
Abstract
Objective
This study aimed to assess the treatment success and prognostic variables in elderly patients with nasopharyngeal carcinoma (NPC) who underwent definitive radiation therapy between January 2018 and December 2023.
Methods
The study employed a retrospective design and utilized the database system of our institution, which is centralized in a single location. A total of 125 patients, aged 60 or older, who were diagnosed with undifferentiated carcinoma of the nasopharynx (UCNT) based on histological confirmation, were included in the study. The data collection period spanned from January 2018 to December 2023.
Results
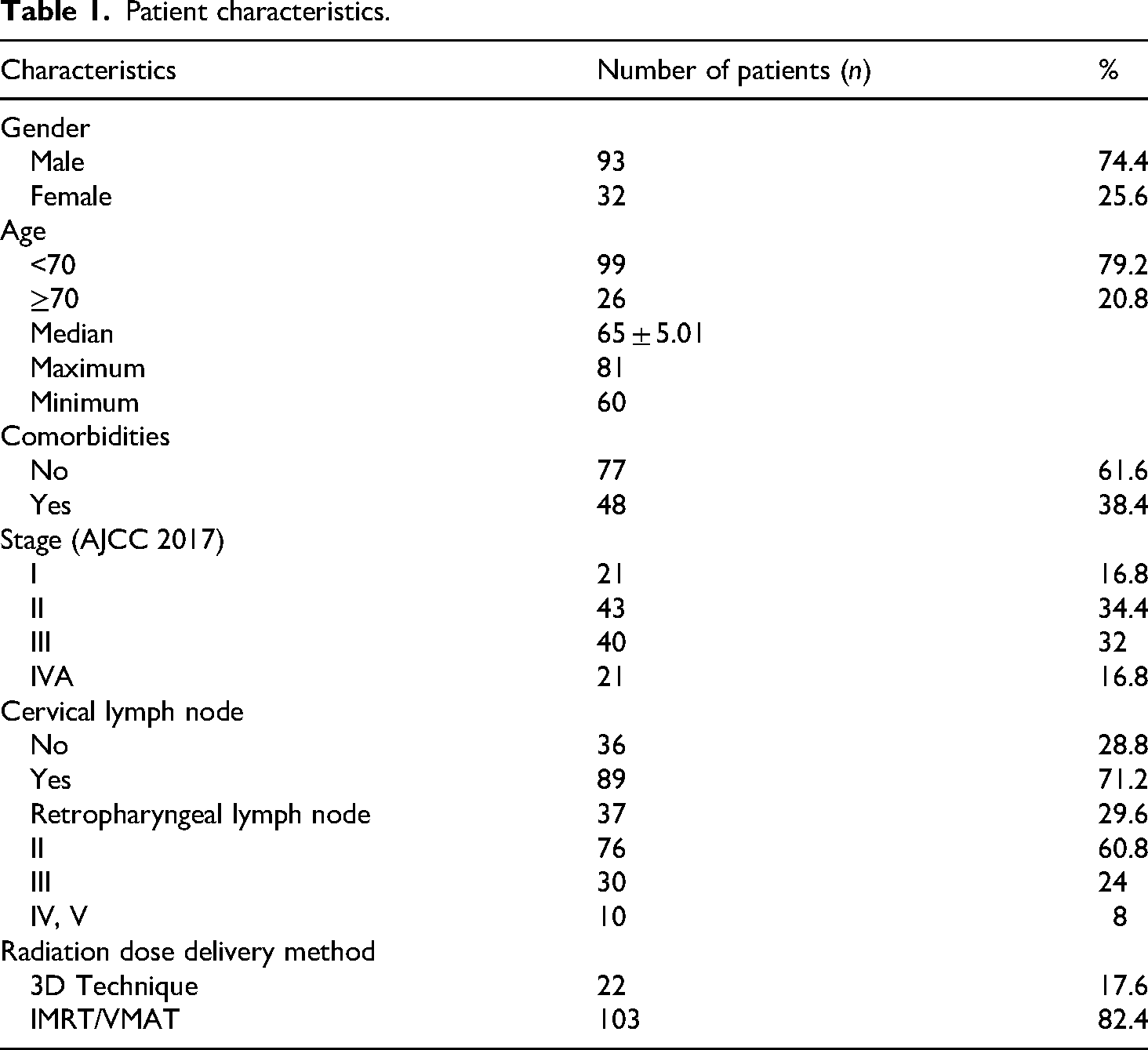
125 patients (93 male (74.4%), 32 females (25.6%); average age, 65.9 years) were identified, 16.8% were stage I, 34.4% stage II, 32% stage III, 16.8% stage IVA. The median follow-up for all 125 patients at the time of this analysis was 32.97 months (range 0.39–80.64 months). The mean OS was 64.75 ± 2.78 months. The 1-year and 5-year OS for the entire cohort were 93% and 69%, respectively. The mean disease-free survival (DFS) was 61.91 ± 2.87 months with a 5-year rate of 72%. According to multivariate analysis, overall survival was significantly influenced by both clinical stage (P < .05) and the presence of comorbidities. The majority of patients experienced good treatment tolerance, with grade 3 adverse effects including mucositis (6.4%), dermatitis (6.4%), and neutropenia (8.8%).
