinuria by 20%–50%. 56 Patients who comply with dietary protein restriction will have lower urinary protein loss. Likewise, 24-h urine urea nitrogen (UUN) is also a biological marker used for the estimated protein intake (EPI). 57 EPI is calculated using the following formula: [(UUN (g/day) + (body weight (kg) × 0.031 g nitrogen/kg/day)] × 0.625. 58 The 24-h urinary creatinine is needed to ascertain the completeness of the 24-h urine collection. In a complete collection, the creatinine excretion should be approximately 20–25 and 15–20 mg/kg per day in men and women, respectively.59,60
Salt restriction
The 24-h urine sodium (Na) is a monitoring parameter of the sodium intake of people with advanced CKD. 57 Higher urinary sodium indicates higher dietary sodium intake. The ideal intake of sodium should be less than 100 mmol per day. 61 However, numerous studies reported that people with CKD commonly have urinary sodium excretions between 150 and 200 mmol that are above the recommended level. 61
Adherence to an alkaline diet
Diet can affect the acid–base balance in the body and this significantly influences the development and progression of CKD. Hence, the adherence to oral intake of alkali- or base-inducing fruits and vegetables will be evaluated using the Net Endogenous Acid Production (NEAP).62,63 NEAP will be estimated using a previously validated equation: NEAP (mEq/d) = −10.2 + 54.5 (protein intake [g/d] ÷ potassium intake [mEq/d]). 64
Ethics and endpoint
This study has been approved by the Medical Research Ethics Committee of the University Malaya Medical Centre (MREC ID NO: 201952-7389) and Universiti Putra Malaysia (JKEUPM-2019-374). Written informed consent will be obtained from all participants who agree to participate. All data will be kept confidential and used for research purposes only.
Statistical analyses
After data entry, the accuracy of the data will be determined by two researchers before data analysis. The principal investigator is responsible for managing, compiling, and maintaining the data that are saved and password-protected in the computer. Data analysis will follow both the protocol and the intention-to-treat approach. The normality and multicollinearity of the data will be determined. Data transformation is performed if required. Multiple imputations will be performed to address missing data. SPSS 25.0 (SPSS, Chicago, IL) will be used for data analysis and effect estimation.
Categorical variables in this study will be described as frequencies and percentages while continuous variables will be described as either means and standard deviations or medians and interquartile range. Baseline characteristics between the intervention and control groups will be compared using the chi-square test (qualitative variables), t-test or ANOVA (normally distributed quantitative variables), and nonparametric tests (non-normally distributed variables). Furthermore, the associations between baseline variables will be assessed using correlation analysis.
The primary outcomes in this study include CKD-specific knowledge and CKD self-management, both of which are continuous variables. To compare the changes in these measures, the Generalized Estimating Equations (GEE) procedure will be used. GEE is a robust method that can be used to test the effectiveness of the intervention by controlling for demographic variables such as age, gender, occupation, education level, and disease duration if there is any baseline imbalance in these variables. In this analysis, both between and within-group differences can be obtained. In the results section, the baseline values, final values, and the differences in the values in treatment and control groups the 95% confidence intervals and p-values will be reported. In addition, GEE will also be used to test the other outcome measures in this study, the SEMCD and KDQOL-36™. Similar analyses will be performed for BP control, patients’ adherence to CKD diet.
For GEE, the data will be entered in long-form, that is, each outcome variable will be entered as a single variable. Additionally, an extra variable, a “Time”, will be coded as 1 and 2, that indicates the baseline and the end of the study. The subject ID and their respective demographic characteristics will be repeated for Time 1 and Time 2 for both the control and treatment subjects. Under the repeated option in the analysis, Subject ID will be used as the subject variable and Time as the within-subject variable. For the covariance matrix, the robust estimator will be used. Scale response will be used in the type of model and the response will be the selected outcome variables. The significance of Time, Group effects, and the interaction effect of Time × Group will be tested. For all the tests, the level of significance will be set at 0.05.
Discussion
This RCT is well-positioned at the explanatory end of the pragmatic–explanatory spectrum to evaluate the effectiveness of the CKD-NLSM support program compared to the standard usual care in people with Stages 3–4 CKD. The participants’ knowledge of kidney disease, as well as self-efficacy and self-management behavior in managing CKD, will be assessed through translated and validated questionnaires. Additionally, domains such as HRQoL, adherence to disease-specific diet regime, and BP monitoring will also be a part of the study outcomes. More importantly, the study will demonstrate the feasibility of nurse-led CKD education programs in assisting people with CKD to achieve better self-efficacy, disease management, and improved QoL. To the best of our knowledge, this will be the first intervention study in Malaysia that integrate self-management, educational and psychosocial support using culturally relevant scenarios for people with CKD Stages 3–4, and measuring important self-reported and objective outcomes.
