
Abstract
Persistent pupillary membranes are a common congenital anomaly that usually resolves spontaneously in early infancy. However, bilateral extensive persistent pupillary membranes that entirely obscure the pupils, involve the visual axis, and adhere firmly to the lens are rarely reported. This report presents a rare case of bilateral extensive persistent pupillary membranes in a young child, resulting in severe visual axis obstruction and firm adhesion to the anterior lens capsule. Surgical removal led to a substantial improvement in visual acuity without complications. This case highlights the importance of early diagnosis and timely surgical intervention to restore vision and prevent long-term complications such as deprivation amblyopia.
Introduction
Persistent pupillary membranes (PPMs) are congenital remnants of the tunica vasculosa lentis, a fetal vascular network that typically regresses by the sixth month of gestation. 1 Although PPMs are observed in up to 95% of neonates, most cases are benign and asymptomatic, resolving spontaneously in infancy. 2 PPMs can be classified as mild (non-obstructive strands) or severe (dense sheets that block the visual axis or adhere to ocular structures). 3 While isolated strands are commonly seen, bilateral, extensive PPMs that adhere firmly to the anterior lens capsule are exceptionally rare, with only a few similar cases reported, and can cause profound visual impairment if untreated.4–6
This report presents a rare case of a young child with bilateral dense PPMs requiring surgical intervention. The case is unique due to the bilateral density of the membranes, their firm adhesion to the lens, and delayed presentation in a rural setting. It underscores diagnostic and surgical challenges, postoperative outcomes, and broader implications for pediatric vision screening and access to ophthalmologic care in underserved areas.
Case presentation
A young child from rural Gansu Province, China, was brought to our ophthalmology clinic at The Second Hospital of Lanzhou University, Lanzhou, China, in June 2023 for her first ophthalmologic evaluation with a reported history of poor vision in both eyes since infancy. Her parents had noted that she often squinted in bright light and avoided direct sunlight, but no prior ophthalmologic evaluation had been performed, particularly no neonatal eye screening.
