
Abstract
Achalasia cardia is quite uncommon worldwide. The patients treated with a retrievable fully covered self-expanding metallic stent shown a strong curative impact in this case study and follow up, which can serve as guidance for the clinical treatment of Achalasia cardia.
Introduction
Achalasia cardia (AC) is a rare functional disease brought on by primary esophageal motility disorder. This condition is primarily characterized by esophageal peristalsis disorder, lower esophageal sphincter (LES) hypertension, and weakened relaxation response to swallowing action1,2 and is generally thought to be brought on by neuromuscular dysfunction of the esophagogastric junction (EGJ). Reflux, retrosternal discomfort, and dysphagia are the primary clinical symptoms. 3 AC has a (0.03–1.63) and (1.8–12.6)/100,000 global incidence rate and prevalence, respectively. This disease tends to affect persons between the ages of 30 and 60 and has a similar incidence rate in men and women. As opposed to Asia and eastern areas, it is more prevalent in European and American nations.4,5,6 The most common AC therapy options include medication, botulinum toxin injection, balloon dilatation, and surgery. Peroral endoscopic myotomy (POEM), Heller's myotomy, and other surgical procedures are the most frequently utilized. 7 Both patients’ excellent results following endoscopically fully covered self-expanding metallic stent (FCSEMS) implantation provide a novel approach to the treatment of AC.
Case 1
Medical history
A male patient around 40s presented with a history of retrosternal burning and dysphagia for the past 15 years, with worsening symptoms over the past 5 years like greater pain behind the sternum, an increase in the sensation of choking after eating, and new symptoms such nighttime reflux of food, choking, and burping, all of which were given a dysphagia score of 3 according to worldwide nutrition experts (Table 1). A barium swallow was performed, which supported the diagnosis of AC. Endoscopy and upper gastrointestinal contrast examination are shown in Figure 1. His esophagus was clearly dilated with a maximal diameter of 4 cm, and the typical “bird's beak” sign is shown in Figures 1(d) and 2(a). Other tests are normal. After ruling out conditions linked to esophageal and gastric mucosal injury, the patient was initially diagnosed with grade II AC at the Lanzhou University Second Hospital (Lanzhou City, China) in December 2021 (an Eckardt score of 5, accompanied by some clinical signs such as weight loss of 5 kg, occasional dysphagia, retrosternal pain, and reflux symptoms, or imaging evidence of an esophagus with a maximum diameter of 4–6 cm), according to the Eckardt score, which rates clinical symptoms of AC.

