
Abstract
Objective
This study aimed to evaluate the associations between body mass index (BMI), dietary nutrient intake, and the risk of branch retinal vein occlusion (BRVO) in a nationally representative Korean population, with a focus on sex- and BMI-specific differences.
Methods
This population-based cross-sectional study analyzed data from adults aged ≥40 years who participated in the 7th and 8th Korea National Health and Nutrition Examination Surveys (KNHANES) conducted between 2017 and 2021. BRVO was diagnosed using standardized fundus photography and optical coherence tomography interpreted by certified retinal specialists. BMI was categorized according to Asia–Pacific criteria, and dietary intake of macronutrients and micronutrients was assessed using structured nutrition surveys. Comparisons were performed between participants with and without BRVO, stratified by sex and BMI category. Survey-weighted logistic regression models were applied to account for the complex sampling design and to adjust for age, smoking status, alcohol consumption, hypertension, diabetes mellitus, and BMI.
Results
A total of 15,790 participants (6,629 men and 9,161 women) were included, of whom 96 (43 men and 53 women) were diagnosed with BRVO. Participants with BRVO were significantly older and had a higher prevalence of hypertension (all P < 0.001). Overall, individuals with BRVO showed significantly lower intakes of protein, crude fiber, iron, sodium, and potassium (all P < 0.05). Although overall BRVO prevalence did not differ significantly across BMI categories, sex-stratified analyses revealed an increasing prevalence with higher BMI in women. Associations between dietary nutrient intake and BRVO varied across BMI strata.
Conclusions
Lower nutrient intake and metabolic risk factors, including hypertension and BMI, may be associated with BRVO risk. The observed sex- and BMI-specific differences highlight the importance of tailored nutritional and metabolic risk assessment. Longitudinal studies are warranted to clarify causal relationships.
Introduction
Retinal vein occlusion (RVO), encompassing both central (CRVO) and branch (BRVO) subtypes, is the second most common retinal vascular disorder after diabetic retinopathy.1,2 More than half of patients with RVO regain functional visual acuity sufficient for daily activities when they receive appropriate treatment.3,4 RVO occurs more frequently in retinal veins than arteries and often carries a relatively favorable prognosis. 5 Recent global epidemiologic data indicate that RVO is a relatively common retinal vascular disorder, with an overall pooled prevalence of approximately 0.8% in the adult population, and branch retinal vein occlusion accounting for the majority of cases. 6 This considerable worldwide burden highlights the need to better understand modifiable metabolic and lifestyle-related risk factors for RVO. In the Korean population aged ≥19 years, the prevalence of RVO was reported to be 0.6% (standard error 0.1%) between 2008 and 2012, and the incidence of clinically diagnosed RVO was approximately 48 per 100,000 person-years. 7
Advancing age is a major risk factor for RVO. 8 Previous studies have reported that certain cardiovascular and systemic conditions, particularly hypertension, are associated with RVO, whereas the associations with other factors such as smoking or generalized atherosclerotic changes have been inconsistent across populations and analyses.9–12 Metabolic syndrome, defined by elevated blood pressure, hyperglycemia, dyslipidemia, and central obesity, has been shown to increase the risk of RVO among smokers compared with non-smokers. 13 Furthermore, recent large population-based cohort studies have reported that patients with RVO have an increased risk of cardiovascular morbidity and all-cause mortality, suggesting that RVO may be a marker of systemic vascular disease.14,15
Dietary patterns and specific nutrient intake are increasingly recognized as modifiable determinants of cardiovascular health. Diets rich in fish, fruits, vegetables, whole grains, and nuts, as well as nutrients such as omega-3 fatty acids, antioxidant vitamins (A, C, D), and folic acid, may improve vascular health and potentially reduce the risk of RVO. 16 However, no Korean study has investigated the associations of systemic conditions, body mass index (BMI), and nutrient intake with BRVO.
This study aimed to evaluate the associations between BMI, dietary nutrient intake, and the risk of BRVO in a nationally representative Korean population using a recently released dataset from the Korean National Health and Nutrition Examination Survey (KNHANES) conducted between 2017 and 2021.