Conclusions
There has been a rise in the number of older patients, and they exhibit comparable clinical characteristics to the general population. The predicted criteria were clinical stage, age beyond 70, and comorbidities, each considered independently. Utilizing multidisciplinary therapeutic options is crucial for optimizing the chosen treatment for patients.
Introduction
Nasopharyngeal carcinoma (NPC) is a frequently diagnosed form of head and neck cancer in southern and southeast Asia, particularly in China, Indonesia, Vietnam, and other countries in the region. 1 Radiation therapy (RT), either with or without chemotherapy, is now considered the established treatment for nonmetastatic nasopharyngeal carcinoma (NPC). 2 Two consequences often arise in normal tissues within the irradiated area due to the nasopharynx's close proximity to vital organs, including the brain, brain stem, spinal cord, pituitary gland, optic nerve, and optic chiasm. These consequences have a significant impact on the patient's quality of life. The older population is more susceptible to experiencing treatment-induced adverse effects from chemotherapy and radiation. This is owing to their reduced ability to tolerate severe reactions and their higher likelihood of having concomitant comorbidities, which can further affect their general health status.
Multiple studies have demonstrated that being older and having other medical conditions are important factors that can predict both overall survival (OS) and disease-free survival (DFS).3,4 However, due to the stringent inclusion and exclusion criteria of clinical trials, only a limited number of elderly patients are eligible for enrollment, resulting in a lack of clarity regarding the most effective treatment strategies for this population.4,5 We conducted this study to analyze the treatment success and prognostic variables in elderly patients with nasopharyngeal carcinoma (NPC) who underwent definitive radiation therapy between January 2018 and December 2023.
Methods
Patient data collection
This retrospective study underwent independent review and received approval from the Institutional Review Board. Convenience sampling was employed; a total of 125 patients, aged 60 or above, who were diagnosed with undifferentiated carcinoma of the nasopharynx (UCNT) based on histological confirmation, were included in the study. The data collection period spanned from January 2018 to December 2023. This study was conducted in accordance with the Declaration of Helsinki (1975) as revised in 2024. The reporting of this study adheres to the STROBE guidelines. 6
The eligibility criteria for this study included recently diagnosed patients who were 60 years or older, had nonmetastatic UCNT that was confirmed by histological examination, did not undergo surgery, and were treated with definitive radiation therapy, with or without chemotherapy. Definitive radiotherapy (RT) was defined as the administration of a radiation dose equal to or greater than 66 Gy, in accordance with the latest recommendations. 2 The tumors were classified based on their histologic types according to the categorization established by the World Health Organization (WHO). 7 The tumor staging was conducted using the 8th edition 8 of the American Joint Committee on Cancer (AJCC) staging standard.
Patients with an unclear stage, pathologic therapy with a palliative goal, lack of treatment, or missing follow-up information were excluded from the study.
Treatment and survival
The treatment methods employed were radiation and chemotherapy. The patient underwent final radiotherapy, either with or without chemotherapy.