Nasal gastroscopy and esophageal barium meal examination. (a) Dilatation of lower esophagus, (b) narrow cardia, (c) needle eye at cardia, and (d) dilatation of the lower esophagus, the sign of “beak-like.”
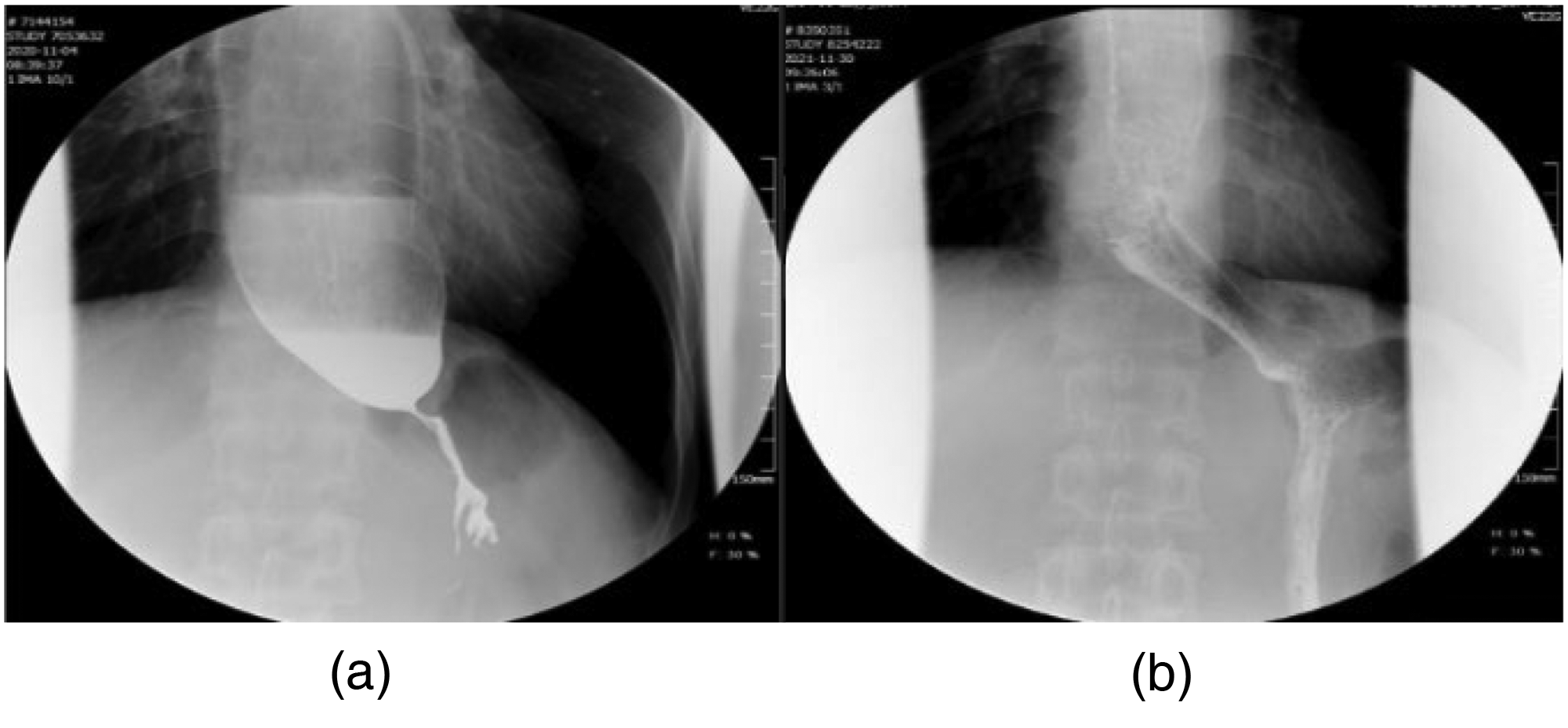
Upper gastrointestinal contrast. (a) Before treatment, the esophagus was dilated and the lower segment of the esophagus was funnel-shaped, like the sign of “beak-like,” (b) 1 day after the metal peritoneal esophageal stent was placed, the contrast medium in the esophagus, the stent and the portal of the esophagus passed smoothly.
Dysphagia scores are recommended by international nutrition experts.

Endoscopic FCSEMS implantation operation
The patient was generally in good and stable condition. The third day following hospitalization, an FCSEMS was implanted via the Through-The-Scope (TTS) method, after the patient had signed an informed consent form. The operator employed transnasal gastroscopy due to the severe stenosis of the cardia. The cardia was as narrow as a needle eye, and the total esophagus was dilated as seen via the scope. To inject contrast agent (Ioversol Injection, specification: 50 mL/bottle) for esophagography, the zebra guide wire (manufactured by Boston Science Company, model: M001465020, specification: 0.035in × 260 cm, Figure 3(a)) was introduced through the endoscope. The lower section of the esophagus displayed a transverse alteration, while the upper part of the esophagus was dilated, according to X-ray contrast (dynamic X-ray monitoring approximately 10 seconds postinjection revealed that approximately 80% of the contrast agent remained in the esophageal lumen, while only 20% passed through the cardia). An FCSEMS (manufactured by Nanwei Medical Technology Co., Ltd, model: MTN-SE-S-20-80-A-8-650, specification: 80 mm × 20 mm) was positioned along the zebra guide wire once the position of the narrow section had been confirmed (Figure 3(b)). Enter the mirror again and release the stent under the double monitoring of the endoscope and X-ray. Once more, the contrast agent can enter the gastral cavity without any problems. Through the guide tube in the nasopharynx, the stent-string is placed outside the body.

