
Abstract
To develop a predictive model to assess the risk of peri-operative hypothermia occurrence in children undergoing thoracoscopic lobectomy and validate its effectiveness. 172 children who underwent thoracoscopic lobectomy were randomly divided into a training set of 124 cases and a validation set of 48 cases in a 7:3 ratio. The study found a 33.1% incidence of intraoperative hypothermia (IPH) in children undergoing thoracoscopic lobectomy. Logistic regression analysis was performed using SPSS 26.0 to screen influencing factors, establish a risk prediction model, and draw the receiver-operating characteristic curve. Univariate analysis identified anesthesia-skin incision time, operating-room temperature, humidity, basal body temperature, end body temperature, and body temperature half an hour after anesthesia as influencing factors. Multivariate logistic regression revealed anesthesia-skin incision time (odds ratio (OR) = 1.595), operating-room humidity (OR = 4.094), and body temperature half an hour after anesthesia (OR = 112.595) as independent predictors. The nomogram model demonstrated an excellent discrimination with area under the curve (AUC) of 0.989 (95% confidence interval (CI): 0.976–1.000), maximum Youden index of 0.94, sensitivity of 1, specificity of 0.94, and cutoff value of 0.195. The Hosmer-Lemeshow test (χ2 = 1.751, P = 0.195) and bootstrap resampling (consistency coefficient = 0.947) confirmed the model's goodness of fit, internal consistency, and stability. Validation set results are similar to those in the training set, with an AUC of 0.989 (95% CI: 0.969–1.000), a sensitivity of 1, a specificity of 0.929, and a calibration curve error of 0.032 (<0.05), indicating high predictive accuracy. These findings suggest nomogram is a robust tool for predicting IPH in the pediatric thoracoscopic lobectomy.
Introduction
Intraoperative hypothermia (IPH) is, by definition, the phenomenon of a patient's core body temperature of less than 36°C during surgery, or the phenomenon in which the rate of heat loss is greater than the rate of heat generation. 1 The incidence of IPH is particularly high in thoracoscopic lobectomy due to the long operative time, the need for children to be exposed to laminar flow for a long time, and chest lavage. Compared with adults, children have smaller body surface area and large proportion of their core heat is lost through non-evaporative heat dissipation mechanisms such as conductivity, convection, and radiation. 2 Besides the physical factors, children are also vulnerable to IPH because of the inability of their weak central nervous system to effectively regulate body temperature and less subcutaneous fat tissue. 3 Studies have suggested that the occurrence rate of IPH in children is as high as 45–55%. 2 IPH in children leads to complications such as post-operative chills, tissue hypoxia, coagulopathy, delayed anesthesia recovery, delayed wound healing, and wound infection.4,5 This prolongs the hospitalization time of children and increases the financial burden on their families.
The action monitoring indicators outlined in the “Action Plan for Improving Surgery Quality and Safety (2023–2025)” 6 issued by the National Health Commission in 2023, proposed two national monitoring indicators: a gradual increase in the active warming rate during surgery and a gradual decrease in the incidence of hypothermia during surgical anesthesia. At the same time, clinical medical staff and anesthesiologists have made relevant improvements since the release of the “expert consensus on the prevention and treatment of hypothermia in perioperative patients (2023),” however, the statistical results of some hospitals in Beijing from 2019 to 2021 show that the active warming rate during surgery was only 26.3%. 7 Therefore, formulating reasonable and scientific warming measures is of crucial significance in decreasing the incidence of hypothermia during surgery in children undergoing thoracoscopic lobectomy. As for now, studies in China on IPH in patients undergoing thoracoscopic lobectomy mostly focused on investigating its prevalence, analyzing associated risk factors, 8 and exploring nursing intervention. 9 Also, most of these studies involve adults, and hence effective risk prediction model to predict the possibility of hypothermia during surgery in children undergoing thoracoscopic lobectomy is lacking.
Therefore, this study was performed to construct a risk prediction model for IPH in children undergoing thoracoscopic lobectomy. The objective focuses on establishing a clinically valuable tool for medical staff to identify high-risk groups, reduces the incidence of post-operative hypothermia in children, and improves the quality of their post-operative recovery.
