
Abstract
Objective
This study aimed to examine the association between the C-reactive protein-albumin-lymphocyte (CALLY) index and the hypertension prevalence in adults with diabetes.
Methods
This cross-sectional study was conducted using data from the National Health and Nutrition Examination Survey (NHANES) (1999–2010). Adult participants diagnosed with diabetes were included. The CALLY index was calculated based on C-reactive protein (CRP), albumin (ALB), and lymphocyte count (LC) and divided into two groups. Univariate and multivariate logistic regression models were used to evaluate the association between the CALLY index and hypertension prevalence, adjusting for confounders such as age, sex, race, poverty-income ratio (PIR), smoking, and alcohol consumption. Restricted cubic spline (RCS) analysis was performed to explore potential nonlinear relationships.
Results
A total of 4163 diabetic adults were included. A significant inverse association was observed between the CALLY index and hypertension prevalence. In multivariate analysis, after adjusting for confounders, participants in the upper quantile (M2) exhibited a lower hypertension prevalence compared to those in the lower quantile (M1) (odds ratio (OR) = 0.82, 95% confidence interval (CI): 0.71–0.94, p = 0.004). RCS analysis indicated a nonlinear association, with a protective effect of the CALLY index against hypertension.
Conclusion
The CALLY index is associated with hypertension prevalence in diabetic adults, integrating inflammatory, immune, and nutritional parameters. CALLY may serve as a potential biomarker for risk stratification; however, causality cannot be inferred due to the cross-sectional study design.
Introduction
Hypertension and diabetes are two prevalent chronic diseases worldwide, with an increasing burden of comorbidity, particularly among adults. 1 Both conditions are leading contributors to premature mortality and disease burden. 2 The coexistence of hypertension and diabetes significantly increases the odds of cardiovascular disease, kidney disease, and other chronic complications.3,4 Therefore, identifying diabetic patients with higher prevalence of hypertension and implementing effective interventions has become a critical issue in clinical and public health research.
Diabetes, particularly type 2 diabetes mellitus (T2DM), is often accompanied by metabolic disorders, chronic low-grade inflammation, and immune dysfunction. These pathological processes not only influence the progression of diabetes but also contribute to the presence of hypertension.5,6 The interplay between hypertension and diabetes involves multiple mechanisms, including oxidative stress, endothelial dysfunction, and insulin resistance. This interaction exacerbates vascular damage and arteriosclerosis in hypertensive patients, further aggravating metabolic stress in diabetic individuals and creating a vicious cycle of complications.7–9 The C-reactive protein-albumin-lymphocyte (CALLY) index has been validated in several clinical contexts, particularly in oncological settings where it demonstrated prognostic value for survival outcomes. Previous studies have shown that CALLY effectively integrates inflammatory burden (C-reactive protein, CRP), nutritional status (albumin), and immune function (lymphocyte count) into a single composite score. However, its application in diabetic populations and relationship with hypertension remains largely unexplored.
Recently, biomarkers related to inflammation, immunity, and nutrition, such as CRP, albumin (ALB), and lymphocyte count (LC), have been increasingly recognized for their critical roles in cardiovascular and metabolic diseases. 10 Inflammation is a hallmark of diabetes and has also been implicated in the pathogenesis of hypertension.11,12 CRP serves as a global marker of systemic inflammation, ALB reflects nutritional status and metabolic health, while LC indicates immune system activity. 13 As a composite index integrating these three markers, the CALLY index offers a more comprehensive assessment of overall health status and has the potential to predict hypertension prevalence in diabetic patients. By evaluating the inflammatory, immune, and nutritional states of diabetic patients, CALLY may serve as a more integrated and predictive biomarker.
This study aims to investigate the association between the CALLY index and the hypertension prevalence in adult patients with diabetes. By comprehensively assessing inflammation, nutrition, and immune status, we seek to determine whether the CALLY index can serve as a predictive tool for hypertension prevalence. Our findings may provide novel insights into hypertension screening in diabetic patients and contribute to improved clinical management and intervention strategies.