On presentation, her uncorrected visual acuity (Snellen) was 20/400 in the right eye (OD) and 20/200 in the left eye (OS). Cycloplegic refraction revealed hyperopic astigmatism with a prescription of +2.25−0.75 × 176 in OD and +1.75−1.00 × 180 in OS; however, no improvement in visual acuity was achieved with correction.
Slit-lamp biomicroscopy revealed extensive PPMs in both eyes, completely obscuring the pupils and involving the visual axis. The membranes exhibited a dense, spiderlike appearance (Figure 1(A) and (B)). Anterior segment optical coherence tomography (OCT) demonstrated fully developed membranes spanning the entire pupillary region, with firm attachments to the anterior lens capsule bilaterally (Figure 2(A) and (B)). Posterior segment examination, including funduscopy, revealed no abnormalities, and intraocular pressures (IOP) measured 14 mmHg in OD and 16 mmHg in OS. There were no systemic or syndromic features suggestive of anterior segment dysgenesis or congenital ocular malformations. Other ocular structures appeared normal. The diagnosis of bilateral persistent pupillary membranes was made.
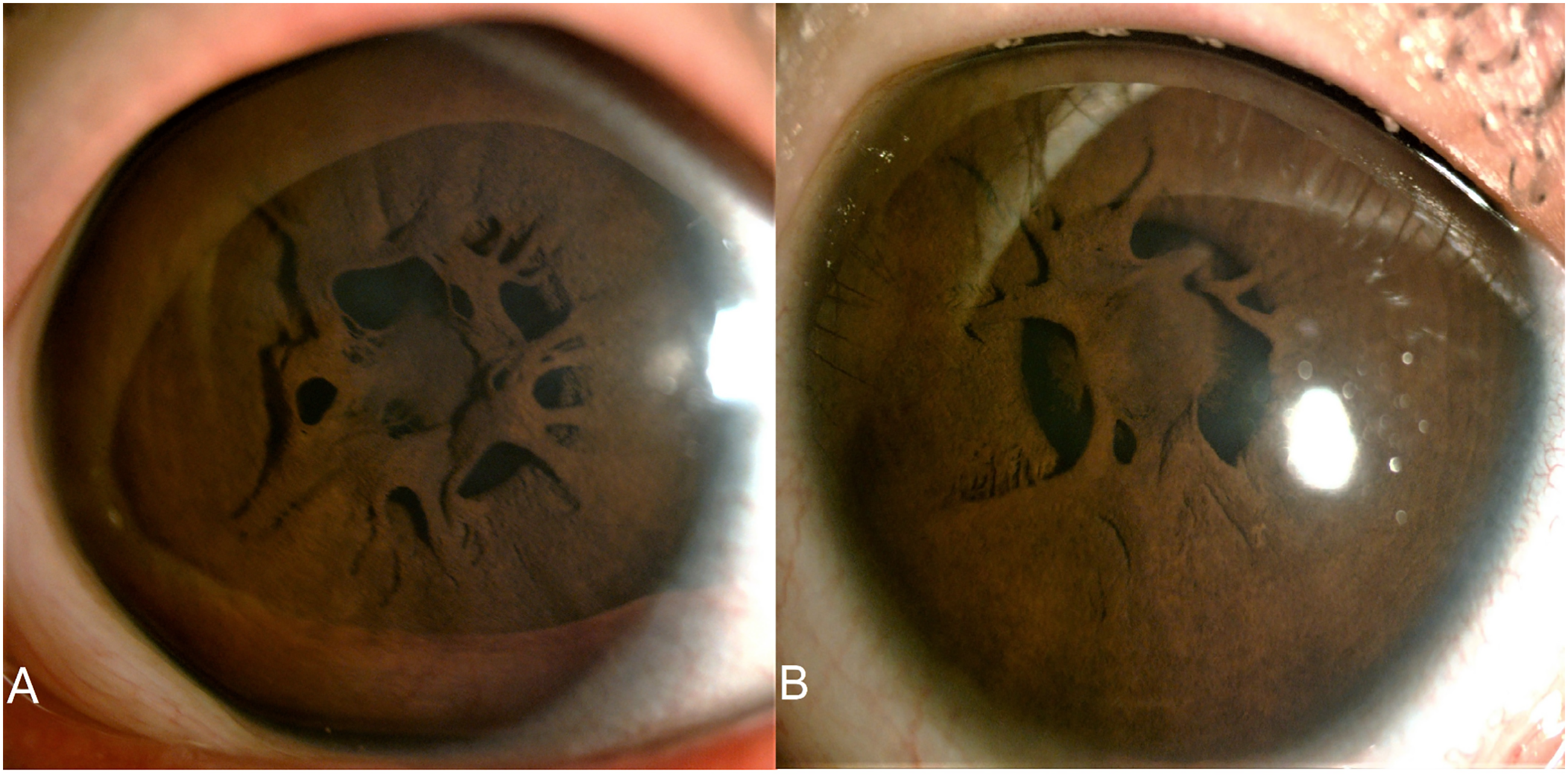
Photos of the anterior segment in the right eye (A) and left eye (B) showed that the persistent pupillary membranes exhibited a dense, spiderlike appearance.
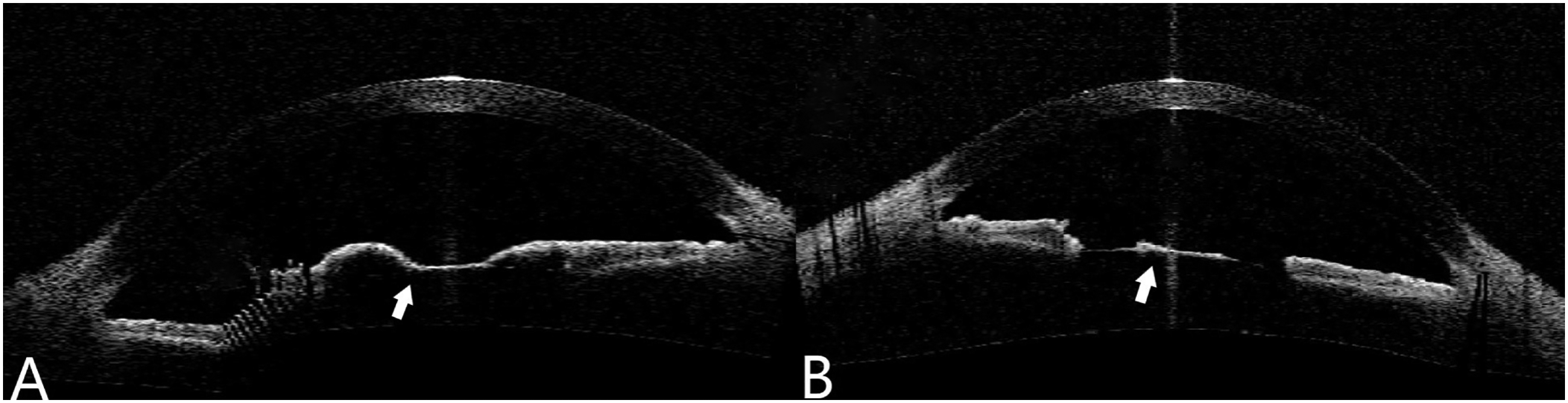
Photos of anterior OCT showed full membranes across both pupils in the right eye (A) and left eye (B) (white arrows show the PPMs attached to the lens).
Given the significant visual axis obstruction and the lack of visual improvement with refractive correction, surgical intervention was deemed necessary. Bilateral surgical removal of the PPMs was performed under general anesthesia. Intraoperatively, the membranes were found to be densely adherent to the anterior lens capsule. To minimize the risk of lens damage, a cohesive viscoelastic was injected to create space and facilitate blunt dissection using micro-forceps under high magnification. Adhesions were carefully peeled from the lens capsule without capsule violation. Postoperatively, the visual axis was clear, and no evidence of cataract formation or other complications was observed (Figure 3(A) and (B)).

Photos of the anterior segment after surgical removal in the right eye (A) and left eye (B) (white arrows show the persistent pupillary membranes (PPMs), pigment substance adheres to the surface of the lens).