Radiation therapy: All patients were immobilized using a thermoplastic head–neck–shoulder mask to guarantee that the radiotherapy fields could be accurately reproduced on a regular basis. Both non-contrast CT scans (used for dose calculation) and contrast-enhanced CT scans (used for target delineation) were obtained, covering the area from the vertex to 2 cm below the sternoclavicular joint, with slice thickness set at 3 mm. The gross tumor volumes (GTVs) of the primary tumor and involved lymph nodes were identified based on the extent of disease visualized through CT, MRI, ¹⁸F-FDG PET-CT imaging, and findings from physical examination. Target contours for the primary site and nodal disease were drawn following the recommendations of the International Commission on Radiation Units and Measurements (ICRU) Report 62. 9 The clinical target volume was defined as the gross tumor volume with the inclusion of an extra margin of 5–10 mm. The recommended doses were 70 Gy administered in 33–35 fractions, with each fraction delivering 2.00–2.12 Gy. These doses were specifically prescribed for the planned target volumes that were determined based on the gross tumor volume of both the primary site and the lymph nodes. Each patient underwent daily radiation therapy, administered five times per week.
Systemic therapy: Patients received diverse systemic medicines such as Cisplatin, Gemcitabine, Docetaxel, and Fluorouracil.
For a patient with stage I: Radiotherapy alone is recommended. Stage II was divided into two subgroups: T2N0M0 and T0-2N1. For T2N0, radiotherapy alone is generally indicated. However, concurrent chemoradiotherapy may be considered if the tumor volume is large or if serum EBV-DNA levels are high. For T0-2N1, concurrent chemoradiotherapy is recommended. Stage III–IVA cases were divided into two subgroups: T3N0 and all other stage III–IVA cases except T3N0. For T3N0, concurrent chemoradiotherapy is indicated. For stages III–IVA (excluding T3N0), induction chemotherapy is recommended first, followed by concurrent chemoradiotherapy. All treatment decisions must be individualized based on each patient's condition. Our study focuses on elderly patients, and treatment regimens were selected according to their tolerance and overall health status. For example, in patients with multiple comorbidities or poor performance status, radiotherapy alone was considered instead of concurrent chemoradiotherapy.
The intensity of both acute and long-term side effects was evaluated according to the National Cancer Institute's CTCAE version 3.0, as well as the late toxicity grading system established by the Radiation Therapy Oncology Group and the European Organization for Research and Treatment of Cancer.
Study endpoints
This study assessed multiple survival endpoints, including overall survival (defined as the duration from randomization to death from any cause), disease-free survival (the time interval from randomization to either locoregional or distant metastatic recurrence, or death from any cause, whichever occurred first), locoregional recurrence-free survival (the period without confirmed locoregional relapse), and distant metastasis-free survival (the duration without evidence of distant metastatic spread).
Follow-up
Every patient received regular clinical follow-up by an otolaryngologist and/or radiation oncologist. These follow-ups occurred every 3 months during the first two years after radiation treatment, every 6 months for the following three years, and annually afterward. The histological examination confirmed the presence of local and regional recurrence. The diagnosis of distant metastases was confirmed through either pathological or radiological evidence. At each follow-up,10,11 treatment-related toxicities were evaluated and rated using the RTOG radiation morbidity rating standards.
Statistical analyses
The two-tailed Pearson χ2 test (or Fisher's exact test when categorical variable values were ≤5) was used to analyse categorical variables. Survival was assessed using the Kaplan–Meier method, and any variation in survival was analyzed using the stratified log-rank test. The Cox proportional hazards model was employed for multivariable analysis to determine the combined impact of prognostic variables on survival. Statistical significance was determined as having a P-value less than .05.