Methods
Study design and data source
This cross-sectional study utilized data from the National Health and Nutrition Examination Survey (NHANES) from 1999 to 2010. NHANES, conducted by the Centers for Disease Control and Prevention (CDC), is a nationally representative health survey designed to collect information on the health, nutrition, and disease status of the US population. 14 The survey employs a stratified, multistage sampling design to ensure representativeness, providing high-quality data for public health research. For this study, we included participants meeting the following criteria: (1) aged ≥18 years, (2) diagnosed with diabetes, and (3) with complete CRP, ALB, and LC data. Exclusion criteria were: (1) individuals without a diabetes diagnosis, (2) those lacking hypertension data, and (3) participants missing CRP, ALB, or LC measurements. After applying these criteria, a total of 4163 participants were included in the final analysis. Figure 1 illustrates the detailed flowchart of participant selection. This study was conducted in accordance with the Helsinki Declaration of 1975 as revised in 2024. 15 The reporting of this study conforms to STROBE guidelines for cross-sectional studies. 16

Flowchart of participant inclusion and exclusion.
Definition of the CALLY index
In NHANES, all biological samples were processed under standardized laboratory conditions. The CALLY index was calculated using CRP, ALB, and LC levels as an integrated biomarker of inflammation, nutritional, and immune status. The CALLY index was considered the primary exposure variable in this study and was calculated using the following formula:CALLY index = [albumin (g/dL) × lymphocyte count (/μl)]/[CRP (mg/dL) × 104]. 13 By combining these three indicators, the CALLY index provides a comprehensive assessment of systemic inflammation, immune function, and nutritional status, making it a potentially valuable predictor of hypertension prevalence in diabetic patients.
Definition of diabetes and hypertension
Diabetes was defined based on the following criteria: (1) random blood glucose level ≥11.1 mmol/L, (2) fasting blood glucose level ≥7.0 mmol/L, and (3) self-reported physician diagnosis of diabetes. This analysis included participants with diabetes regardless of type (type 1 or type 2 diabetes mellitus). Hypertension was diagnosed if: (1) systolic blood pressure (SBP) ≥ 140 mmHg or diastolic blood pressure (DBP) ≥ 90 mmHg, (2) self-reported physician diagnosis of hypertension. This cross-sectional analysis examined the prevalence of hypertension at baseline among diabetic participants. We did not analyze incident (new-onset) hypertension during follow up, as NHANES provides cross-sectional data at single time points.
Selection and adjustment of covariates
To ensure the robustness of our analysis, we selected covariates that could potentially influence hypertension prevalence. These covariates included sex, age, race, education level, smoking status, alcohol consumption, poverty-income ratio (PIR), white blood cell count (WBC), and platelet count (PLT). Previous studies have extensively investigated the complex interactions of these factors and their varying degrees of influence on hypertension prevalence.17–21 Age and sex are well-established associated factors for hypertension, while PIR reflects socioeconomic status, which may indirectly affect overall health. Since these covariates could confound the association between the CALLY index and hypertension prevalence, they were carefully controlled in the statistical analysis.
Statistical analysis
All statistical analyses were performed using R software (version 4.0.3). First, descriptive statistical analyses were conducted to summarize the means, standard deviations, and frequency distributions of all variables. Differences between hypertensive and nonhypertensive groups were compared using the chi-square test for categorical variables and the unpaired t-test for continuous variables, as appropriate. Multivariate logistic regression models were then used to evaluate the association between the CALLY index and hypertension prevalence. In these models, hypertension (presence or absence) was treated as a binary dependent variable, while the CALLY index was included as either a continuous or categorical exposure variable. To avoid reduced statistical power due to excessive stratification, CALLY was divided into two quantiles: the lower quantile (M1) and the upper quantile (M2), with the cutoff value determined by the median CALLY index in the study population. Four logistic regression models were constructed: model 1—no adjustments. Model 2–adjusted for age, sex, education level, and PIR. Model 3—further adjusted for race, smoking, and alcohol consumption. Model 4—additionally adjusted for WBC and PLT levels. To explore potential nonlinear associations between the exposure and outcome variables, smoothing spline fitting and threshold effect analysis were applied. Stratified analyses were also conducted to assess whether the relationship between the CALLY index and hypertension prevalence varied across different subgroups. Statistical significance was set at p < 0.05. Interaction analyses were performed to assess whether the association varied by sex and age subgroups.