Methods
This study was based on data obtained from the 7th and 8th Korea National Health and Nutrition Examination Survey (KNHANES), a nationwide, population-based program administered by the Ministry of Health and Welfare of Korea. All KNHANES participants had provided written informed consent, and the survey protocol complied with the Declaration of Helsinki of 1975 as revised in 2024. The present analysis of anonymized public data was additionally approved by the Institutional Review Board of Kangbuk Samsung Hospital, Seoul, Republic of Korea on August 23rd, 2024 (IRB No. 2024-08-022). This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 17
Study population
This population-based cross-sectional study analyzed data from adults aged ≥ 40 years who participated in the 7th (2016–2018) and 8th (2019–2021) KNHANES. Each survey cycle consisted of three components: a health interview, a nutrition survey, and a health examination. KNHANES is a nationwide survey conducted by the Korea Disease Control and Prevention Agency (KDCA) using a multistage, stratified cluster sampling design based on the National Census Registry. A rolling sampling method was employed to ensure comparability across survey years and maintain national representativeness. 18 The quality of ophthalmologic data was validated by the Epidemiological Survey Committee of the Korean Ophthalmological Society. Sampling weights were applied to account for the complex survey design, non-response, and post-stratification, 19 enabling estimation of population-level parameters for the Korean adult population. 20 The detailed methodology of KNHANES has been described previously. 21
The number of CRVO cases in the KNHANES dataset was very small (1 case in 2017, 2 in 2018, 1 in 2019, 3 in 2020, and none in 2021). Therefore, CRVO was not included in the analysis to avoid unstable estimates and potential bias.
Data collection and outcomes
Demographic and clinical variables were collected through structured health interviews and physical examinations, which included blood pressure measurements, anthropometric assessments, laboratory tests, and ophthalmologic evaluations. Ophthalmic examinations were conducted as part of the physical assessment, during which 45° non-mydriatic color fundus photographs were obtained using a fundus camera (TRC-NW6S; Topcon, Tokyo, Japan), and optical coherence tomography (OCT) was performed using the CIRRUS HD-OCT 500 device (Carl Zeiss Meditec, Dublin, CA, USA).
Branch retinal vein occlusion (BRVO) was diagnosed based on characteristic sectoral retinal hemorrhages with associated venous dilatation or tortuosity confined to the distribution of a branch retinal vein on fundus photographs acquired with the Visucam 224 (Carl Zeiss Meditec AG, Germany) and interpreted by board-certified retinal specialists designated by the Korean Retina Society. Each image was independently evaluated by two graders, and in cases of disagreement, final adjudication was made by a senior review committee within the Korean Retina Society. 21
Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared (kg/m2), and categorized into four groups: underweight (<18.5 kg/m2), normal weight (18.5–22.9 kg/m2), overweight (23.0–24.9 kg/m2), and obese (≥25.0 kg/m2).
Dietary intake was assessed using detailed food frequency questionnaires administered during health interviews. The analyzed nutrients included total food intake, energy, macronutrients (protein, fat, carbohydrate), and crude fiber, as well as a range of micronutrients, such as calcium, phosphorus, iron, sodium, potassium, and vitamins. Specifically, vitamin intake components included vitamin A, β-carotene, retinol, thiamin, riboflavin, niacin, and vitamin C. Nutrient intake levels and BMI categories were compared between participants with and without RVO, stratified by sex.
Hypertension was defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg or current use of antihypertensive medication. Diabetes mellitus was defined as a fasting plasma glucose level ≥126 mg/dL, glycated hemoglobin (HbA1c) level ≥6.5%, self-reported physician diagnosis, or current use of antidiabetic medication.