Methods
Study design and population
This study is a retrospective study. A total of 172 children who underwent thoracoscopic lobectomy under general anesthesia in our hospital were selected from January 2022 to June 2024. The inclusion criteria comprised of the following: (1) neonates and young children aged 0–72 months; (2) undergoing elective surgery under general anesthesia; (3) thoracoscopic surgery; and (4) legally authorized representatives providing written informed consent for study enrollment, with explicit documentation of voluntary participation. The exclusion criteria comprised of: (1) core body temperature >38°C within 3 days before surgery; (2) abnormal body temperature metabolism; (3) receipt of mild hypothermia treatment during the peri-operative period; and (4) sudden drop in body temperature within 5 min after the start of surgery or fall-out of the temperature probe during surgery.
Sample size
The sample size is calculated as 5–10 times the number of independent variables in regression analysis. According to the literature review, the number of statistically independent variables is 19. Since 10–20% of the samples might leave a few fields blank, a sample size of at least 156 cases is required. To ensure the effectiveness of the results, this study included 172 effective patients. Patients were randomly assigned in a 7:3 ratio to form a training set of 124 patients and a validation set of 48 patients using the Sample function in the R language.
Study procedures
To obtain reliable results, we trained anesthesiologists and anesthesia nurses in temperature management, temperature measurement, and data collection. Nasopharyngeal temperature measurement is most commonly used in patients with general anesthesia and intubation; it can also be used in patients with laryngeal mask ventilation, because the measurement site is closer to the brain and it is easier to measure the temperature. 10 Intraoperative thermoregulatory monitoring was conducted via nasopharyngeal placement of a temperature sensitive probe, which recorded core body temperature trajectories from anesthetic induction until surgical completion in accordance with standardized physiological surveillance protocols. The anatomic reference parameter was defined as the linear interlandmark span extending from nose wing to the corresponding ipsilateral mandibular angle, measured in strict accordance with craniofacial anthropometric standards for precise anatomic localization. Then the temperature-sensitive probe is properly fixed with the tape. IPH is defined as a core body temperature lower than 36.0°C. The nasopharyngeal temperature is recorded every 5 min from the beginning of anesthesia to the end of operation. The operating-room temperature was obtained through the operating-room control system. All patients were routinely kept warm with quilts and inflatable heating blankets, and intravenous fluids and pleural lavage fluids were heated before use.
Data collection
A total of 172 patients who underwent thoracoscopic lobectomy were enrolled, including 124 patients in training set and 48 patients in validation set. A data sheet was developed to document demographic data and risk factors. This data sheet inclusion: (1) general data: sex, age, height, weight, and body mass index; (2) surgery-related data: American Society of Anesthesiologists (ASA) physical condition classification (hereinafter referred to as ASA classification), anesthesia duration, anesthesia skin incision time, operation time, intraoperative fluid volume, intraoperative blood loss, the total output, operating-room temperature, operating-room humidity, basal body temperature, end body temperature, heart rate in the room, hypothermia time after anesthesia, and wetness of dressings. General information and surgery-related information of patients were obtained through the hospital surgery anesthesia information system and nursing records. We have de-identified all patient details.
Ethical consideration
All patients indicated voluntary to participate in this study and provided written informed consent.
Statistical analysis
SPSS 26.0 and R 4.4.0 software running on R Studio was used for the data sorted and analyzed. Count data were expressed as frequency, composition ratio, and rate. Binary logistic regression was used for univariate analysis. Multivariate logistic regression was used to analyze the statistically significant independent variables in the univariate analysis and screen out independent influencing factors. The risk prediction model for IPH in children undergoing thoracoscopic lobectomy was generated with the help of R language packages such as caret, plyr, rms, epiDisplay, rmda, and gstummary. The robustness and clinical practicality of the model were assessed by using the Hosmer–Lemeshow (H–L) test, sensitivity, specificity, area under the curve (AUC), calibration curve, and decision curve analysis (DCA).