Results
Baseline characteristics of the study population
A total of 4163 participants were included in this study, of whom 2176 were male and 1987 were female. Among all participants, 2666 (64.0%) had hypertension, while 1497 (36.0%) did not. As shown in Table 1, significant differences were also observed in sex, age, race, and PIR across different CALLY quantiles (p < 0.05 for all).
Baseline characteristics of the study population stratified by CALLY index quantiles (M1 and M2).
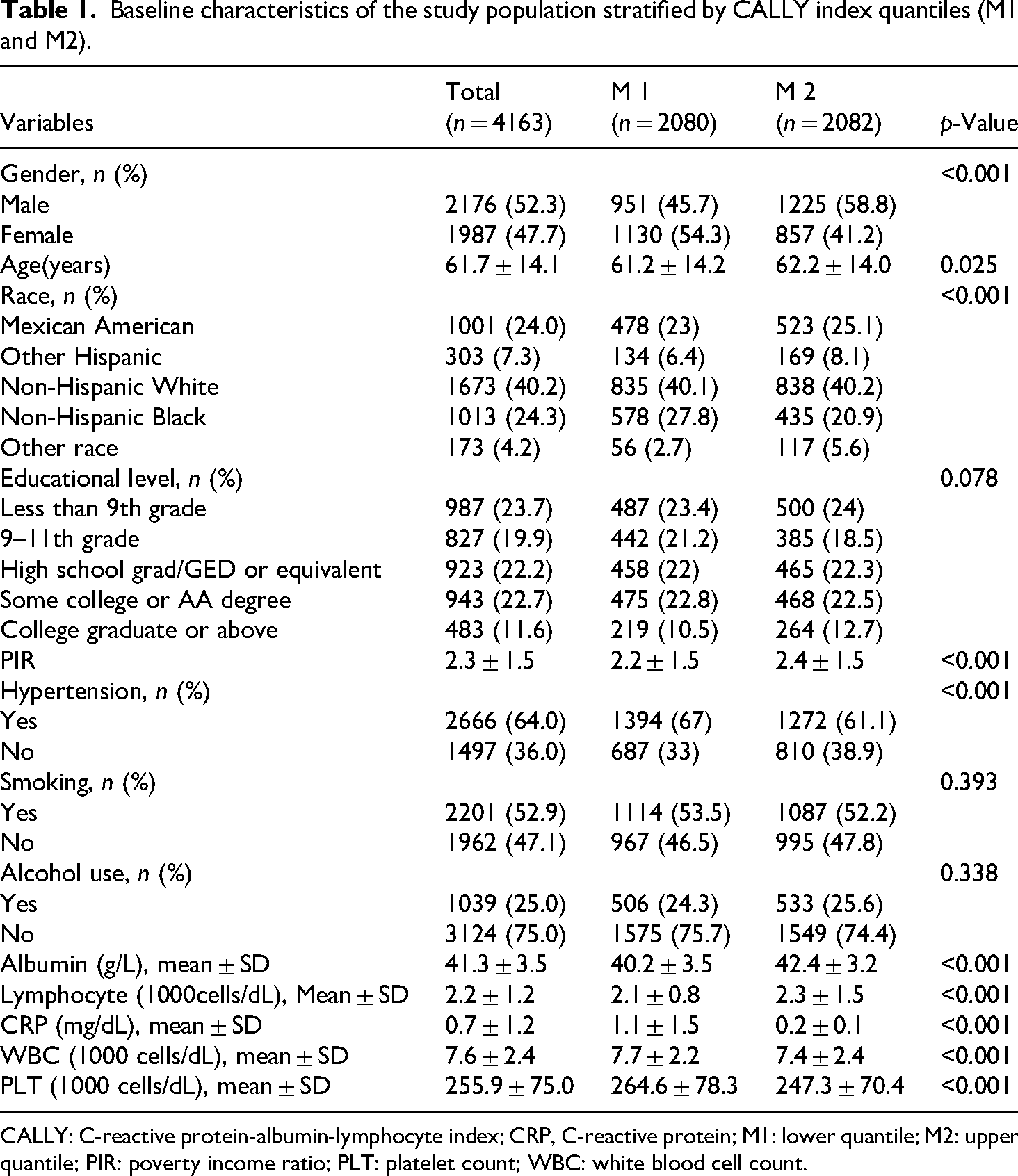
CALLY: C-reactive protein-albumin-lymphocyte index; CRP, C-reactive protein; M1: lower quantile; M2: upper quantile; PIR: poverty income ratio; PLT: platelet count; WBC: white blood cell count.
Association between CALLY and hypertension
Our findings indicate that a higher CALLY index is associated with a lower prevalence of hypertension in adults with diabetes. In the logistic regression models where hypertension was the dependent variable, the CALLY index showed a significant inverse association with hypertension prevalence (Table 2). In the unadjusted model, compared to participants in the M1, those in the M2 had a 23% lower hypertension prevalence (OR = 0.77, 95% CI: 0.68–0.88). After adjusting for all covariates, this association remained significant (OR = 0.82, 95% CI: 0.71–0.94). These results suggest that the CALLY index, as an integrated biomarker, correlates significantly with the hypertension prevalence among patients with diabetes. Elevated CALLY levels corresponded to reduced hypertension prevalence in diabetic patients, independent of confounding variables. However, while statistically significant, further research is required to validate its clinical utility, particularly across different subpopulations.
Association between C-reactive protein-albumin-lymphocyte index and hypertension prevalence in diabetic adults.

Model 1, crude model.
Model 2, adjusted for gender, age, educational level, PIR.
Model 3, adjusted for gender, age, educational level, PIR, race, BMI, hypertension, smoking, alcohol use.
Model 4, adjusted for gender, age, educational level, PIR, race, BMI, hypertension, smoking, alcohol use, WBC and PLT.
BMI: body mass index; CALLY: C-reactive protein-albumin-lymphocyte index; CI: confidence interval; OR: odd ratio; PIR: poverty income ratio; PLT: platelet count WBC: white blood cell count.
Restricted cubic spline (RCS) analysis
After adjusting for all covariates, RCS analysis was conducted to explore the potential nonlinear relationship between the CALLY index and hypertension prevalence in diabetic adults (Figure 2). The results revealed a nonlinear association, where the hypertension prevalence decreased with increasing CALLY levels initially, followed by a plateau at higher CALLY levels where the association was no longer statistically significant.