There are strengths and limitations to this study. First, successful randomization with concealed allocation will increase the between-group comparability. Secondly, the availability of the mobile phone contacts of the participants and their significant others facilitates the follow-up education with CKD nurse-educators and helps to reduce drop-outs. Furthermore, telephone follow-up is recognized as a useful strategy to reinforce education information and to encourage participants to change their health behaviors. There has been increasing evidence to indicate the important role of family encouragement and continuous support in the self-management of chronic diseases in terms of consuming healthful diets, taking medication, and undertaking physical activity. Treatment fidelity strategies are included to ensure that the intervention will be delivered as per protocol. The same training given to the CKD nurse-educators as outlined in the trainer’s written manual, standardized presentation slides are used for every training session, the nurse-educators will fill in log diaries and attendance lists, and the principal investigator will be present at all the sessions. Lastly, the study will apply validated Malay versions of KiKS, CKD-SM, and SEMCD to measure the study outcomes. We are aware of the risk of using not previously validated measures in the trial. The decision to include KiKS, CKD-SM, and SEMCD was taken after considering the importance of having CKD-specific outcome measures, beside the validated KDQOL-36™ and other objective outcome measures. The questionnaires in many different languages have been used and were found to be reliable and valid in patients with pre-dialysis CKD.
There are some potential limitations in the study. As the participants are from an urban tertiary hospital and required to understand the Malay language, this may lead to selection bias whereby the non-Malay-speaking Chinese, Indians, and other ethnic groups, and those who are literacy- and economically challenged would be under-represented. Given the nature of the intervention, it is not possible to blind the CKD nurse-educators and the participants. We acknowledge that this may contribute to response bias in the self-reported outcome measures. Also, social desirability bias may arise with self-reported instruments. However, with a number of objective physiological parameters included as study outcomes, we believe this will reduce the biases in the comparison of the outcomes between the two groups. Thirdly, due to time and budget constraints, the follow-up will only be up to 12 weeks. It can only produce short-term outcomes and no longer-term outcomes such as the progression to ESKD, CVDs and, behavioral change at longer term. However, we are confident of producing high-quality evidence at 12-week post-intervention, and this evidence is urgently needed for a self-management support program for people with non-dialysis dependent CKD in Malaysia. There is a high disease burden of CKD in the country, CKD-NLSM program could improve treatment adherence and QoL in people with non-dialysis CKD. 10 The study findings can be used to guide the program improvement and longer follow-up in the future such as involving participants from broader backgrounds, who are admitted to the inpatient wards or CKD patients in the community settings to evaluate the effectiveness of the self-management program in delaying CKD progression in different populations.
Conclusion
Self-management support programs have been reported to produce many positive outcomes in people with CKD. However, similar studies are few in low-to-middle-income countries. This parallel RCT is planned to evaluate the effectiveness of a theory-based, CKD-NLSM support program developed for people with CKD Stages 3–4 compared to standard usual care in Malaysia. Our study will contribute high-quality evidence on the effect of a CKD-NLSM program on the short-term kidney disease knowledge, self-efficacy, CKD self-management behavior, HRQoL, BP control, and adherence to CKD diet in people with non-dialysis dependent CKD.
Supplemental Material
sj-docx-1-sci-10.1177_00368504211026159 – Supplemental material for The effectiveness of nurse-led self-management support program for people with chronic kidney disease stage 3-4 (CKD-NLSM): Study protocol for a randomized controlled trial
Supplemental material, sj-docx-1-sci-10.1177_00368504211026159 for The effectiveness of nurse-led self-management support program for people with chronic kidney disease stage 3-4 (CKD-NLSM): Study protocol for a randomized controlled trial by Al Sawad Ayat Ali, Soo Kun Lim, Li Yoong Tang, Aneesa Abdul Rashid and Boon-How Chew in Science Progress
Footnotes
Acknowledgements
We would like to thank the management and patients at the University Malaya Medical Centre, for their support and cooperation during this study. We extend our gratitude to the CKD nurse-educators Miss. Karina Binti Abdul Wahid Pereira and Miss. Fatimah Hasanah Binti Mohd Radzi for their assistance in delivering CKD-NLSM support program. We express our sincere appreciation to The National Kidney Foundation of Malaysia (NKF), 70, Jalan 14/29, 46100 Petaling Jaya, Selangor Darul Ehsan, Malaysia for their collaboration in designing and printing the CKD booklet.
Author contributions
AAS drafted, formulated, and submitted the manuscript. All authors SKL, LYT, AAR & BHC contributed to the study designs, read, revised, and approved the research protocol critically for important intellectual content and helped to draft the final manuscript. All authors gave final approval of this manuscript to be published. Authorship eligibility is in accordance with the International Committee of Medical Journal Editors (ICMJE) guidelines.
Author’s Note
Boon-How Chew is also affiliated with Clinical Research Unit, Hospital Pengajar Universiti Putra Malaysia (HPUPM Teaching Hospital), Serdang, Malaysia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study has received funding/assistance from a commercial organization.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.