
Abstract
Neurofibroma is a rare nerve sheath tumor of neuroectodermal origin, especially the huge and isolated neurofibroma located in the inguinal region. To our knowledge, no such case has previously been reported. We report a case of 34-year-old male patient with a 4-year history of progressive enlargement of the medial root mass in his left thigh with sitting and standing disorders along with pain. The tumor was completely removed by operation, and pathological diagnosis showed neurofibroma. There was no obvious neurologic defect after surgery, and no recurrence tendency was found in the follow-up of 2 years. For a large solitary mass with slow growth and no malignant clinical manifestations for a long time, clinicians cannot rule out the hypothetical diagnosis of neurofibroma, even though its growth site is very rare, such as this case of a huge tumor located in the groin. For neurogenic tumors, early operation should be performed, and the prognosis of patients after tumor resection is excellent.
Background
Neurofibroma are benign nerve sheath tumor that originate from neuroectoderm, grow along a nerve or nervous tissue. 1 They account for only 5% of all benign soft tissue tumors. 2 The giant type of solitary neurofibroma without presentation of type I neurofibromatosis (NF-1) is even rarer, and to the author’s knowledge, this type located in the groin region has no relevant case been reported.
Case presentation
A 34-year-old male had a progressively enlarged mass in his left inner thigh root for 4 years. He complained about sitting and standing disorders along with pain. The patient had no previous history of trauma and denied the family history of Von Recklinghausen’s disease. Physical examination showed that the mass was solid, movable with clear boundary. Tinel sign in his inguinal region was positive. No other anomalies were found. Electromyogram suggested that the sensory nerve conduction velocity (SCV) of the affected side was slightly slower than the contralateral. Laboratory tests were normal. And X-ray of left limb showed the bone invasion and destruction caused by the mass (Figure 1). Magnetic resonance imaging (MRI) manifested a circular abnormal signal focus in the left pubic muscle space with clear boundary, and has low signal on T1-weighted image (T1WI), high signal on T2-weighted image (T2WI). There was patchy or flocculent shadow of long T1 and short T2 signal in the mass (Figure 2). After injection of contrast medium, the capsule was significantly enhanced, while the inside of the mass was enhanced slightly and unevenly, and the boundary between the mass and the surrounding muscles was clear (Figure 3). Generally, primary diagnosis was benign tumor and nerve source was considered first, thus preoperative biopsy is not considered which may cause complications related to neurogenic tumor.

In the anteroposterior (a) and lateral (b) radiographs of X-ray, there were slight osteolytic features of ischial and pubic branches which was indicated by the black arrow in Figure 1(a), along with the increased acetabular density and sharpened edges, and manifested a huge soft tissue shadow which was indicated by the red arrows.

An abnormal signal foci with clear circular boundary in the left pubic space on MRI, about 8.2×7.4×8.4 cm in size. Figure (a) and (b) was the coronal plane of MRI and figure (c) and (d) was the transverse section of MRI. It had slightly lower signal on T1WI (a, c) and high signal on T2WI (b, d). There was patchy or flocculent shadow of long T1 and short T2 signal in the mass with a visible capsule.

After injection of contrast medium, the capsule was significantly enhanced, while the inside of the mass was enhanced slightly and unevenly, and the boundary between the mass and the surrounding muscles was clear.
Then the patient underwent radical resection of the tumor. The mass sized 10.6 × 8.5 × 5.5 cm with intact capsule was found to originated from the femoral nerve, and some of the surrounding nerve fiber tracts were extruded extremely thin by it (Figure 4). After excising the tumor, the femoral nerve was released. Pathological findings showed that the tumor cells were mainly spindle cells in the shape of ticking tadpole, and the background was rich in mucus like substances (Figure 5). The results of immunohistochemistry were S-100 (+), CD34 (vascular+) (Figure 6). These proved the diagnosis of neurofibroma. After the operation, there was no neurologic defect in the patient. Two years after follow-up, the daily life of patient had no adverse affection, and no local recurrence was discovered.

After muscle incision of sartorius, it was found that the tumor with intact capsule originated from the femoral nerve, and the base of it was located in the pubic muscle, the whole mass was between the groin and the inner thigh, about 10.6 × 8.5 × 5.5 cm in size.