Results
Demographic characteristics
Between January 2018 and December 2023, a group of 125 patients who had been diagnosed with UCNT by pathology were enrolled. Out of the total number of patients, 93 were male patients, accounting for 74.4% of the population. On the other hand, there were 32 female patients, making up 25.6% of the population. This results in a female-to-male ratio of 2.9:1. The mean age of the patients was 65.9 years, with the majority falling within the age range of 60–70 years (79.2%). In our study, the median age was 65 ± 5.01 years which the youngest patient was 60 and the oldest was 81 (Table 1). The tumor stage that occurred most frequently was stage II, accounting for 34.4% of cases. The distribution of the remaining stages was as follows: 16.8% were stage I, 32% were stage III, and 16.8% were stage IVA. During the presentation, the proportion of cervical lymph nodes was 71.2%, with the highest frequency observed in cervical lymph node group 2 (60.8%). Out of the 48 patients, comorbidities were present, with cardiovascular disorders being the most prevalent (36.8%).
Patient characteristics.
Each patient underwent final radiation therapy, with 41.6% receiving radiation alone, 34.3% receiving contemporaneous chemoradiation, and 24% receiving induction chemotherapy followed by chemoradiation. The predominant treatment regimen in concurrent chemoradiation was Cisplatin 1, 22, 43, accounting for 44.8% of cases (Table 2).
The treatment characteristics.

Survival
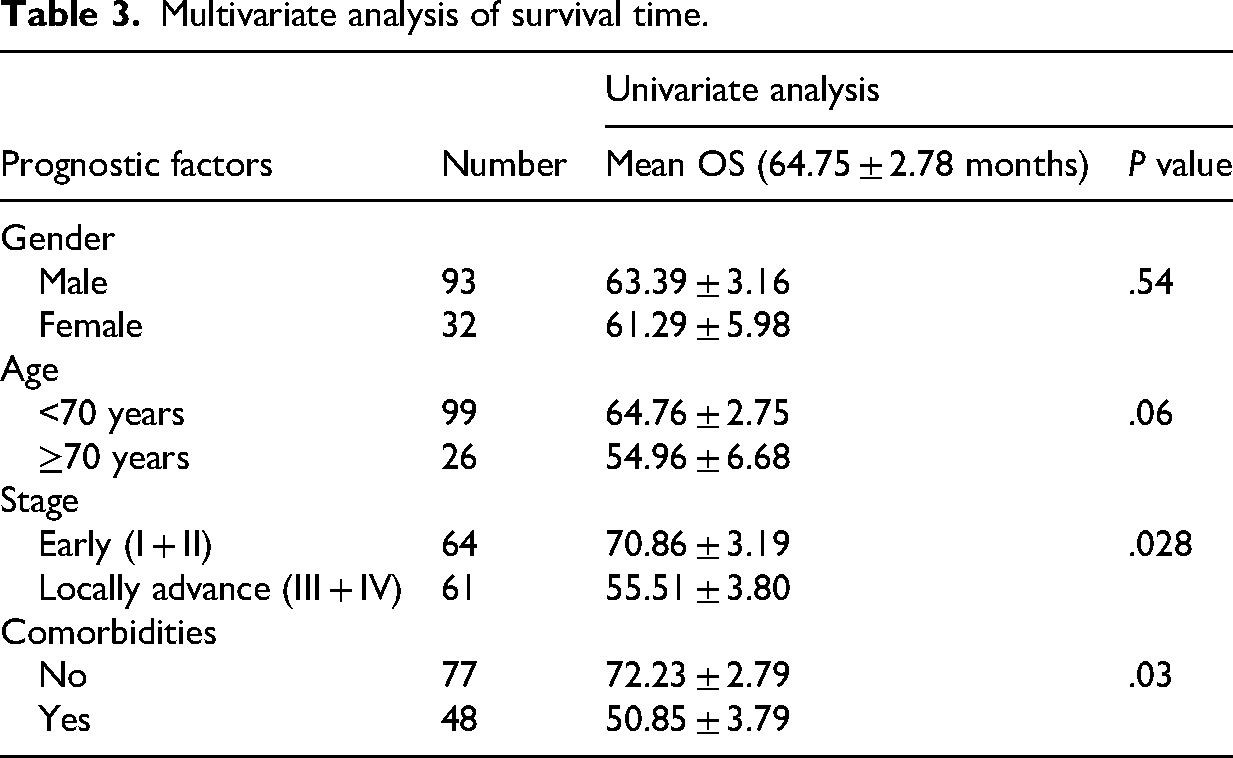
The overall reaction rate was 80%, with 80% of participants achieving a complete response and 20% achieving a partial response. The average operating system (OS) duration was 64.75 ± 2.78 months. The one-year and five-year overall survival rates for the total group were 93% and 69% respectively. The average disease-free survival (DFS) was 61.91 ± 2.87 months, with a 5-year rate of 72%. The average operating system (OS) duration for patients younger than 70 years was 64.76 ± 2.75 months, while for patients over 70 years it was 54.96 ± 6.68 months (P > .05). There was a statistically significant difference (P < .01, Table 3) in the survival rates of patients with comorbidities (mean overall survival of 50.85 months) compared to individuals without comorbidities (mean overall survival of 72.23 months). Patients in the early stage had a considerably longer overall survival (OS) of 70.86 months compared to those in the advanced stage, who had an OS of 55.51 months (P < .05).