Results
Demographic characteristics
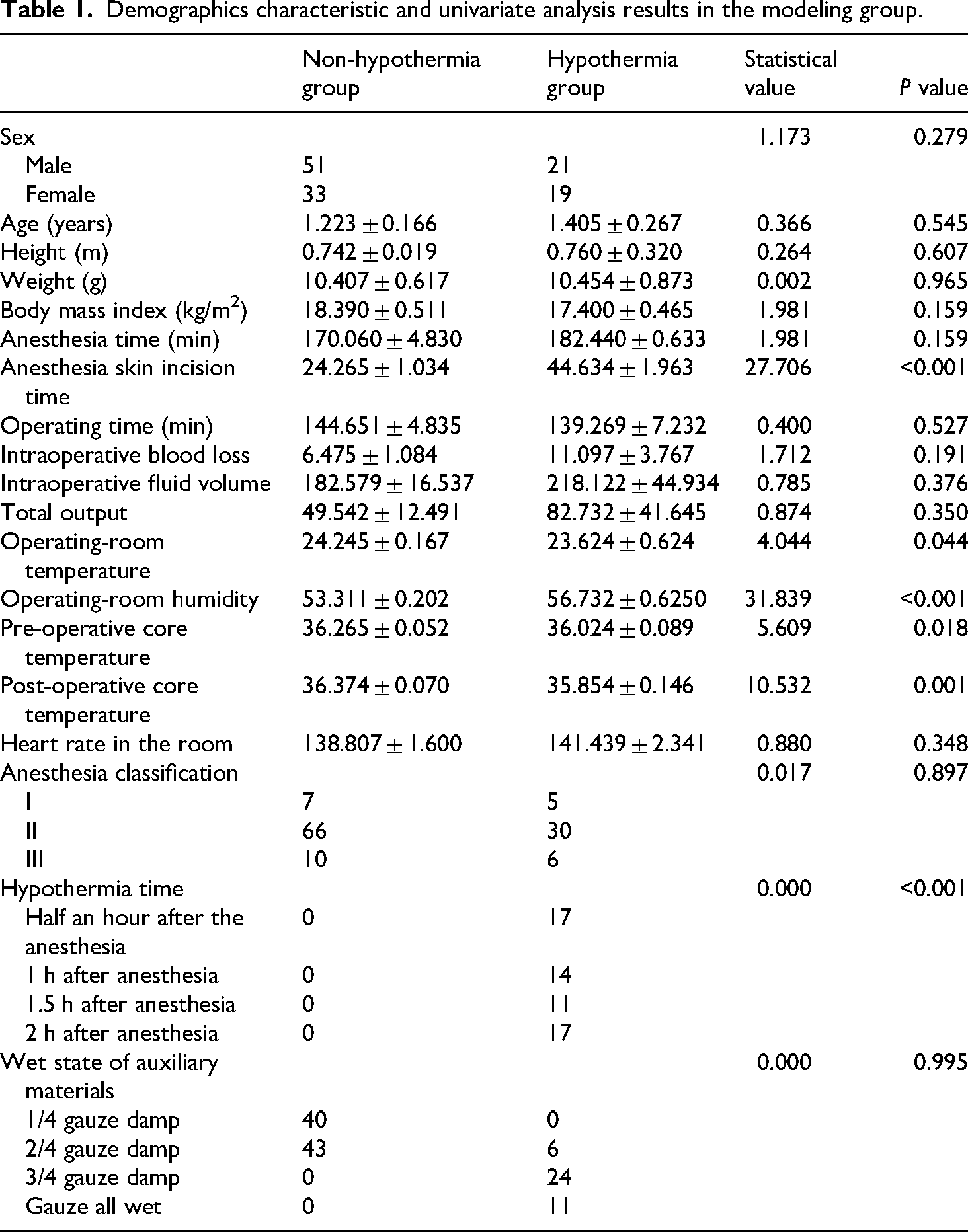
In total, 172 children were enrolled in this study and these participators with surgical modifications or incomplete data were excluded to ensure the reliability of the study. The training set comprised of 124 valid cases, of which 41 (33.1%) had IPH. A comparison of general information between the hypothermia group and the non-hypothermia group in training set is shown in Table 1. There were no significant statistical differences between these two groups (P > 0.05). Univariate analysis suggested that factors influencing IPH in children undergoing thoracoscopic lobectomy included anesthesia-skin incision time, operating-room temperature, operating-room humidity, basal body temperature, end body temperature, and body temperature half an hour after anesthesia.
Demographics characteristic and univariate analysis results in the modeling group.
Prediction model for IPH in children undergoing thoracoscopic lobectomy
We considered hypothermia during pediatric surgery as the dependent variable (no hypothermia = 0, hypothermia = 1). Multivariate logistic regression analysis (anesthesia-skin incision time, operating-room temperature, operating-room humidity, basal body temperature, end body temperature, and body temperature half an hour after anesthesia) was performed to screen predictive variables using the forward stepwise method. The results showed that anesthesia-skin incision time (odds ratio (OR) = 1.595), operating-room humidity (OR = 4.094), and body temperature half an hour after anesthesia (OR = 112.595) were independent factors influencing IPH (Table 2). The results of the logistic regression model were visualized and a nomogram model of IPH was generated (Figure 1). The factor with the largest contribution to hypothermia was the anesthesia-skin incision time, and the score was 100 when this time was 80 min.