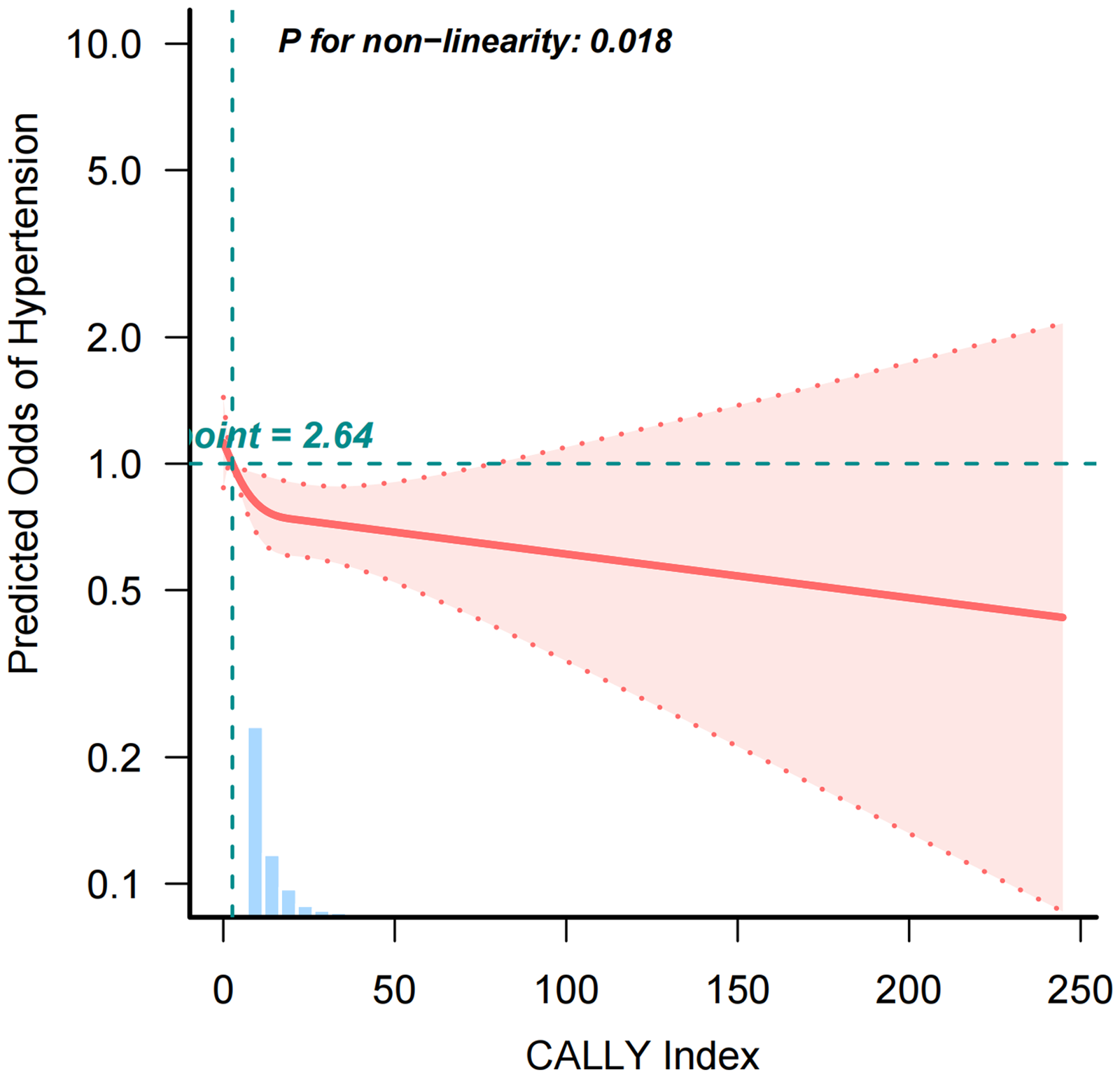
Restricted cubic spline curve illustrating the relationship between CALLY and hypertension prevalence in diabetic adults. CALLY: C-reactive protein-albumin-lymphocyte index.
