
Abstract
Objective
Gastrointestinal diseases are common, yet some countries still lack endoscopy. Modern flexible endoscopy was introduced to the Solomon Islands National Referral Hospital (NRH) in 2012, but little is known about gastrointestinal disease in the country.
Methods
This retrospective cohort study describes trends in upper gastrointestinal diseases to inform local research and health programming. Demographic, clinical, and endoscopic data, including rapid urease test (RUT) results for H. pylori, were abstracted from consecutively entered patient medical records at the NRH.
Results
A total of 761 patients underwent upper endoscopy and RUT (2019–2022). Although RUT was positive in only 25.8% of patients (N = 196), relatively common findings of erosions (N = 90, 11.8%) and ulcers (N = 89, 11.7%), as well as frequently reported symptoms of upper gastrointestinal bleeding (N = 168, 22.1%), suggest a higher true prevalence of H. pylori-associated peptic ulcer disease in this cohort. Age was associated with an endoscopic finding of ulcers on univariate analysis. Multivariable modeling indicated a significant association between the presence of gastric erythema and erosions and the diagnosis of duodenitis. Multivariable regression also showed symptoms of melena and hematemesis to be significantly associated with the endoscopic finding of ulcers. Among patients treated for H. pylori who underwent follow-up endoscopy and RUT, 28.8% failed treatment.
Conclusion
There was a high degree of concern regarding gastrointestinal symptomology and pathology in this cohort. Access to endoscopy and RUT in Solomon Islands remains limited to a single endoscopy unit. Future efforts should explore non-invasive clinical pathways for the expansion of RUT and the management of ulcer disease in Solomon Islands.
Introduction
The global distribution of gastrointestinal disease disproportionately impacts countries according to sociodemographic indicators, with incidence, prevalence, death rates, and disability-adjusted life years (DALYS) remaining highest in countries with low levels of sociodemographic development. 1 The high global burden of gastrointestinal disease is multifactorial, resulting from both non-infectious and infectious etiologies. In low- and middle-income countries (LMICs), factors including diet, immune-compromising comorbidities, genetics, body-mass index, environment, healthcare infrastructure, as well as tobacco and alcohol use contribute to the high prevalence and severity of gastrointestinal disease. Some infectious diseases such as Hepatitis B, Hepatitis C, and Helicobacter pylori (H. pylori) cause chronic gastrointestinal disease, contributing to the high burden of gastrointestinal cancers in LMICs. 2 Indeed, H. pylori is the most common cause of infection-attributable cancers worldwide and it is estimated that roughly half of the global human population are infected with H. pylori. 2 H. pylori dominates as a cause of upper gastrointestinal disease, notably peptic ulcer disease and gastric cancer. The bacterium's pathogenicity has been attributed to several established virulence-associated genes, such as the cytotoxin associated gene A (cagA) gene that is located within the cag pathogenicity island. 3
Gastrointestinal endoscopy has been widely used in high-income countries for about 50 years to detect and treat upper gastrointestinal disease. However, its implementation has been slower in LMICs due to deficits in human resources, infrastructure and training, and competing health needs.4,5 Pacific island countries and territories (PICTs) face high burdens of both infectious and non-communicable diseases, climate change, and geographic isolation together with a high incidence of gastrointestinal disease and sparse access to gastroenterological care.6,7 Furthermore, while global access to safe drinking water has increased in recent years, some PICTs in Melanesia such as Fiji and Solomon Islands actually experienced a decline in access between 2010 and 2020. 8 In Solomon Islands, poor sanitation coverage as well as the widespread practices of open defecation and unsafe sewage management likely contribute further to the high incidence of gastrointestinal disease.8,9
The first formal endoscopy program at the National Referral Hospital (NRH) in Solomon Islands was established in 2012 with help from international partners. 10 Prior to this, endoscopy was performed ad hoc by visiting physicians or by local surgeons with minimal formal training in endoscopy using a rigid endoscope with an eyepiece. The modern endoscopy unit at the Solomon Islands NRH, equipped with flexible endoscopes and video feed, is the only service regularly offering endoscopy in the country. In this unit, the mainstay of H. pylori detection is by RUT on gastric biopsies, 11 with material support from the Australia and New Zealand Gastroenterology International Training Association (ANZGITA). The NRH endoscopy unit is vital in identifying and treating gastroenterological pathologies, including gastric cancer. 12
The RUT is performed routinely in patients undergoing upper endoscopy at the NRH except in cases of laboratory shortages, esophageal obstruction, or known active gastrointestinal bleeding. The RUT protocol in Solomon Islands is based on the protocol developed by Arvind et al. (Appendix 1) 13 and validated and field-tested by Katelaris et al. 14
Per Solomon Islands treatment guidelines, patients diagnosed with H. pylori infection are typically treated with either a 14-day regimen of omeprazole (20 mg 2 ×/day), amoxicillin (500 mg 3 ×/day), and metronidazole (400 mg 3 ×/day) or a 7 to 14-day regimen of omeprazole (20 mg 2 ×/day), clarithromycin (500 mg 2 ×/day), and amoxicillin (1 g 2 ×/day). 15 The second treatment regimen is prescribed in cases of prior failed treatment or if the patient has used metronidazole previously. The duration of this therapy is determined by the prescribing physician.