Esophageal metal peritoneal stent implantation under nasal gastroscope. (a) Guide wire was introduced into the gastric cavity, (b) the stent was released smoothly, (c) the stent was expanded, and (d) the stent was well expanded under X-ray radiography.
Postoperative treatment
Within 2 to 4 hours of the operation, the patient was recommended to consume warm water and liquid meals. The patient initially had nausea and acid reflux after eating, but these symptoms essentially vanished after receiving medications that suppressed acid production, treated emesis, and improved gastrointestinal motility. After the symptoms completely disappeared, he was instructed to take semiliquid and solid food without choking feeling, and dysphagia. A single point was awarded. Following surgery, the esophageal dilatation above the stent was greatly reduced, with a maximal diameter of 22 mm and an equivalent to half of a thoracic vertebra's transverse diameter. Smooth passage of the contrast material through esophagus, stent, and cardia (Figure 2(b)).
Reexamination and follow up
One month following the surgery, the patient underwent a re-examination in the outpatient department. Dysphagia score received a score of 1 and there were no symptoms such nighttime food reflux, choking, burping, etc., meanwhile, the weight of patient increased significantly. When the gastroscope was checked again, it was discovered that the stent had shifted and fallen off into the gastric cavity. Consequently, the original stent was removed under the supervision of endoscopy and X-ray, and an FCSEMS was then implanted in the lesion again (the specification, origin and placement method of the stent are the same as before). The stent was removed by endoscopy in March 2022 after the patient's evaluation revealed no unusual discomfort (Figure 4), and the integrated relaxation pressure (IRP) of the lower esophageal sphincter decreased from 22 mmHg pretreatment to 10 mmHg post-treatment. The patient had no abnormal symptoms after the operation, and regular re-examination was ordered. At 40 months post-stent removal, the patient remained asymptomatic. After telephone follow up, the patient has no symptoms such as post-sternal pain, eating choking, reflux, hiccuping, or choking after a normal diet. The dysphagia score is 1 point, and the His appetite has been significantly improved, with a weight increase of about 11 kg, meanwhile, the Eckardt scores reduced to 0 post-treatment.

Removal of the esophageal metal peritoneal stent under nasal gastroscope. (a) The distal end of the stent and (b) and (c) no erosion and ulcer of the cardia and esophagus mucosa were found after the stent was taken out.
Case 2
Medical history
Since 2019, a young female patient around 30 years old has suffered from upper chest pain after meals, along with nausea, vomiting, and occasionally nighttime reflux. These symptoms eased after vomiting. After consulting a local hospital, she was diagnosed with “gastritis” and given symptomatic medication, Nevertheless, her condition failed to improve. In May 2022, she developed dysphagia. Endoscopic and upper gastrointestinal barium tests revealed stenosis of the cardiac orifice, leading to a diagnosis of AC. She was then transferred to the Lanzhou University Second Hospital for treatment in the same month, where her dysphagia was rated as a score of 3 upon admission (Table 1). A thoracoabdominal CT scan revealed dilation of the entire esophagus with effusion and narrowing of the cardia, which was clinically considered to be AC (see Figure 5(a)–(c)). Other examinations showed no abnormalities. Based on the information above, after excluding esophageal malignancies and related injuries, the initial diagnosis was AC (grade III, an Eckardt score of 7 is characterized by clinical symptoms such as weight loss of 5 kg, occasional retrosternal pain, daily dysphagia, and reflux symptoms, or an esophageal maximum diameter >6 cm on imaging.).

Abdominal CT examination. (a) Marked dilatation of the middle and upper esophagus, (b) marked dilatation of the middle and lower esophagus, and (c) constriction of the cardiac portal. CT: computed tomography.
Endoscopic FCSEMS implantation operation
Placement of the FCSEMS was performed via the TTS method as in case 1, as shown in Figure 6. Following operation initiation and contrast injection, dynamic X-ray monitoring approximately 10 seconds postinjection revealed that approximately 90% of the contrast remained in the esophageal lumen, with only 10% passing through the cardia. In contrast, the contrast passage rate approached 100% post-stent implantation.