Pathological findings (HE stained): (a) ×50, the capsule was intact, (b) ×400, the tumor cells were mainly spindle cells, (c) ×400, the background was rich in mucus like substances, (b) and (c), the cells were in the shape of ticking tadpole.
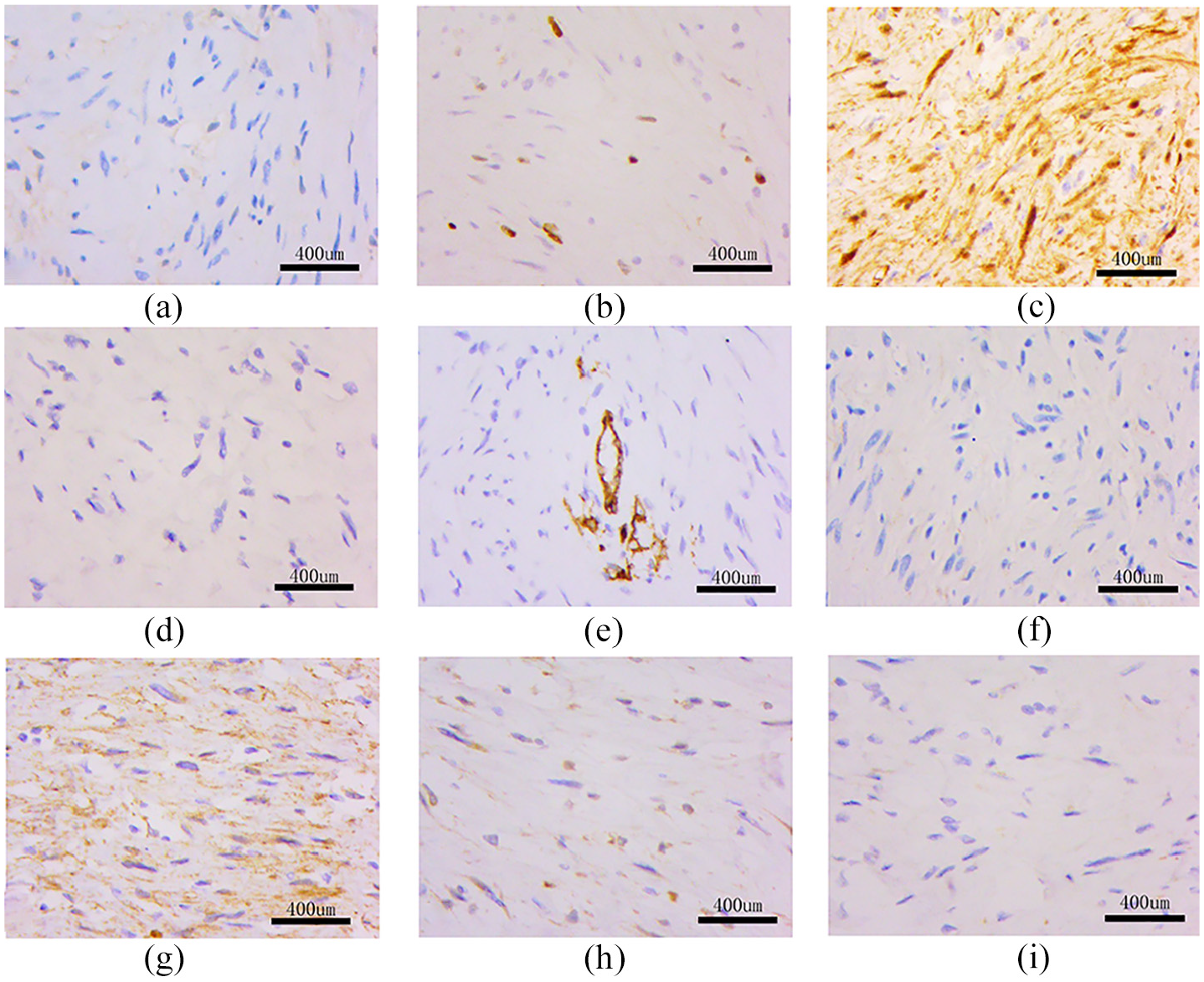
The results of immunohistochemistry (×400): (a) CK (Pan) (−), (b) Ki-67 (about 2% +), (c) S-100 (+), (d) desmin (−), (e) CD34 (vascular+), (f) SMA (−), (g) β-Catenin (+), (h) bcl-2 (−), and (i) CD99 (−).
Ethical approval was given by the medical ethics committee of the First Affiliated Hospital, College of Medicine, Zhejiang University, and the written informed consent was obtained from the patient for his anonymized information to be published in this article.
Discussion
Neurofibroma is a rare benign nerve sheath tumor composed of Schwann cells, perineural like cells and fibroblasts.3,4 The solitary type is usually a small polypoid mass with its maximum size of less than 2cm.5,6 Only 10% neurofibromas are related to NF-1,7,8 but due to the effect of NF-1, this type has larger volume, higher tendency of malignant transformation and higher recurrence rate.5,9,10 Therefore, though no correlation performance was found in this case, clinically, we should actively look for manifestations of von Recklinghausen’s disease to exclude the possibility of malignancy.
Neurofibroma usually grows slow, has no sexual or age preference and no discomfort, 11 its diagnosis is mainly depending on the result of imaging and microscopy. Schwannoma is the most difficult to differentiate, for they has homologous lesions and similar imaging manifestations. MRI might be a good choice.12–14 Compared with schwannoma, neurofibroma often lacks complete capsule, 15 and has rich myxoid tissue to show a characteristic T2WI with low signal inside and high signal outside.9,16 However, the solitary mass of this case is not only huge with unique location, but also has complete capsule on MRI without the target sign. Thus final diagnosis depends on the pathological examination. First, unlike schwannomas, the parent nerve of neurofibroma is usually separable in plexiforms rather than isolated ones. 15 Secondly, neurofibroma is rich in mucoid tissue, while schwannoma has a compact stroma. 9 Additionally, the nuclei of neurofibroma are slender and wavy, while schwannomas’ are oblong and have Verocay bodies.5,11 Besides neurofibroma has uneven staining of S-100, local immune response to epithelial membrane antigen (EMA), and strong CD34 positive, while schwannoma has more intense and uniform staining of S-100, and the capsule stained EMA.2,5