Statistical analysis
Continuous variables are presented as means with standard deviations (SD), and categorical variables are presented as numbers and percentages. Group comparisons were performed using the svyttest and svychisq functions from the survey package in R for continuous and categorical variables, respectively. The associations between nutritional intake and BRVO were evaluated using survey-weighted logistic regression models implemented through the svyglm function in R. Both univariate and multivariate analyses were performed. The multivariate models were adjusted for potential confounders including age, smoking status (current/past vs never), alcohol consumption (current vs never), BMI, presence of hypertension, and diabetes mellitus. Results are presented as odds ratios (ORs) with 95% CIs. For subgroup analyses stratified by BMI categories, separate logistic regression models were fitted for each BMI group. The BMI categories were defined as underweight (<18.5 kg/m2), normal weight (18.5-22.9 kg/m2), overweight (23.0-24.9 kg/m2), and obese (≥25.0 kg/m2) according to the Asian-Pacific criteria.
The complex sampling design of KNHANES was incorporated into all statistical analyses using the ‘survey’ package in R. Survey weights were applied to obtain nationally representative estimates. All statistical analyses were performed using R software version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria), and all statistical tests were two-sided with p-values less than 0.05 considered statistically significant.
This study is a secondary analysis of the KNHANES 2017–2021 data, which is a nationwide survey conducted by the Korea Disease Control and Prevention Agency (KDCA). Therefore, the sample size was not determined by a prospective power calculation but was defined by the number of eligible participants available in the dataset. Specifically, out of the total 38,678 participants in the survey period, we included all 15,790 individuals who met our inclusion criteria (age ≥ 40 years with complete ophthalmologic and nutritional data) to maximize statistical power and precision. As this is one of the largest population-based studies on BRVO to date, the sample size provides sufficient statistical power to detect meaningful associations, as reflected in the narrow confidence intervals of our estimates. An item non-responder analysis was performed by comparing baseline characteristics between included and excluded participants using standardized mean differences (SMDs). To improve model stability and reduce the potential impact of sparse data in certain BMI subgroups, additional sensitivity analyses were conducted by collapsing BMI categories into three broader groups (<23, 23–24.9, and ≥25 kg/m2). Continuous nutritional variables were standardized and analyzed per 1–standard deviation (1-SD) increment. Potential non-linear associations between dietary intake and BRVO risk were further evaluated using restricted cubic spline models.
Results
From 2017 to 2021, 38,678 individuals participated in Korea National Health and Nutrition Examination Survey (KNHANES). Among them, 15,790 participants (6,629 men and 9,161 women) were included in the final analysis (Figure 1). Of these, 96 individuals were diagnosed with branch retinal vein occlusion, including 43 men and 53 women. Flowchart of participant selection and inclusion in the Korea national health and nutrition examination survey (KNHNES) between 2017 and 2021.
Demographics of study participants.

Abbreviations: BP: Blood Pressure; BRVO: branch retinal vein occlusion; HDL-C: high-density lipoprotein cholesterol; RVO: retinal vein occlusion.
Dietary intake of study participants with and without retinal vein occlusion (RVO).

P values resulting from general linear model for continuous variables.
Abbreviations: BRVO: branch retinal vein occlusion; RVO: retinal vein occlusion; SE: standard error.
aAdjusted for age.
Compared with included participants, excluded individuals were substantially younger and had lower metabolic parameters, including BMI and waist circumference, whereas differences in other variables such as sex, diabetes, and hypertension were minimal (Supplemental Table S1).
The prevalence of BRVO according to BMI.

P values resulting from general linear model.
Abbreviations: BMI: body mass index; BRVO: branch retinal vein occlusion; CI: confidence interval.
Difference of dietary intake between BRVO and non-RVO groups in men.

Difference of dietary intake between BRVO and non-RVO groups in women.