Nomogram of IPH. IPH: intraoperative hypothermia.
Multiple regression results of intraoperative hypothermia.
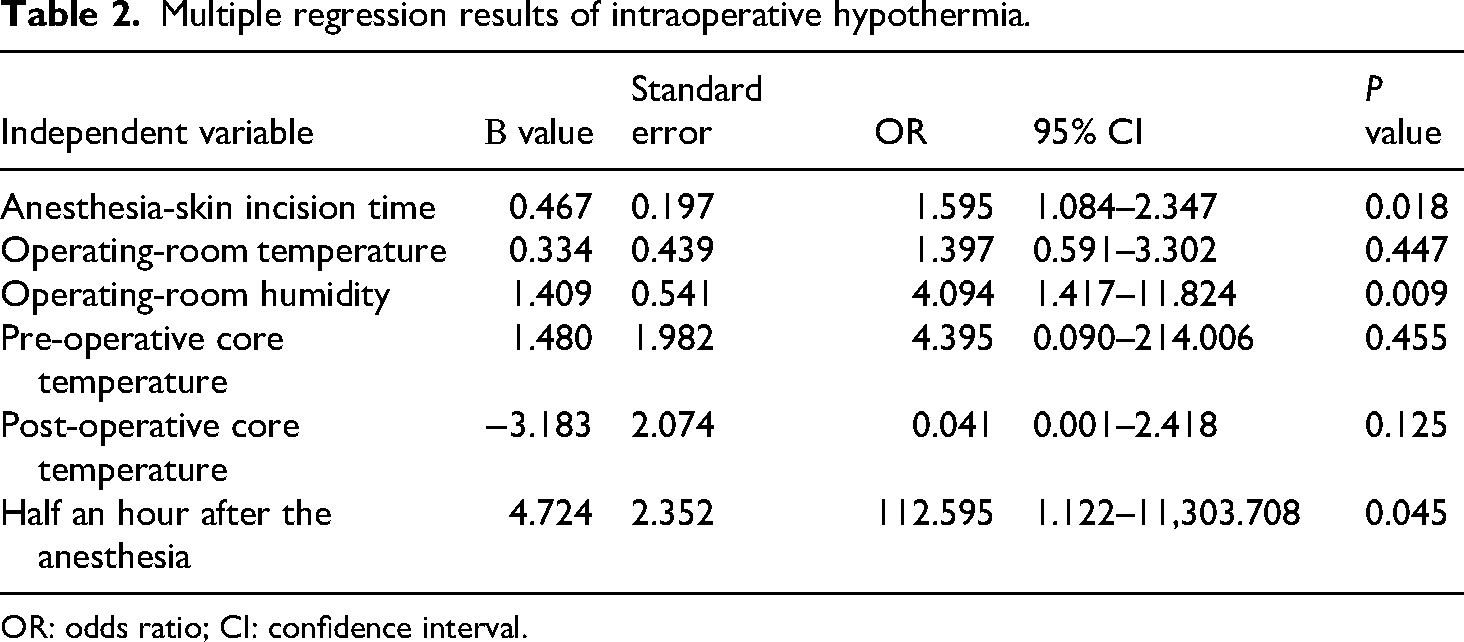
OR: odds ratio; CI: confidence interval.
Efficacy and internal validation of the IPH risk prediction model for children undergoing thoracoscopic lobectomy in the training set
Model discrimination
During the entire calculation process, the test variable was the specific predicted probability of the nomogram, and the state variable was the occurrence of hypothermia risk. “0” was used to indicate the non-occurrence of hypothermia, and “1” was used to indicate the occurrence of hypothermia. Finally, the receiver-operating characteristic curve for risk prediction was obtained (Figure 2). The AUC value was 0.993 (95% confidence interval (CI): 0.984–1.000), confirming that the discrimination of this model was quite obvious. In the entire curve, the maximum Youden index was 0.94, the sensitivity was 1, the specificity was 0.94, and the corresponding cutoff value was 0.195. This indicates that the probability of hypothermia calculated by the nomogram was ≥0.644, implying a high risk.

Receiver-operating characteristic curve.