Subgroup analyses
To further investigate whether the association between the CALLY index and hypertension prevalence differed across subgroups, we performed stratified analyses based on sex and age. Sex-stratified analysis: the association was more pronounced in males (OR = 0.65, 95% CI: 0.55–0.78, p < 0.001), whereas no significant association was observed in females (OR = 1.05, 95% CI: 0.87–1.27, p = 0.626). This suggests that male diabetic patients with lower CALLY levels are at a higher prevalence of hypertension. Age-stratified analysis: the inverse association between CALLY and hypertension was stronger in participants younger than 60 years (OR = 0.62, 95% CI: 0.51–0.76, p < 0.001), whereas the association was weaker and of marginal significance in participants aged 60 years and older (OR = 0.84, 95% CI: 0.71–0.99, p = 0.042) (Table 3). Interaction analyses confirmed the observed subgroup differences: sex interaction p < 0.001, age interaction p = 0.027, indicating that the protective effect of CALLY was more pronounced in male and younger patients. This suggests that the protective effect of the CALLY index is more evident in younger diabetic adults, possibly due to age-related physiological changes and chronic disease progression.
Subgroup analysis of CALLY and hypertension prevalence in diabetic adults.

CI: confidence interval; OR: odd ratio.
Discussion
Hypertension is highly prevalent among individuals with diabetes, with studies indicating that more than 50% of hypertensive patients are also diagnosed with type 2 diabetes mellitus (T2DM). 22 The presence of hypertension significantly exacerbates cardiovascular odds in diabetic patients, increasing the incidence of complications such as diabetic retinopathy and nephropathy. Given the frequent coexistence of hypertension and diabetes, these conditions collectively elevate the odds of cardiovascular events and mortality.23,24 Notably, uncontrolled hypertension among diabetic patients further complicates disease management and worsens clinical outcomes. This study is the first to examine the relationship between the CALLY index and hypertension prevalence in diabetic patients. By analyzing this composite index, which integrates inflammation (CRP), nutritional status (ALB), and immune function (LC), we identified a significant inverse association between CALLY levels and hypertension prevalence. Our findings suggest that diabetic patients with higher CALLY levels have a lower prevalence of hypertension.
Inflammation is a key pathological process in chronic metabolic diseases such as hypertension and diabetes.25,26 Recent studies suggest that inflammation not only plays a crucial role in hypertension pathogenesis but also contributes to increased cardiovascular risk in diabetic patients. 27 Elevated levels of inflammatory markers, particularly CRP, have been widely associated with the onset and progression of hypertension.28–30CRP, an acute-phase protein synthesized by the liver, rises in response to bacterial infections, tissue injury, or chronic inflammation. It promotes endothelial inflammation, enhances local oxidative stress, and facilitates immune cell infiltration into vascular walls, all of which contribute to presence of hypertension.31–33
In diabetic patients, chronic low-grade inflammation further increases the hypertension prevalence. Hyperglycemia itself induces a persistent inflammatory state by promoting oxidative stress, altering endothelial function, and impairing nitric oxide bioavailability, thereby facilitating hypertension progression. Elevated CRP levels in diabetic patients not only indicate chronic inflammation but also reflect endothelial dysfunction.34,35 This dysfunction is particularly severe in diabetes due to prolonged hyperglycemia, which leads to endothelial cell damage and apoptosis, further accelerating vascular stiffening and hypertension. 36 Additionally, CRP exacerbates vascular structural changes by promoting immune cell infiltration and vascular smooth muscle proliferation.37,38 Therefore, CRP elevation can serve as a significant marker of higher hypertension prevalence in diabetic patients.