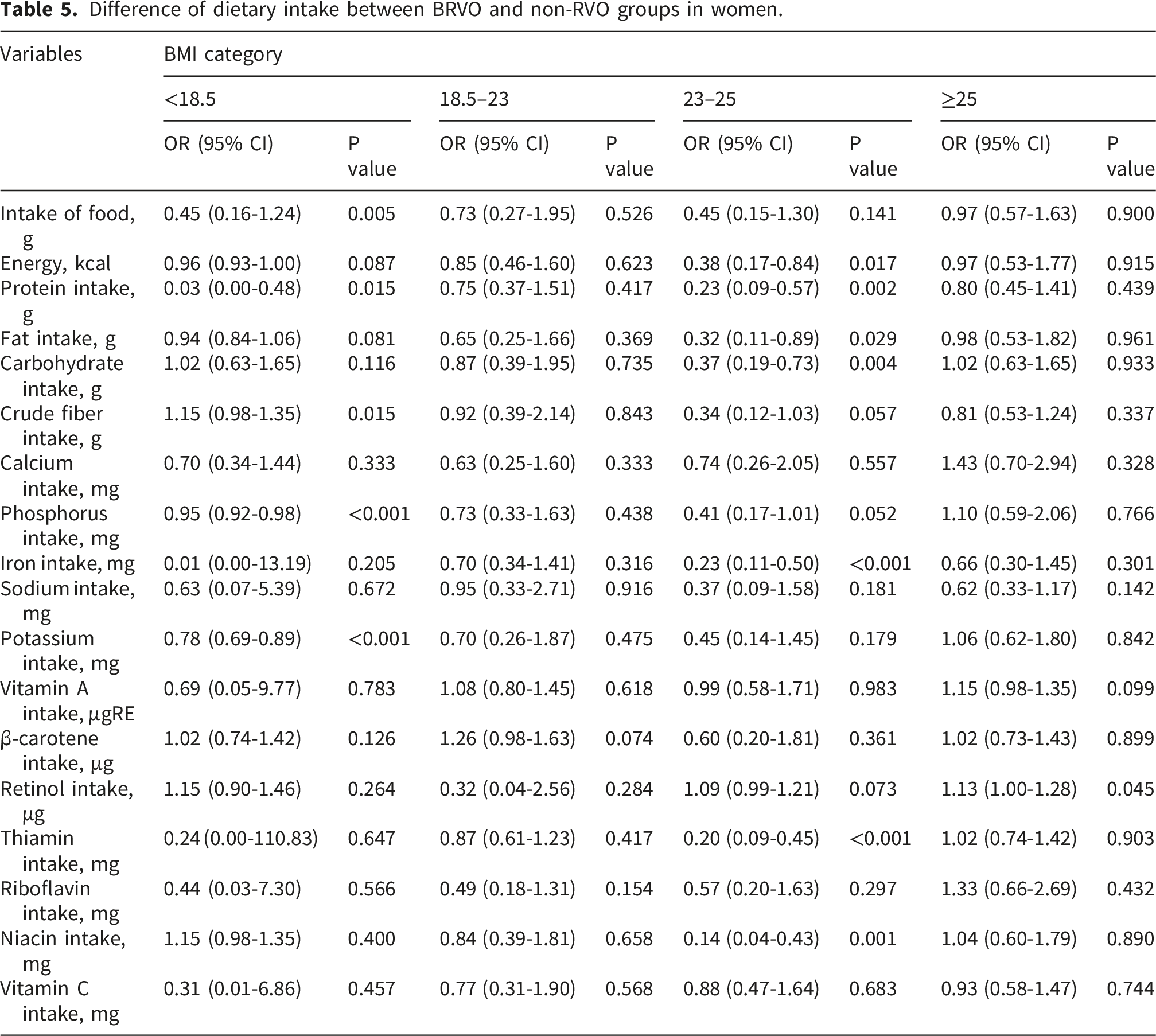
In the BMI 23–25 category, the overall differences were minimal in both sexes. Among women, iron intake was significantly lower in the BRVO group (r = –0.25, P < 0.001), whereas most other nutrients did not differ. In men, no significant differences were observed in any dietary variable within this BMI range.
In contrast, among men with BMI 18.5–23, several nutrients showed significant differences. Protein intake was lower in the BRVO group (r = –0.03, P = 0.012), along with fat intake (r = –0.04, P = 0.061) and potassium (r = –0.00, P = 0.003). Additionally, reductions in micronutrients such as vitamin A and β-carotene were observed. In women within the same BMI category, no significant dietary differences were found.