Multivariate analysis of survival time.
Acute and late adverse effect
Patients commonly encountered the normal acute and delayed side effects of radiation and chemotherapy, such as dry mouth (xerostomia), skin inflammation (dermatitis), inflammation of the mouth and throat (oral and pharyngeal mucositis), and low white blood cell count (neutropenia). The majority of patients discontinued their therapy for less than 7 days due to the harmful effects of the medication and the presence of other medical conditions. The grade 3 toxicity included mucositis (6.4%), dermatitis (6.4%), and neutropenia (8.8%). The most common long-term consequence observed was neck fibrosis, which occurred in 27.2% of cases. Trismus was another frequently reported impact, occurring in 15.2% of cases. No instances of central nervous system necrosis were found, as indicated in Table 4.
Incidence of treatment complications.

Discussion
NPC is rare in most parts of the world, but more common in Asian populations, particularly those with Southern Chinese or Southeast Asian ancestry. The unique epidemiological characteristics of NPC indicate that its development is a complex, multistep process involving interactions among Epstein–Barr virus (EBV), inherited genetic susceptibility, and various environmental factors, such as tobacco use, specific dietary habits, and occupational hazards. The combination of genetic predisposition and environmental factors plays a role in its distribution. Specifically, Epstein–Barr virus (EBV) infection, genetic predispositions, and dietary habits like consuming salted or preserved foods (which are often seen in Chinese people) are major contributing factors. An elevated occurrence of NPC was noted in older patients12,13 residing in regions where the disease is prevalent. In addition, for a nonendemic region, a second peak of NPC risk by ages 65–79 years has been discovered emerging. 14 The definition of elderly patients varied among the research. In this particular investigation, we classified “elderly patients” as individuals who were 60 years of age or older. The mean age was 65.9 years, with the majority falling within the range of 60–70 years old (79.2%). The female-to-male ratio is 2.9:1, which is comparable to the GLOBOCAN 2020 figures for the overall population of Vietnam, where the male-to-female ratio is 2.89:1.1. 1 Elderly individuals often experience a higher prevalence of medical comorbidities, including cardiovascular diseases, metabolic disorders, chronic renal disease, and lung diseases. These conditions can significantly impact their overall health and the progression of their therapy. In our study, we observed comorbidities in 48 (38.4%) patients, with cardiovascular disorders being the most prevalent. In Ying Huang et al.'s 4 investigation on older patients with NPC, comorbidities were seen in a range of 22.4% to 58%, as determined by the Charlson Comorbidity Index (CCI) or the Adult Comorbidity Evaluation-27 (ACE-27) (Impact of comorbidity).