Metal-coated esophageal stent implantation under nasogastric microscope. (a) Endoscopic introduction of a guide wire into the stomach cavity, (b) endoscopic placement of a metal-coated stent, (c) endoscopic stent dilatation and (d) the stent dilated well on X-ray.
Postoperative treatment
The patient was instructed to drink warm water after 2 hours and consume a liquid diet after 4 hours following the operation. The patient said they experienced significant nausea and reflux within 2 days of stent placement. After 3 days of symptomatic treatment, these symptoms basically disappeared, and the dysphagia score was reduced to 1. One week after treatment, the patient underwent a follow-up endoscopy, which revealed that the stent had shifted below the cardia. After adjusting the stent position, the patient was discharged for recuperation.
Reexamination and follow up
The patient was admitted for a re-examination 2 months after surgery. She said she experienced a foreign body sensation, but no significant dysphagia or other symptoms. The dysphagia score was 1, and her weight remained like before. Endoscopy revealed good expansion of the stent. In response to the patient's and her family's request, the stent removal procedure was performed in July 2022. The patient had no abnormal symptoms after the procedure, and a follow-up gastrointestinal contrast examination showed the lower esophagus to the cardia has poor peristalsis, and the passage of contrast medium is slightly slow, and the upper esophagus is dilated, and the stomach is normal in shape, showing a hook-like contour and the IRP of the lower esophageal sphincter decreased from 28 mmHg pretreatment to 12 mmHg post-treatment. There won’t other abnormalities were found (see Figure 7) and regular re-examination is recommended. As of now, 3 years after the stent placement surgery, through telephone and outpatient follow up, the patient has no relevant discomfort symptoms after eating. The dysphagia score is 1, and the weight has increased by about 8 kg compared with before. The Eckardt scores reduced to 0 post-treatment.

Upper gastrointestinal angiography. (a) Hooked stomach, narrow at the cardia and (b) gastric cavity contrast filling well.
Discussion
AC, a chronic, incurable disorder, stems from loss of inhibitory neurons in the esophagus and LES plexus, heightening excitatory neuron activity, per the 2020 ACG Clinical Guidelines. 8 Reduced levels of nitric oxide and vasoactive intestinal peptides from inhibitory neurons can cause cardiac stenosis, occlusion LES dysfunction, and esophageal peristalsis disruption. 9 AC is often misdiagnosed as gastroesophageal reflux disease (GERD), treated with PPIs. 10 These patients may have swallowing issues, with few experiencing heartburns. For AC and GERD differentiation, generally use gastroscopy, esophageal barium radiography, and esophageal high-resolution manometry (HRM). “Beak-like” sign crucial for AC diagnosis.
Traditional therapies (Table 2), such as medications, botulinum toxin, and balloon dilation, possess inherent limitations. Though surgery holds the potential for cure, it is accompanied by risks including reflux, perforation, and bleeding. 11 FCSEMS, designed to expand luminal muscles with body heat, 12 alleviate digestive obstructions gently and uniformly over time, outperforming balloon dilation in tolerability because the radial expansion force is created spontaneously, slowly, and uniformly during the stent expansion process, as a result, the ripping of muscle tissue is slow and mild. 13 However, their use in benign esophageal strictures is limited by risks like bleeding, perforation, and reflux due to tissue proliferation,14,15,16 and the ease with which long-term expansion can result in muscle fiber tearing and scar stricture.
Comparison of various treatments for achalasia. 11

POEM: Peroral endoscopic myotomy.
