
Abstract
The resection of middle ear paragangliomas can be challenging given their vascular nature and the small volume of the tympanic cavity, particularly when the tumor in the hypotympanum is close or attached to the internal carotid artery (ICA). We performed combined underwater endoscopic and microscopic surgery for a Class B1 middle ear paraganglioma according to the modified Fisch classification. The suspicious bone in the hypotympanum and around the petrous ICA was drilled with underwater endoscopy. The feeding arteries, the caroticotympanic and inferior tympanic arteries, were suctioned and cauterized under microscopy. To the best of our knowledge, no case of middle ear paraganglioma treated with underwater endoscopy has been reported. Underwater endoscopy, providing a clear operative field with blood and bone dust irrigation, is a good indication for middle ear paragangliomas. In contrast, microscopic preparation for unexpected bleeding is important, particularly when the tumor closely extends to vital structures, such as the ICA or the jugular bulb.
Keywords
Introduction
Parangangliomas, formerly defined as benign tumors, are no longer classified as benign or malignant, because any lesion can have metastatic potential and no clear-cut features can predict metastatic behavior since the 4th edition of the World Health Organization classification. 1
Middle ear paragangliomas, commonly known as “glomus tympanicums,” originate from the glomus bodies that lie along Jacobson's nerve (tympanic branch of the IX nerve) and Arnold's nerve (auricular branch of the X nerve). 2 Fisch 3 classified temporal bone paragangliomas into Classes A, B, C, and D, and this classification was subsequently modified by Sanna. 4
Transcanal and/or retroauricular microscopic surgery is the traditional approach for middle ear paragangliomas.5,6 A transcanal microscopic approach is typically preferred for smaller tumors (Class A), whereas larger tumors often require a postauricular approach for tumor resection and bleeding control.
Recently, endoscopy has been remarkably introduced in managing middle and inner ear pathologies, and transcanal endoscopic management7–9 was reported for early-stage middle ear paragangliomas.
Due to their highly vascular nature, significant bleeding can be experienced during surgery, particularly when the tumor is close or attached to the internal carotid artery (ICA). In this situation, preparation for unexpected bleeding might be more important than the minimally invasive approach, which does not require external incisions.
We performed combined underwater endoscopic and microscopic surgery for a Class B1 middle ear paraganglioma. The suspicious bone in the hypotympanum and around the petrous ICA was drilled with underwater endoscopy, and significant bleeding of the caroticotympanic artery was managed with suction and cauterization under microscopy.
Case report
A 48-year-old female visited a nearby otolaryngologist with a 1-month history of hearing impairment in the left ear. The patient had pulsatile tinnitus 2 years ago; however, she had no history of facial nerve palsy. She was referred to our department with suspicion of a middle ear paraganglioma.
Clinical examination revealed a retrotympanic red mass filling the middle ear cleft with extension to the hypotympanum (Figure 1A). Pure-tone audiometry of the left ear revealed mean air and bone-conduction hearing levels of 33.3 and 0.0 dB at 500, 1000, and 2000 Hz, respectively. Computed tomography (CT) revealed a middle ear mass originating from the promontory, extending into the hypotympanum; however, the ossicular chain seemed to be preserved (Figure 1B and C). Gadolinium-enhanced magnetic resonance imaging showed an enhanced middle ear mass isolated from the jugular bulb (JB) and ICA (Figure 2). Based on the aforementioned findings, we diagnosed the patient with Class B1 middle ear paraganglioma.

(A) Left ear. A pulsatile reddish mass can be observed in the middle ear cavity. The margins of the tumor are unclear in the otoscopic finding. (B, C) Preoperative computed tomography image of the left ear showing the tumor (star) in middle ear extending to the hypotympanum. The bony walls of the JB and the ICA were not apparently eroded by the tumor, though the bone in the hypotympanum was suspiciously infiltrated by the tumor. M, malleus; ICA, internal carotid artery; JB, jugular bulb; white arrowhead, caroticotympanic artery.