The proportion of cervical lymph nodes was 71.2%, with the highest frequency observed in cervical lymph node group 2 (60.8%), followed by retropharyngeal lymph node (29.6%) and group 3 (24%). The outcome was comparable to the last investigation. A multicenter study conducted in 2012 on patients with nasopharyngeal carcinoma (NPC) revealed that 85% of NPC cases were accompanied by lymphadenopathy. The retropharyngeal region is implicated in 69% of cases, while level II lymph nodes are involved in 70% of cases. The cumulative probabilities of nodal involvement at levels III, IV, and V are 45%, 11%, and 27%, respectively. The low-risk node groups consisted of the supraclavicular, levels IA/IB and VI nodes, and parotid nodes. The frequencies of involvement in these groups were 3%, 0%, 3%, 0%, and 1%, respectively. 15 The tumor stage that occurred most frequently was stage II, accounting for 34.4% of cases. The distribution of the remaining stages was as follows: 16.8% stage I, 32% stage III, and 16.8% stage IVA. Patients with locoregionally advanced nasopharyngeal carcinoma (stages III–IVA) are typically managed with concurrent chemoradiotherapy rather than radiotherapy alone, given its superior local control and overall survival outcomes.16,17 However, in our study, patients were more likely to undergo de-escalation treatment as opposed to following normal guidelines. Approximately 50% of the patients had locoregionally advanced disease, but only 24% got induction chemotherapy, with the majority receiving radiation therapy alone (41.6%). The reason for this is that combining chemotherapy with radiation therapy can be dangerous, as the side effects caused by concurrent chemotherapy are significant. This treatment is not suitable for older individuals who are more likely to have poorer overall health and are less able to tolerate severe reactions, as well as having other existing medical conditions. Despite being a less intensive approach, a previous study reported favorable outcomes of radiation therapy alone in elderly patients, with 4-year overall survival and disease-free survival rates of 51.0% and 54.7%, respectively. 3
The median duration of follow-up for all 125 patients included in this analysis was 32.97 months, with a range of 0.39–80.64 months. The majority of patients (53.6%) successfully completed the treatment with a gap of less than 7 days. Patients had post-radiotherapy evaluation one month following treatment completion using RECIST 1.1 criteria. 18 The evaluation included clinical examination, maxillofacial MRI, whole-body CT, ENT endoscopy, and PET/CT. The complete response rate was determined to be 80%, whereas the partial response rate was 20%. During the time of this analysis, 19 patients succumbed to cancer recurrence or metastasis, whereas 5 patients died due to other causes such as COVID-19, heart failure, and so on. The average operating system (OS) duration was 64.75 ± 2.78 months. The whole cohort had a 1-year overall survival (OS) rate of 93% and a 5-year OS rate of 69%. Figure 1 illustrates the disease-free survival of all patients included in the study. The average disease-free survival (DFS) was 61.91 ± 2.87 months, with a 5-year rate of 72% (Figure 1). The literature review yielded results that were in line with earlier findings. Yu Liang et al. 19 showed that the 3-year and 5-year progression-free survival (PFS) rates for elderly patients with nasopharyngeal carcinoma (NPC) were 77.9% and 66.3%, respectively. Additionally, the 3-year and 5-year overall survival (OS) rates were 79.3% and 66.8%, respectively. The primary factor contributing to mortality was the recurrence and spread of the disease, with only a small number of individuals succumbing to other health conditions. In a matched cohort study, although the rates of complete locoregional response were similar, patients with nasopharyngeal carcinoma (NPC) aged 65 and older who received chemoradiotherapy had significantly worse survival compared to younger, demographically matched controls (5-year overall survival [OS]: 54.6% vs. 75.3%; 5-year cancer-specific survival [CSS]: 56.6% vs. 77.8%). 20 Huang et al. examined data from 1137 NPC patients aged 65 or above and found that their 5-year OS was only 50.4%, which is lower than that of the general population over 60 years old. 4 Overall survival analyses are shown in Figure 2, stratified by (A) all patients, (B) co-morbidities, (C) age, and (D) clinical stage. In our study, the mean OS tend to be longer for patients younger than 70 (64.76 ± 2.75 months) compared with patients over 70 years (54.96 ± 6.68 months); however, the difference is not statistically significant with P > .05. There was a significant difference (P < .01, Table 3) in survival between patients with comorbidities (mean OS 50.85 months) and patient without comorbidities (72.23 months). Similarly, patients with early stage had significantly longer OS (70.86 months) than advanced stage (55.51 months) (P < .05). The study on overall survival in elderly NPC found that Comorbidity as measured by CCI is a strong independent prognostic factor for OS. 4 Sommat et al. 21 also demonstrated that being over the age of 70 was significantly associated with poorer overall survival (hazard ratio [HR] 2.40; 95% confidence interval [CI], 1.44–4.00; P = .001) and reduced disease-free survival (HR 1.85; 95% CI, 1.02–3.36; P = .043).