As biopsy has a risk of causing nerve damage, which is likely to occur in this case as some of the nerve fiber tracts were extruded particularly thinly by the tumor. Thus, the preferred treatment for neurofibroma is still complete resection, which has good postoperative prognosis and low recurrence.2,3 However, the parent nerve of neurofibromas is usually unseparable in solitary neurofibromas. 15 Thus, it should be noted that under the premise of complete resection, the scope of tumor resection should be precisely determined, and microsurgery is recommended, and the parent nerve and non-involved nerve fibers need to be preserved as much as possible, so as to avoid serious risk of nerve injury and the sacrifice of the parent nerve. Alternative therapies include enucleation and subtotal resection, but often have inevitable recurrenc. 15 Radiotherapy, a feasible method, is only used to control or reduce the growth of isolated lesions, and is effective for juvenile angiofibroma. 17 Therefore, in consideration of the limitation and huge type of the focus in this case, as well as the adverse effects on patient’s daily life, we performed a complete resection of the tumor in this patient with respect to the neighboring neurovascular structures and the parent nerve.
Conclusion
In general, this paper presents a rare case of giant solitary neurofibroma located in the groin area without NF-1 performance. When tumor becomes too large or too deep, it can cause neurological symptoms or compression symptoms of adjacent organs and may also bring difficulty to operation and cause poor prognosis. Therefore, early diagnosis is important, which can be achieved by MRI and clinical manifestations. The confirmed diagnosis is through pathological sections. As most of the neurofibromas show good limitations, preferred treatment is still surgery, especially in this case with large and isolated neurofibroma. Good prognosis and low recurrence rate are obtained after radical resection.
Footnotes
Author contributions
HL designed the study, performed data collection, analyzed the results, and HY Z drafted the manuscript. All the authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (the grant number 81702135), Zhejiang Provincial Natural Science Foundation of China (grant number LY20H060007, LS21H060001), the Zhejiang Traditional Chinese Medicine Research Program (grant number 2016ZA124, 2017ZB057) and Zhejiang Medicine and Hygiene Research Program (grant number 2016KYB101, 2015KYA100). The funding bodies had no role in the design of the study; in collection, analysis, and interpretation of data; and in drafting the manuscript.
Ethics approval
Ethical approval to report this case was obtained from *The medical ethics committee of the First Affiliated Hospital, College of Medicine, Zhejiang University (2018(566))*.
Consent for publication
Written informed consent was obtained from the patient for publication of clinical details and clinical images. Upon request, a copy of the consent form is available for review by the Editor of this journal.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be publishedin this article.