(A, B) Preoperative gadolinium-enhanced magnetic resonance imaging shows an enhanced middle ear mass in the middle ear cleft (white arrowhead). The enhanced mass was isolated from the JB and the ICA. C: internal carotid artery, JB: jugular bulb, S: sigmoid sinus.
During surgery, a postauricular skin incision was made under general anesthesia. After, a circumferent canalplasty was performed, the tympanic membrane (TM) was elevated from the bony annuls and the surface of the tumor. In contrast, the TM was not detached from the handle of the malleus because of possible avoidance of postoperative lateralization of the TM. The chorda tympani and ossicular chain were preserved. The tumor was removed by piecemeal excision, and the inferior tympanic artery was coagulated. Then, the suspicious bone in the hypotympanum was drilled with underwater endoscopy. Bleeding from the caroticotympanic artery was encountered and was managed by coagulation under microscopy. After total tumor removal with endoscopic investigation, the tympanomeatal flap was replaced using fascia (Figure 3).
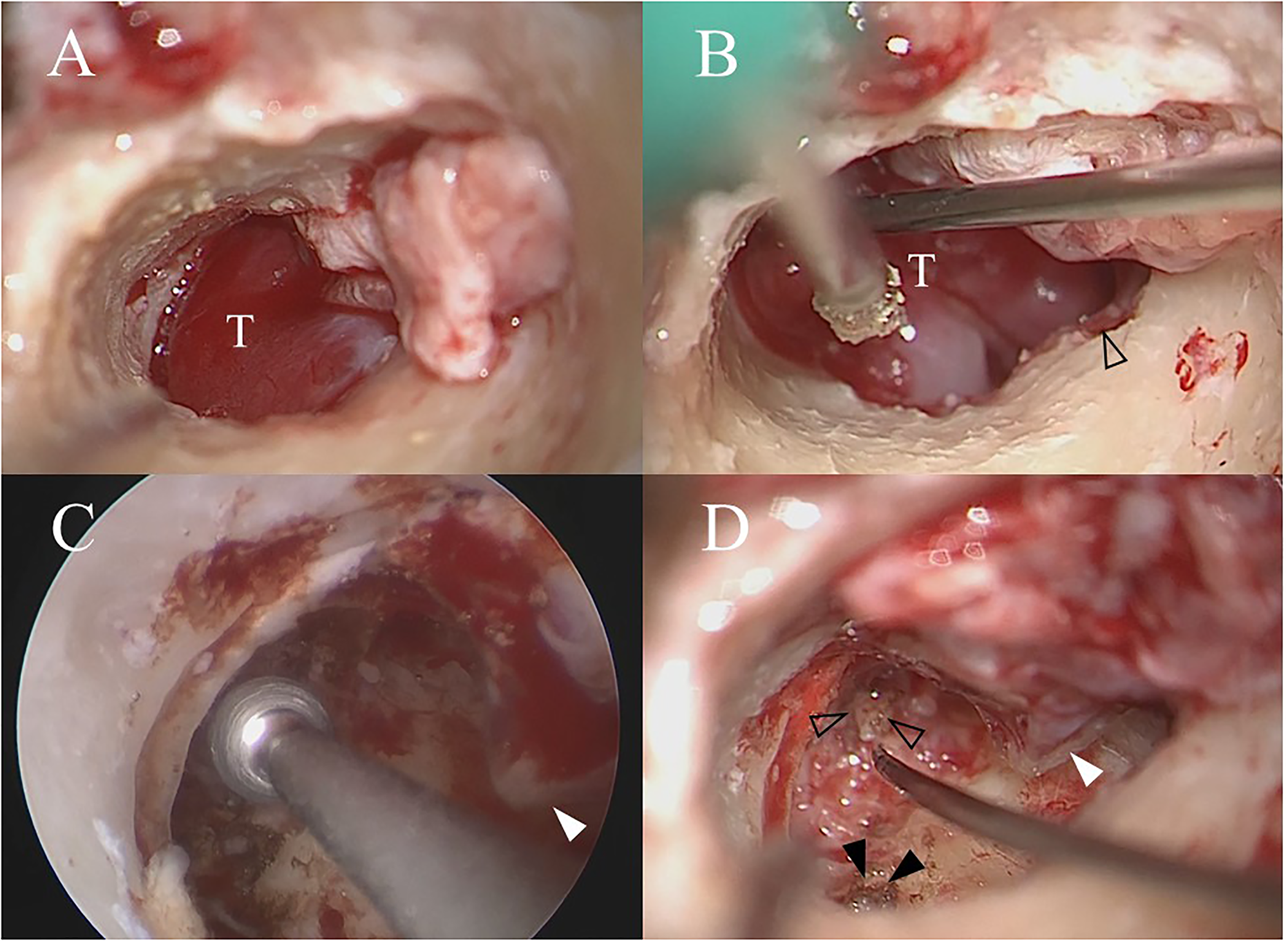
(A) Canalplasty was performed, and the tumor in the middle ear was well-identified. The tympanomeatal flap was elevated while preserving the malleus handle. (B) The tumor in the middle ear was removed by piecemeal excision with the preservation of the chorda tympani (arrowhead) and ossicular chain. (C) Underwater endoscopic view. The suspicious bone in the hypotympanum was drilled out with the preservation of the cochlea, JB, and ICA. The handle of the malleus was identified (white arrowhead). (D) Surgical view after total tumor removal. The inferior tympanic (black arrowhead) and carticotympanic (arrowhead) arteries were coagulated to achieve total tumor removal. The handle of the malleus was identified (white arrowhead). T, tumor.
The patient's postoperative clinical course was uneventful, without dizziness, pulsatile tinnitus, taste disturbance, and facial nerve palsy. The left ear cavity had dried within 3 months after the operation (Figure 4A), and the patient's hearing improved postoperatively, demonstrating mean air and bone-conduction hearing levels of 13.3 and 1.7 dB at 500, 1000, and 2000 Hz, respectively. Postoperative CT revealed the total tumor removal in the middle ear cavity (Figure 4B and C).

(A) Otoscopy image of the left ear 6 months after surgery. The tympanic perforation is not observed after hypotympanotomy. (B, C) CT image of the left ear 6 months after surgery showing that the bone in the hypotympanum is drilled out and the bony walls of the JB and the ICA around the carticotympanic artery (white arrowhead) are preserved. M, malleus; ICA: internal carotid artery, JB: jugular bulb.