In the underweight group (BMI <18.5), both men and women with BRVO had lower food intake compared to non-RVO groups (men: r = 0.00, P = 0.009; women: r = –0.00, P = 0.002).
Additional sensitivity analyses using collapsed BMI categories and standardized nutritional variables yielded results broadly consistent with the primary analyses (Supplemental Table S2 and S3). Restricted cubic spline analyses suggested non-linear associations for most dietary variables, with a few exceptions, including total energy and phosphorus intake in women.
Discussion
This study demonstrates that lower nutrient intake, age, hypertension, and BMI may contribute to the risk of BRVO in the Korean population, based on data from the 2017–2021 KNHANES. As the most recently released dataset, KNHANES 2017–2021 provides an up-to-date representation of the current ocular health status of Koreans. To our knowledge, this is the first study to investigate the associations between systemic conditions, BMI, dietary nutrient intake, and BRVO risk using this nationally representative dataset.
Previous clinical studies have reported that age is significantly associated with the risk of RVO.22,23 The meta-analysis by Rogers et al. showed that the prevalence of BRVO increased with age, from 1.57 per 1,000 in individuals aged 40–49 years to 10.32 per 1,000 in those aged ≥80 years, which is approximately a sevenfold rise. 8 Hypertension is also recognized as a traditional risk factor for RVO, 24 and lowering blood pressure has been linked to a reduced risk. 25 In the present study, both age and hypertension were identified as factors associated with BRVO, regardless of sex.
Although diabetes has been identified as a potential risk factor for RVO in earlier studies,24,26 a large meta-analysis found a significant association only with CRVO, not with BRVO. 27 Supporting this, a recent Korean study reported that well-controlled diabetes was linked to a 55% lower prevalence of BRVO. 28 Consistent with these findings, diabetes was not significantly associated with BRVO in either men or women in our study.
Several previous studies have reported a higher risk of BRVO among individuals with elevated BMI. 24 A large population-based cross-sectional study involving 155,466 subjects similarly demonstrated that the presence of RVO was associated with increased BMI. 29 Park et al. further suggested that the elevated relative risk observed in overweight and obese populations may be explained by obesity-related comorbidities such as diabetes, hypertension, and hypercholesterolemia, as the significance diminished after adjustment for these covariates. 30 In line with these findings, our study also revealed an increasing trend of BRVO prevalence from normal weight to overweight and obese groups. However, this association was statistically significant only in women, while no significant relationship was observed in men. These results indicate that the link between BMI and BRVO may be stronger in women, suggesting that sex-specific factors could play an important role. Future studies on BRVO might therefore consider stratified analyses by sex when evaluating the impact of BMI. Moreover, further research is warranted to examine more detailed BMI categories and to compare the odds ratios of BRVO across different obesity subgroups, which may help clarify the dose–response relationship between adiposity and BRVO risk.
Although lower BMI is often accompanied by reduced total energy intake in population studies, previous intervention and cohort studies have shown that dietary composition and specific nutrient patterns are associated with vascular outcomes independent of total caloric intake or body weight.31,32 Recent evidence highlights the role of diet in the prevention and management of RVO, with studies showing that higher consumption of fish, nuts, fruits, and vegetables exerts protective effects, while deficiencies in vitamins A, C, D, and folic acid act as independent risk factors due to their anti-inflammatory and vascular-protective properties. 16 A large population-based study further reported that sufficient magnesium intake reduced the odds of RVO by 64%, 33 emphasizing the importance of specific micronutrients. In our study, men with BRVO consistently showed lower intake of a wide range of nutrients, suggesting generally lower overall dietary intake, whereas women demonstrated more selective patterns, particularly in protein, iron, fiber, and phosphorus, with iron intake being lowest in the overweight group. Importantly, as even the intake of key macronutrients such as protein and fat was associated with BRVO, we cautiously suggest that ensuring a balanced and sufficient intake of these fundamental nutrients may benefit certain patient groups.
Given the lower total food and energy intake observed in participants with BRVO, the reduced intake of multiple nutrients may partly reflect an overall reduction in dietary quantity rather than isolated deficiencies of specific nutrients. Nevertheless, several nutrient differences remained significant after adjustment for age, suggesting that the observed associations are not solely explained by reduced caloric intake or chronological aging.