The patient was prescribed topical levofloxacin 0.5% four times daily for one week and prednisolone acetate 1% four times daily, tapered over 4 weeks. Follow-up visits occurred at 1 week, 1 month, 6 months, and 1 year.
At the one-week postoperative follow-up, the patient's best-corrected visual acuity (BCVA) had improved to 20/30 bilaterally (OD and OS). The patient reported a significant improvement in her ability to see under various lighting conditions, and no signs of deprivation amblyopia were detected. At the six-month postoperative follow-up, uncorrected visual acuity was 20/40 OD and 20/50 OS, with BCVA of 20/25 OD and 20/30 OS, and the slit-lamp biomicroscopy of her anterior segments was normal. At the one-year postoperative follow-up, the results were consistent with those at the one-year follow-up; uncorrected visual acuity was 20/40 OD and 20/50 OS, with BCVA of 20/25 OD and 20/30 OS. Her visual performance was age-appropriate, and no recurrence or cataract formation was observed.
Written informed consent was obtained from the patient's mother for both treatment and publication. All patient details have been fully anonymized. The reporting of this study conforms to CARE guidelines. 7
Discussion
PPMs are the most common congenital iris abnormality in neonates, with a high prevalence, up to 95% of neonates. 2 They originate from the tunica vasculosa lentis, a fetal vascular network that usually regresses before birth. 1 However, when they persist, PPMs can present in varying forms, ranging from small strands that are asymptomatic to extensive membranes obstructing the visual axis, as observed in this case.3,4 Large or bilateral extensive PPMs with firm adhesion to the anterior lens capsule are rare, with few cases reported in the literature, and may cause significant visual impairment, especially when they obscure the visual axis completely.
Most PPMs are isolated, but an association with other abnormalities has been reported, including congenital cataract, iris coloboma, high refractive errors, and micropthalmos.3–6 In this case, we found the pupillary membranes are firmly adhesion to the anterior lens capsule, making surgical removal both necessary and technically challenging, which is very rare (Figures 2 and 3). Adhesions posed a high risk of damaging the anterior capsule, which could have resulted in cataract formation.
However, if large enough to cause visual axis obstruction, like this case, then surgical removal is indicated to clear the visual axis and reduce the risk of deprivation amblyopia. 8 Alternative management techniques, such as laser membranotomy or pharmacologic mydriasis, have been described in milder cases. 9 However, these are not suitable for dense, adherent membranes like those in our case.
Despite severe anatomical obstruction, this patient did not develop deprivation amblyopia – possibly because the obstruction was symmetric, allowing equal (albeit reduced) visual input to both eyes during critical periods of visual development. This contrasts with most unilateral cases, where amblyopia is more common due to asymmetric input. 8
Only a few similar bilateral cases have been reported in the literature. Ahmad et al. 3 described bilateral PPMs associated with congenital cataract, while Kraus and Lueder 8 reported outcomes of surgical excision in visually significant PPMs. Compared to these, our case is notable for the absence of lens opacification and favorable long-term outcomes without complications.
The successful surgical removal of the membranes resulted in a significant improvement in visual acuity (from 20/400 OD and 20/200 OS to 20/30 bilaterally one-week post-operation). This demonstrates that timely intervention can lead to near-normal visual outcomes, even in cases with extensive PPMs. Large PPMs obstructing the visual axis can lead to deprivation amblyopia, which is challenging to reverse, particularly in unilateral cases. This case emphasizes the importance of identifying and addressing such severe presentations to prevent long-term visual impairment.
This case also underscores a public health concern: in rural areas of China, many children do not undergo vision screening until school age. Studies show delayed diagnosis of visual disorders in rural and migrant populations is common. 10 This case underscores the need for improved access to pediatric ophthalmologic care and education for parents and caregivers about the importance of early visual screenings in rural or underserved areas. It highlights how early intervention can significantly impact a child's visual development and quality of life. Thus, more effort needs to be put into the relevant social publicity and health science popularization in those areas.
Conclusion
This case illustrates the successful surgical management of a rare, bilateral presentation of extensive PPMs with firm adhesion to the anterior lens capsule in a child. Despite the severity of the obstruction, visual acuity improved significantly following timely intervention, without long-term complications. Bilateral involvement may have mitigated the risk of amblyopia, emphasizing the importance of early detection. This case highlights the need for proactive pediatric eye screening and access to surgical care, especially in underserved populations. Ophthalmologists should consider surgical excision for dense PPMs obscuring the visual axis, and public health policymakers should promote earlier vision checks in children to prevent avoidable visual disability.
Footnotes
Author contributions
Peng Lu: conceptualization, surgery, and manuscript drafting. Wenwen Tian and Juan Wang: data collection, literature review, and patient consent. Yadong Wang: surgical assistance and critical revision of the manuscript. All authors reviewed and approved the final version.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bethune Charitable Foundation (grant number 2023A-040) and Full-English Curriculum Construction Cultivation Project of Lanzhou University (grant number: lzuyxcx-2022-89).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All relevant data supporting the findings of this case report are included within the article. Further details are available upon reasonable request from the corresponding author.
Patient consent
Written informed consent was obtained from the patient's mother for publication of this case report and any accompanying images.