Discussion
Paragangliomas have undetermined biological potential and should not be termed benign. 10 Multiple therapeutic options are available for managing temporal bone paragangliomas; however, regarding middle ear paragangliomas, surgical excision is considered a safe procedure, allowing total tumor removal with minimal morbidity and better outcome durability.5,6
In cases of middle ear paragangliomas, both microscopic and endoscopic techniques have advantages and drawbacks. Endoscopy provides a magnified, wide surgical view, improved illumination, and the ability to visualize around corners, whereas the retroauricular approach with canal calibration under microscopy has faster and easier bimanual results. 11
Moreover, an innovative technique reported by Yamauchi et al. as underwater endoscopic ear surgery was proposed to repair superior canal dehiscence and labyrinthine fistulas with good results and has the advantages of preservation of inner ear function and clear operative view.12,13 This technique provides a clear operative field without the need for suction and also protects the inner ear and other important structures, including the JB, from unexpected aeration. 14 In cases of middle ear paragangliomas, significant bleeding can be experienced during surgery because of their vascular nature; thus, underwater endoscopy is appropriate for this case because of continuous blood and bone dust irrigation during suspicious bone drilling in the hypotympanum and around the ICA.
The middle ear arteries anastomose extensively to each other, and the promontorial region is mainly supplied by the inferior tympanic artery, which is a branch of the ascending pharyngeal artery and often accompanied by the Jacobson's nerve, and the caroticotympanic artery from the vertical portion of the ICA. 15
In this case, we performed microscopic ear surgery assisted with underwater endoscopy. The tumor was fed by both the inferior tympanic and carticotympanic arteries. Underwater endoscopy, in which the middle ear cleft is filled completely with saline by perfusion, is useful for obtaining a clear operative view with continuous blood and bone dust irrigation during bone drilling in the hypotympanum and around the ICA. The carticotympanic artery was coagulated bipolarly under a microscope bimanually with an enlarged external auditory canal.