These findings, consistent with prior literature, suggest that lower nutrient intake—whether global or nutrient-specific—may be related to the presence of BRVO, and that sex-specific dietary approaches could be considered in future preventive strategies. Nevertheless, lower intake in older individuals may partly reflect age-related physiological and behavioral changes in diet, and residual confounding related to aging and overall undernutrition cannot be fully excluded. Future studies incorporating validated overall diet quality indices, such as Healthy Eating Index–type or dietary diversity measures, may provide a more comprehensive understanding of how overall dietary patterns relate to BRVO beyond single-nutrient analyses.
Several limitations should be acknowledged when interpreting our findings. First, because this was a cross-sectional study, we were unable to establish causal relationships between risk factors and the occurrence of RVO. Future prospective longitudinal cohort studies are needed to clarify causality. Second, the prevalence of RVO may have been underestimated since only macula-centered fundus photographs were evaluated, which could have led to missed diagnoses of peripheral RVO. In addition, previous RVO events without clinically visible residual retinal changes may not have been detected. Third, only participants with gradable fundus photographs were included in the analysis, which may have introduced selection bias; to address this, we compared baseline characteristics between included and excluded participants (Supplemental Table S1). The excluded participants were generally younger and had lower cardiometabolic risk profiles compared with the included population. In addition, dietary intake was assessed using self-reported nutritional surveys without biochemical measurements, and therefore actual nutrient deficiencies or circulating nutrient levels could not be determined. Furthermore, supplementary analyses suggested that several dietary variables may exhibit non-linear associations with BRVO risk, including potential U-shaped patterns at extreme intake levels. Therefore, the associations estimated using linear regression models should be interpreted with caution. Finally, because the study population consisted of Korean adults, caution is warranted when generalizing these findings to other ethnic groups. Nevertheless, this study is the first to investigate the relationship between body mass index, nutritional intake, and retinal vein occlusion in the Korean population. Importantly, our analysis stratified risk factors by sex, providing novel insights into gender-specific associations. Another notable strength lies in the relatively large sample size compared with previous population-based surveys. Furthermore, the large sample size and the use of standardized, nationally representative KNHANES data enhance the reliability and generalizability of our findings.
Conclusion
We found that nutritional inadequacies and metabolic risk factors, such as hypertension and elevated BMI, may increase the risk of BRVO. By analyzing risk factors separately in men and women, we identified sex-specific associations that provide novel insights. These findings highlight the importance of dietary management and metabolic health monitoring as potential strategies for reducing the burden of BRVO in the Korean population.
Supplemental material
Supplemental material - Associations of nutritional intake and body mass index with branch retinal vein occlusion: A cross-sectional study using data from a Korean national survey
Supplemental material for Associations of nutritional intake and body mass index with branch retinal vein occlusion: A cross-sectional study using data from a Korean national survey by Bokyung Kim, Eunseob Kim, Yun Tae Kim and Mingui Kong in Science Progress.
Footnotes
Acknowledgement
Artificial intelligence–based tools were used to assist with language editing and clarity during manuscript preparation. The authors take full responsibility for the content, analysis, and interpretation of the data.
Ethical considerations
This study was conducted in accordance with the tenets of the Declaration of Helsinki, and was approved by the institutional review board IRB at the Kangbuk Samsung Hospital on August 23rd, 2024 (approval number: 2024-08-022) in Korea.
Consent to participate
Given the retrospective design of this study and the use of anonymized data, requirements for informed consent were waived by the institutional review board IRB at the Samsung Medical Center in Korea.
Author contributions
Conceptualization: Kim B, Kong M. Data curation: Kim B, Kim E, Kim YT, Kong M. Formal analysis: Kim YT, Kong M. Investigation: Kim B, Kong M. Methodology: Kim B, Kim E, Kim YT, Kong M. Validation: Kong M. Writing – original draft: Kim BK, Kim YT, Kong M. Writing – review & editing: Kong M.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.