Disease-free survival of all patients.

Overall survival. (A) All patients, (B) comparative OS in patients by co-morbidity, (C) by age, and (D) by clinical stage.
Patients undergoing high-dose radiation treatment in the nasopharynx region may develop acute adverse effects, including skin responses, stomatitis, dry mouth, hearing loss, and taste loss. A majority of patients (53.6%) discontinued their therapy for less than 7 days mostly because of treatment toxicities. There was a statistically significant difference in treatment delay between patients with comorbidities and those without comorbidities. The grade 3 toxicity included mucositis (6.4%), dermatitis (6.4%), and neutropenia (8.8%). The majority of patients underwent IMRT radiation, which effectively reduces the dose to the skin compared to previous techniques, resulting in a decreased incidence of dermatitis. 22 The elevated incidence of mucositis seen in our study can be attributed to the frequent occurrence of radiation doses to the oral cavity that exceed the permitted levels. This is commonly due to the involvement of the high-risk volume of nasopharyngeal carcinoma (NPC). 23 Radiotherapy for NPC is linked to late problems that can reduce the patients’ quality of life due to the close proximity of essential structures. The predominant late impact observed in our investigation was neck fibrosis, with a prevalence of 27.2%. This was followed by trismus, which had a prevalence of 15.2%. No instances of central nervous system necrosis were detected, and no cases with a severity score higher than 2 were identified. Our patients were administered state-of-the-art radiation procedures and were given instructions to perform medical exercises in order to minimize the occurrence of late problems associated with radiation therapy, such as trismus and fibrosis in the jaw and neck. We had the belief that it was imperative to minimize the occurrence of late complications resulting from radiation therapy.
Limitations
This study is subject to several constraints and potential problems. Firstly, the study employed a retrospective, observational design, meaning that it looked back at past data rather than conducting an experiment. The outcomes of the study relied on the completeness and accuracy of the medical records that were utilized. The retrospective design may lead to potential selection bias due to the single-center setting. Furthermore, the lack of a younger control group limits the strength of the study because it prevents comparison of outcomes across different age groups. Secondly, intensity-modulated radiation therapy (IMRT) is now the established and widely accepted treatment for older individuals with nasopharyngeal carcinoma (NPC). Nevertheless, in our research, a total of 22 individuals had 3D-radiation treatment. It is possible that some of the long-term harmful effects experienced by older patients in this study were not accurately assessed. For instance, the average duration of cranial nerve palsy was around 8 years. 24
Conclusions
The number of older patients has been rising, and they exhibit comparable clinical characteristics to the general population. The clinical stage, age over 75, and comorbidities were identified as independent prognostic factors. Utilizing multidisciplinary therapy strategies is crucial for maximizing the effectiveness of the chosen treatment for patients.
Footnotes
Acknowledgments
The authors declare that they have no acknowledgements to report.
Ethic approval
The studies were reviewed and approved by the Ethics Committee of Hanoi Medical University, Vietnam as the number: 3206/QĐ-ĐHYHN on February 5, 2022. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article. This study was conducted in accordance with the Declaration of Helsinki (1975) as revised in 2024. The reporting of this study adheres to the STROBE guidelines. 6 To protect patient privacy, all patient details were de-identified to ensure that individuals could not be identified in any way. This de-identification process was conducted prior to data analysis.
Author contribution
N.V.D. designed the study and supervised the research, data collection, and manuscript drafting, and collected and analyzed the data. D.D. contributed to study supervision, methodology, collected and analyzed the data, manuscript drafting, and manuscript revision. H.N.T., N.T.T.N., N.H.P., and A.V. supported data analysis and interpretation. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data utilized in this study are available upon contact with the corresponding author.