Model calibration
The H–L test was used to check the calibration ability of this model. The χ2 and P values were 1.751 and 0.988, respectively, which had indicated the nomogram model possess a high sense of predictive accuracy (Figure 3).

Calibration curve of the intraoperative hypothermia risk prediction model for children in the training set.
Internal consistency, stability, and clinical utility of this model
The bootstrap resampling analysis was used to prove the stability of the model. After 1000 sampling times, the consistency coefficient was 0.947, which proved that the model had good internal consistency and high stability. DCA demonstrated that superior net clinical benefit for the nomogram-based model of IPH in thoracoscopic surgical cohorts compared to both “total intervention” and “no intervention” strategies, indicating its enhanced clinical applicability for targeted risk mitigation (Figure 4).

DCA curve of the risk prediction model for intraoperative hypothermia in the training set. DCA: decision curve analysis.
External validation of the risk prediction model for IPH in children undergoing thoracoscopic lobectomy
The AUC value for the validation set data was 0.989 (95% CI: 0.969–1.000), confirming that the discrimination of this model was obvious. According to the maximum Youden index of 0.94 in the training set, the cutoff value corresponding to the validation set was 0.195, the sensitivity was 1, and the specificity was 0.929. The average error of the calibration curve in the validation set was 0.032 (P < 0.05), demonstrating that this model had good predictive accuracy. The DCA showed that high-risk values >0.39 had greater net benefits, suggesting that the nomogram model had good clinical practicality. At the same time, this DCA suggested that the net benefit of high-risk value >0.39 was greater, revealing that this model had very good clinical operability.
Discussion
Key findings
The result of our study is that the incidence of IPH in children undergoing thoracoscopic lobectomy was 33.1%, which was similar to the findings of Gao et al. 11 and Sun et al., 12 but lower than the 45–52% incidence of hypothermia in pediatric surgery in studies conducted in countries other than China. 13 It might be related to the small-sample size of this study, or because clinical staff realized that IPH had many adverse effects on the patient's body, necessitating special attention to this issue in children. Much evidence-based nursing evidence has been applied to peri-operative nursing. 14 Our department has explained the “Operating Room Nursing Practice Guidelines” 15 and provided theoretical and practical training on IPH to operating-room nurses to improve their understanding of IPH, strengthen active and passive warming of children, and reduce the incidence of IPH in children. However, the incidence of IPH in children is still as high as 33.1%, so it is necessary to promote research on pediatric hypothermia. This study purposed and trained a risk prediction model that can help operating-room nursing staff to identify children at high risk of IPH, increase the level of attention paid to these children, and develop targeted improvement measures to reduce the incidence of IPH in children, which eventually will improve patient prognosis, increase hospitalization comfort, and enhance medical quality.
Analysis of factors influencing IPH in children undergoing thoracoscopic lobectomy
The anesthesia-skin incision time of children was correlated with hypothermia and had a significant influence in predicting IPH. The possible reasons are as follows: difficult airway during anesthesia refers to the condition in which the child's airway is blocked and breathing is difficult due to abnormal airway structure, previous medical history, or adverse symptoms caused by surgery after anesthesia. Difficult airway prolongs the preparation time for intubation. Zhao et al. 16 showed that body temperature redistribution and net heat loss to the environment after anesthesia induction, led to a drop in the core body temperature. During general anesthesia, the child is initially positioned supine. After anesthesia intubation, the position is changed to a lateral position and fixed with a body position device. However, using a blanket to maintain the child's body temperature in this process is difficult. The difficulty lies in ensuring consistent coverage, leading to prolonged skin exposure, increasing heat dissipation. Surgeons often determine the opening position according to their own habits and the specific location of the patient's lesion. The surgical position is mostly lateral position, which exposes more skin tissue to the outside and increases the heat dissipation area. Before surgical incision, the skin of the surgical patient should be disinfected with a skin disinfectant. The hospital under study uses 0.5% iodine tincture disinfectant for repeated disinfection three times. An extremely wet disinfection cotton ball leads to the soaking of the auxiliary materials on the left and right sides of the child. Consequently, the wet auxiliary materials stick to the child's body, causing hypothermia. Further, the disinfectant cannot be pre-heated, reducing the disinfection effect. The disinfection area in thoracoscopic surgery is large, and the disinfectant needs to dry to achieve the disinfection effect.