While POEM is a highly effective treatment for achalasia cardia, FCSEMS offers potential advantages such as reversibility, reduced procedural complexity, and suitability in patients unfit for surgery. Early-century clinical trials by specialists demonstrated their short- and long-term efficacy and safety. Zheng's retrospective study 17 showed 16.7% patients changed their stents’ position or repositioned them due to the stent displacement, all stents removed within 2 to 6 weeks, with 12.5% patients relapse at 10 to 16 months. Li et al. 18 evaluated retrievable metal stents for AC, observing 7.6% recurrence after 24 months. These results suggest that metal stent is effective in the treatment of AC but reminds high recurrence rate. Another study 19 suggested that extending stent retention decreases recurrence rates and times for AC. Meantime, Kaixiang Feng 20 reported on 21 AC patients treated with large esophageal stents, finding no recurrence and improved QoL over 24 months postremoval, demonstrating the significance of the big stent's impact and the adequate dilatation of the cardia. Comparatively speaking, systematic data reports on the use of retrievable esophageal metal stents to treat AC are currently lacking besides China. According to prior studies, esophageal stent retention times typically range from 1 week to 6 weeks and should be removed after 2 weeks following stent implantation due to the issue of muscle fiber healing time, it is not advised to keep them in place for an extended period. Thus, determining the optimal stent placement duration holds crucial clinical significance. Shutian Xiang 21 noted that 2 patients who removed the stent within 2 weeks (12 days) experienced recurrence during the 60-day follow up. This leads to the preliminary conclusion that some AC patients’ symptoms cannot be effectively reduced after 2 weeks of stent implantation. Using the same stent placement time to treat patients with different variables has certain defects in treatment. In this study, both patients provided verbal informed consent and agreed to have their visit data reported as part of scientific research and reporting of this study conforms to CARE guidelines. 22 The symptoms were significantly worse for both patients and interfering with normal life prestent. To relieve the patient's symptoms as soon as possible and maximize the treatment efficacy, an endoscopic stent implantation was performed on the patient after detailed communication with the patient's family and obtaining their written informed consent. After placing the FCSEMS, the symptoms improved rapidly. Eckardt scores reduced to 0 in both cases and the esophageal mucosa did not suffer from ulceration, bleeding, and other injuries and inflammatory reactions during the retention period and after removal. Notably, neither patient experienced recurrence for a long time, demonstrating the efficacy of FCSEMS for AC treatment in these cases. Under the premise of safety and effectiveness, the stent can play a longer role and save the cost of multiple treatments for patients. Up to now, both patients have no obvious recurrence with remarkable effects.
Conclusion
Endoscopically FCSEMS placement is safe and effective as a noninvasive treatment in the management of AC, and therefore deserves to be promoted in clinical practice.
Footnotes
Acknowledgements
The authors would like to express their deepest gratitude to their tutor for invaluable guidance, insightful feedback, and unwavering support throughout this research. Authors are also grateful to Dr Wang, etc., for the collaborative efforts, particularly in data collection and manuscript revision. This work was supported by funding from multiple projects, including the National Natural Science Foundation of China, which is gratefully acknowledged. Finally, the authors sincerely thank the patients and their families for their contribution to this study in providing data and case information.
Authors’ contributions
BX collected patient information and wrote the manuscript; YW searched for literature; BW and PH processed pictures and prepared tables; and HC provided ideas for writing, revised the article, and offered financial support.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Natural Science Foundation of China (8247104651, 82160129), Key Project of Science and Technology in Gansu province (22ZD6FA054), Key Talents Project of Gansu Province (2019RCXM020), General Project of Gansu Province Joint Research Fund (24JRRA929), Science and Technology Project of Chengguan District of Lanzhou City (2020SHFZ0039, 2020JSCX0073), Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (CY2017-ZD01), Medical Research Innovation Ability Improvement Project of Lanzhou University (lzuyxcx-2022-160), Excellent Textbook Cultivation Project of Lanzhou University (lzuyxcx-2022-45), and Gansu Province Innovation Driven Assistance Project (GXH20230817-14).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All relevant data are fully available within the article.
Disclosure statement
In conducting this research, we adhered strictly to the highest ethical standards to ensure the protection of participants’ rights, privacy, and wellbeing throughout the study process. Both patients provided verbal informed consent and agreed to have their visit data reported as part of scientific research, and we commit that the data sources for this study are authentic and the research conclusions are of high credibility.