Thus, regarding the surgical approach, the best modality or combination of modalities should be chosen to cure the patient and prevent any complications or tumor recurrence as much as possible for minimally invasive and risky surgery.
Conclusion
We report a case of combined underwater endoscopic and microscopic surgery for a Class B1 middle ear paraganglioma. The suspicious bone in the hypotympanum and around the petrous ICA is drilled under underwater endoscopy. Both the inferior tympanic and caroticotympanic arteries are suctioned and cauterized under microscopy. To the best of our knowledge, no case of middle ear paraganglioma treated with underwater endoscopy has been reported. Underwater endoscopy, providing a clear operative field with blood and bone dust irrigation, is a good indication for middle ear paragangliomas. In contrast, microscopic preparation for unexpected bleeding is important for minimally invasive and risky surgery, particularly when the tumor is closely extending to vital structures, such as the ICA or JB.
Footnotes
Author contributions
YT conceived and designed the case report, contributed to the clinical diagnosis and treatment, collected all data, wrote and revised the manuscript. AT, KS, HO, EI, and MN clinically contributed to this study. SH and TN contributed to literature research. FM supervised the conduct of this study. All the authors approved of the final manuscript.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from Research Ethics Committee Faculty of Medicine, Juntendo University (JHS23-021).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japan Society for the Promotion of Science (grant number 21K09566).
Patient consent for publication
Written Informed Consent was obtained from the patient for the publication of this case report and the accompanying images.
Author biographies
Yusuke Takata received his medical degree (2003) from Tohoku University. He received his PhD degree (2011) in Otorhinolaryngology & Head and Neck Surgery from Tohoku University. He is currently working at Juntendo University Hospital. His research interests include otology, neurotology and skull base surgery.
Takashi Anzai received his medical degree (2009) from Juntendo University. He received his PhD degree (2015) in Otorhinolaryngology & Head and Neck Surgery from Juntendo University Graduate School of Medicine. He is currently working at Juntendo University Hospital. His research interests include otology, neurotology and skull base surgery.
Kenji Sonoda received his medical degree (2015) from Juntendo University. He is currently working at Juntendo University Hospital. His research interests include otology, and hereditary hearing loss.
Hiroko Okada received her medical degree (1995) from Tottori University. She is currently working at Juntendo University Hospital. Her research interests include otology.
Erina Ishimizu received her medical degree from Kitasato University in 2018. She is currently working at Juntendo University Hospital and is enrolled in a PhD program in the Department of Otorhinolaryngology, Juntendo University Graduate School of Medicine. Her research focuses on obstructive sleep apnea.
Masahiro Nakamura received his medical degree (2010) from Osaka Medical College. He received his PhD degree (2020) in Otorhinolaryngology & Head and Neck Surgery from Juntendo University. He is currently working at Juntendo University Hospital. His research interests include endoscopic sinus surgery and skull base surgery.
Satoshi Hara received his Medical Degree from Juntendo University, Tokyo, Japan (2012) and Doctor of Philosophy (Ph.D.) in Otorhinolaryngology & Head and Neck Surgery from Juntendo University Graduate School of Medicine (2021). He is currently working at Johns Hopkins University, Baltimore, Maryland, United States and Juntendo University, Japan. His research interests include otology and neurotology.
Takumi Nakayama received his medical degree (2019) from Juntendo University. He is currently working at Juntendo University Hospital. His research interests include otology.
Fumihiko Matsumoto received his medical degree (2000) from Juntendo University. He received his PhD degree (2006) in the Department of Otorhinolaryngology from Juntendo University Graduate School of Medicine. He is currently working at Juntendo University Hospital. His research interests include otology, oncology and head and neck surgery.