ALB, the predominant plasma protein, plays a crucial role in maintaining osmotic pressure, transporting nutrients, exhibiting antioxidant properties, and regulating immune responses.39,40 In diabetic patients, ALB levels are often altered, especially in those with chronic complications such as diabetic nephropathy, where hypoalbuminemia is common. Hypoalbuminemia frequently occurs in chronic diseases and malnutrition, particularly in diabetes when renal function is impaired. The onset of diabetic nephropathy is often accompanied by proteinuria, leading to reduced plasma albumin levels.41,42 Hypoalbuminemia not only reflects nutritional deficiencies but is also closely linked to metabolic disturbances and increased cardiovascular odds. A decline in ALB may cause sodium and water retention, leading to increased blood volume and subsequent hypertension.43,44 Moreover, reduced ALB levels are associated with endothelial dysfunction, heightened inflammation, and immune dysregulation, all of which are potential mechanisms underlying presence of hypertension.45,46
LC are essential components of the immune system, regulating immune and inflammatory responses. Emerging research suggests a potential association between lymphocyte count and hypertension. 47 Excessive immune activation, particularly lymphocyte proliferation, may contribute to endothelial dysfunction and vascular remodeling, leading to elevated blood pressure. 48 In diabetic patients, immune system dysfunction is frequently observed.49,50 Chronic hyperglycemia not only induces oxidative stress and alters endothelial function but also activates immune cells, particularly lymphocytes, exacerbating hypertension prevalence. Lymphocytes play a critical role in the immune-inflammatory response in diabetes, and their levels and activity are closely linked to vascular health.12,51 Studies indicate that individuals with lower lymphocyte counts tend to exhibit immune dysfunction, which may impair vascular repair and endothelial regeneration, thereby increasing hypertension prevalence. 52
As independent biomarkers, CRP, ALB, and LC each reflect different aspects of inflammation, nutrition, and immune status. However, using these markers individually for hypertension prevalence prediction has limitations. A combined approach incorporating these indicators provides a more comprehensive assessment of an individual's overall health. 53 The CALLY index integrates multiple physiological processes, offering a more precise tool for predicting hypertension prevalence in diabetic patients. Research has demonstrated strong associations between dysregulated inflammatory responses, nutritional status, and immune function with hypertension prevalence.54,55 As a composite biomarker, the CALLY index effectively reflects these imbalances. Our study found that higher CALLY levels were significantly associated with a lower hypertension prevalence in diabetic patients, even after adjusting for potential confounders such as age and sex. This finding has important clinical implications, as measuring CALLY could enable clinicians to more accurately assess hypertension prevalence in diabetic patients, particularly those with inflammatory, nutritional, or immune dysfunction. This provides a novel biomarker for early hypertension screening and intervention in diabetic populations.
Our study further revealed that CALLY, as a potential composite biomarker, showed a relationship with lower hypertension prevalence in male diabetic patients, whereas no such association was observed in females. This sex-based difference may be attributed to multiple factors.56–58 First, hormonal differences might play a crucial role. 59 Estrogen exerts cardiovascular protective effects in premenopausal women, which may attenuate the predictive value of systemic inflammation markers like CALLY. In males, the absence of such hormonal buffering may make CALLY a more sensitive indicator of cardiovascular risk.57,60 Second, differences in body composition, particularly in fat distribution, may influence the effect of CALLY on hypertension. 61 Males typically have higher visceral fat accumulation, while females tend to store more subcutaneous fat, potentially leading to sex-specific differences in the association between CALLY and hypertension prevalence.60,62 Moreover, age was also a modulating factor in this relationship. A significant inverse association between CALLY and hypertension was observed in younger patients, but this association weakened in older individuals. This attenuation might be attributed to age-related physiological changes and the increasing burden of chronic diseases. 63 Age-related differences may be linked to the vascular aging process.64,65 With aging, structural and functional changes in the vasculature, such as increased arterial stiffness, contribute to hypertension. The protective effects of CALLY may diminish in older patients due to these vascular changes. Additionally, older individuals are more likely to have multiple comorbidities, such as chronic kidney disease or heart failure, which could confound or modify the relationship between CALLY and hypertension.66,67 Future research should further investigate the mechanisms underlying the role of CALLY across different sex and age groups and explore its potential clinical utility as a preventive and interventional target. The observed sex and age interactions suggest differential effects of CALLY across demographic subgroups, though validation in independent cohorts is needed before clinical application.