Operating-room humidity is also an independent influencing factor of the hypothermia risk prediction model. This is consistent with the research results of Yan et al. 17 Although they mentioned that operating-room humidity has an effect on the occurrence of hypothermia, they did not provide a basis for the conclusion. Compared with ordinary wards, operating rooms have higher control requirements for indicators such as humidity, temperature, and cleanliness. Inappropriate operating-room humidity may increase the bacterial reproduction rate, reduce the patient's intraoperative comfort, and increase the risk of surgical incision infection and hypothermia. Since the air in the operating room is in circulation with the outside world, in order to improve the quality of humidity in the operating room, relevant departments of the hospital should formulate reasonable temperature and humidity setting standards, strengthen the quality control training of operating-room personnel, guide them to correctly control the indoor temperature and humidity, and regularly monitor and maintain the temperature and humidity in the operating room to ensure that the humidity is within a reasonable range.
The OR value of body temperature is the highest within half an hour after anesthesia, which is the most critical period to predict the risk of hypothermia in pediatric surgery. The research results show that the inhibition of tonic thermoregulatory vasoconstriction induced by anesthetics, redistribution of body temperature from core to periphery, and net heat loss to the environment are the main reasons for core hypothermia within half an hour after anesthesia, accounting for 89% of the cases.18–20 Large amounts of body heat flow rapidly to the periphery, and even an effective active heating system does not prevent core hypothermia within the first hour of surgery. During thoracoscopic surgery, measures such as anesthesia intubation and urinary catheterization are required after anesthesia induction. For children, the exposure area is large: the younger the child is, the more difficult it is to place a urinary catheter, the longer the exposure time, and the faster drop in the child's body temperature. Most pediatric patients use infusion pumps during surgery and cannot use heated infusion devices. This is also one of the main reasons for the rapid drop in body temperature in children within half an hour after anesthesia.
Good performance of the risk prediction model for IPH in children undergoing thoracoscopic lobectomy
In the present study, multiple hypothermia risk prediction models were developed and verified in multiple cohorts. However, the population of this study comprised of children undergoing thoracoscopic lobectomy, which was different from previous model studies, leading to the differences in risk factors. The successful establishment of this model could dynamically predict the risk factors for IPH in children undergoing thoracoscopic lobectomy, aiming to implement peri-operative warming measures for high-risk children, reduce the incidence of IPH, and improve the children’ prognosis. However, this study also had certain shortcomings. The research participants were all from the same hospital. In addition, there has been a result of less bleeding compared to other more common surgeries, resulting in slightly different results compared with other studies. Nevertheless, the study proved that the risk prediction model was more effective and has strong clinical practicality. In the future, prospective multicenter investigations with adequately powered cohorts will be essential to externally validate and refine the predictive algorithm, ensuring generalizability across diverse clinical settings.
Limitations
The limitations of this study included its single-center nature, limiting the generalizability of the findings. Therefore, further validation using larger, multicenter cohorts is needed. Additionally, the low incidence of hypothermia in our sample might have affected model stability, necessitating further refinement with expanded datasets. The following limitations of this study need to be noted when interpreting the results. First, in the variable screening stage, we used the stepwise forward selection method. Although this method is still widely used in the construction of clinical prediction models, it has been pointed out that it may tend to retain too many noise variables in relatively limited sample sizes, leading to bias in effect estimation. Therefore, the set of selected variables in this study may not be optimal, and there is uncertainty in the stability and reproducibility of the model. Future research can further adopt regularization strategies such as Lasso and Elastic Net, or combine with stable selection techniques such as bootstrapping to improve the robustness of variable screening.
Conclusions
In this study, multivariate logistic regression analysis was used to construct an intraoperative prediction model for the risk of IPH in children undergoing thoracoscopic lobectomy. The identified factors included the time from anesthesia induction to skin incision, operating-room humidity, and body temperature 30 min post-anesthesia. The model demonstrated a good predictive accuracy and practical clinical value, offering a reference for targeted warming measures to reduce hypothermia incidence, enhance surgical quality, and support post-operative recovery in pediatric patients.
Footnotes
Acknowledgements
We thank all participants who participated in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Special Research on Perioperative Nursing Quality Control Management by National Health Commission Hospital Management Research Institute and the Key Research and Development Plan Project of Xianyang City, Shaanxi Province (grant number S2024-ZDYF-ZDYF-SF-3032).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The original data cannot be made available to public due to the Ethics Committee restrictions because it contains patient privacy information. Non-sensitive outcome data may be obtained from the authors upon reasonable request.