Despite the important findings, this study has several limitations. Cross-sectional design: the study design prevents the establishment of causal relationships. Future prospective cohort studies are required to validate the predictive role of CALLY in hypertension prevalence. Generalizability: while CALLY demonstrated good predictive performance, its applicability requires further validation in larger and more diverse diabetic populations, particularly considering variations across different regions and disease stages. Potential reporting bias: some data, including hypertension and diabetes diagnoses, relied on self-reported information, which may introduce bias and misclassification errors. Sample heterogeneity: variability in participant characteristics may influence the generalizability of our findings. Therefore, future research should conduct larger-scale and longitudinal studies to further validate the utility of CALLY in different populations. Additionally, because the study uses cross-sectional data, temporal sequencing between CALLY levels and hypertension prevalence cannot be established. Consequently, longitudinal studies are required to validate causal pathways. Furthermore, several variables were not available in the NHANES dataset for the study period, including body mass index (BMI), glycated haemoglobin (HbA1c) levels, comprehensive lipid profiles, antihypertensive medication use, statin therapy, and diabetes duration. These factors could potentially confound the relationship between CALLY and hypertension and should be considered in future studies. Finally, diabetes type differentiation and insulin treatment analysis were not performed in this study. These variables may modify the association between CALLY and hypertension and warrant investigation in future research.
This study provides a novel perspective on hypertension prevalence assessment in diabetic patients. As a simple and cost-effective biomarker combination, CALLY may help clinicians identify diabetic patients with hypertension, particularly in high-prevalence subgroups. Future research should further explore its role in screening, prevention, and clinical management of hypertension in diabetes. CRP, ALB, and LC have been widely used as independent biomarkers in clinical practice, particularly for assessing inflammation, immune function, and nutritional status. However, using these markers individually has limitations, as each reflects only one aspect of systemic health. The CALLY index, which integrates CRP, ALB, and LC, offers a comprehensive evaluation of inflammation, nutrition, and immune function. Elevated CALLY levels often indicate increased inflammation, poor nutritional status, or immune dysfunction. In cardiovascular and metabolic diseases, CALLY has demonstrated strong clinical value as an integrated biomarker. In the context of diabetes and hypertension, CALLY may serve as an indicator of inflammation and immune dysregulation, revealing potential mechanisms underlying presence of hypertension in diabetic patients. Thus, CALLY represents a promising predictive tool for hypertension prevalence assessment in diabetic patients, with important clinical implications for early screening and intervention.
Conclusion
This study demonstrates that CALLY demonstrates a notable relationship with hypertension prevalence in diabetic patients, particularly in males and younger individuals, highlighting its potential clinical value. As an integrated biomarker encompassing inflammation, nutrition, and immune status, CALLY may serve as an effective tool for early odds identification and intervention in diabetic patients at odds for hypertension. Future research should further explore CALLY's predictive mechanisms, optimization strategies, and broader applicability, providing new insights and tools for precision management of hypertension in diabetes.
Footnotes
Ethics approval and consent to participate
Authors’ contributions
FW was involved in conceptualization; FW and JP in data curation and project administration; FW and ZC in formal analysis; JP and ZC in investigation; FW and JX in funding acquisition, methodology; ZC and CX in resources; JP and CX in software; JP and HH in supervision and validation; JP and JX in visualization; JP and FW in writing-original draft; and JP, JX, ZC, CX, HH, and FW in writing-review & editing.
Funding
The authors acknowledge financial support for the research, authorship, and publication of this article. We sincerely thank the Hubei Provincial Administration of Traditional Chinese Medicine (grant no. ZY2023Q028), the Enshi Prefecture Science and Technology Program (grant no. D20230078), the Central Hospital of Enshi Tujia and Miao Autonomous Prefecture (grant no. 2023ZDSYS11), and the 2024 Enshi Prefecture “Sailing Special” Science and Technology Project.
Declaration of conflicting interests
The authors declare that no commercial or financial relationships exist that could be construed as a potential conflict of interest in relation to this study.