The decision to administer antibiotic treatment may be based on RUT results, endoscopic findings, or both. Providers may prescribe either treatment regimen based on the patient's reported medical history as well as the provider's clinical judgment.
In establishing the Solomon Islands Endoscopy Partnership, stakeholders included data collection and publication among its goals for this new program. 10 In the decade since the start of endoscopy in the country, this is the first research study to analyze that data in order to inform local and regional preventing and health service planning.
Methods
Study design
A retrospective medical records review was completed, including all patients who underwent upper gastrointestinal endoscopy and RUT at the NRH between 1 January 2019 and 31 December 2022. Data were extracted from 29 fields including demographic information, health behaviors, symptoms, nonsteroidal anti-inflammatory drug (NSAID) use, endoscopic findings, diagnosis (completed by endoscopist prior to pathology result), histology, H. pylori status (by RUT), as well as health and family history. Endoscopic findings encompassed anatomical abnormalities noted during endoscopy whereas diagnoses referred to the disease or illness that was ultimately diagnosed, considering the patient's clinical, laboratory, and endoscopic findings. Data were also collected regarding follow-up endoscopy and RUT testing. All data were de-identified prior to analysis.
For patients who underwent upper endoscopy and RUT on multiple occasions during the study period that was not related to follow-up endoscopy for H. pylori treatment (N = 10), the study team recorded endoscopy data associated with the first positive RUT result in the database. Additional data on treatment response and follow-up endoscopy were collected for all patients who attended post-treatment follow-up.
This study was conducted in accordance with the Helsinki Declaration of 1975 as revised in 2024. The reporting of this study conforms to STROBE guidelines. 16
Statistical analysis
Statistical analysis was performed using Python 3.9.6 and R 4.3.1. Descriptive analysis was performed to report the frequency of categorical variables and the mean or median of continuous variables. Univariate analyses investigated associations between NSAID usage and the endoscopic diagnoses of gastric ulcers, and duodenitis. Univariate analysis utilized χ2, Fisher's exact, and Kruskal-Wallis tests where applicable.
Multivariable logistic regression modeling was performed for the following outcomes: diagnosis of duodenitis, gastroscopy finding of ulcers, and gastroscopy finding of erosions. Variables of potential significance for inclusion in the multivariable models were identified based on a review of literature and clinical guidelines. Following standard practice, any variable whose variance was < 0.05 was dropped from the analysis since variables with low variance may not explain the variance in our target outcome. 17 A LASSO regression analysis on the remaining features was performed for each outcome to identify the most informative features to be included in the logistic regression. 18 The regularization parameter (lambda) was optimized using cross-validation to minimize the mean square error of the model. After the LASSO regression was performed, features with non-zero coefficients were retained and included in each target's logistic regression model while controlling for age, sex, and province of origin.
Results
A total of 761 upper alimentary tract endoscopies with RUT were performed during the study period. Demographic data are summarized in Table 1. Most patients (n = 501) were men (65.8%), overall mean age was 43.7 years (range 5–89). A positive RUT was reported for 196 (25.8%) of patients. Most patients listed Malaita (n = 334, 43.9%) or Guadalcanal (n = 111, 14.6%), the two most populous provinces, as their primary province of origin. Among the 266 (35.0%) of the sample who reported an occupation, the most common job was market or subsistence farmer (n = 175, 65.8%). The most common medications that patients reported taking included NSAIDs (N = 47, 6.2%), anti-hypertensive agents (N = 45, 5.9%), and anti-diabetic medication (N = 26, 3.4%).
Demographic and clinical characteristics of the study population.

GI: gastrointestinal; IQR: interquartile range; NSAID: nonsteroidal anti-inflammatory drug.
Patients were asked whether they currently use tobacco products, alcohol, and/or betelnut.
Clinical characteristics and endoscopic findings
Clinical data are reported in Table 1. There were 24 unique symptoms reported. The most common were upper gastrointestinal discomfort (N = 497, 65.3%), and upper gastrointestinal bleeding (N = 168, 22.1%). The most common comorbidities were hypertension (N = 62, 8.2%), type 2 diabetes mellitus (N = 52, 6.8%), ischemic heart disease (N = 30, 3.9%), hepatitis B infection (N = 28, 3.7%), and gout (N = 21, 2.8%). The most common drug allergy reported was to co-trimoxazole (N = 74, 9.7%). A significant proportion of patients endorsed regularly drinking alcohol (N = 248, 32.6%), chewing betelnut (N = 436, 57.3%), and smoking tobacco (N = 288, 37.8%).
Endoscopic findings, diagnoses, and histology are reported in Table 2. Common endoscopic findings included erythema or red mucosa (N = 586, 77.0%), erosions (N = 90, 11.8%), and ulcers (N = 89, 11.7%). The most common endoscopic diagnosis overall was duodenitis (N = 78, 10.3%). With regard to the 106 patients who had samples sent for histology, the most common diagnosis was gastritis (N = 38, 41.3%). Among those diagnosed with ulcers (N = 89), 73 patients had Forrest type III ulcers (82.0%). Furthermore, among patients found to have one or more ulcers on endoscopy, histology results were present in the medical records of 32 patients (36.0%). 87 patients (11.4%) had normal endoscopic results.
Most common endoscopic findings, endoscopic diagnoses, and histological diagnoses.
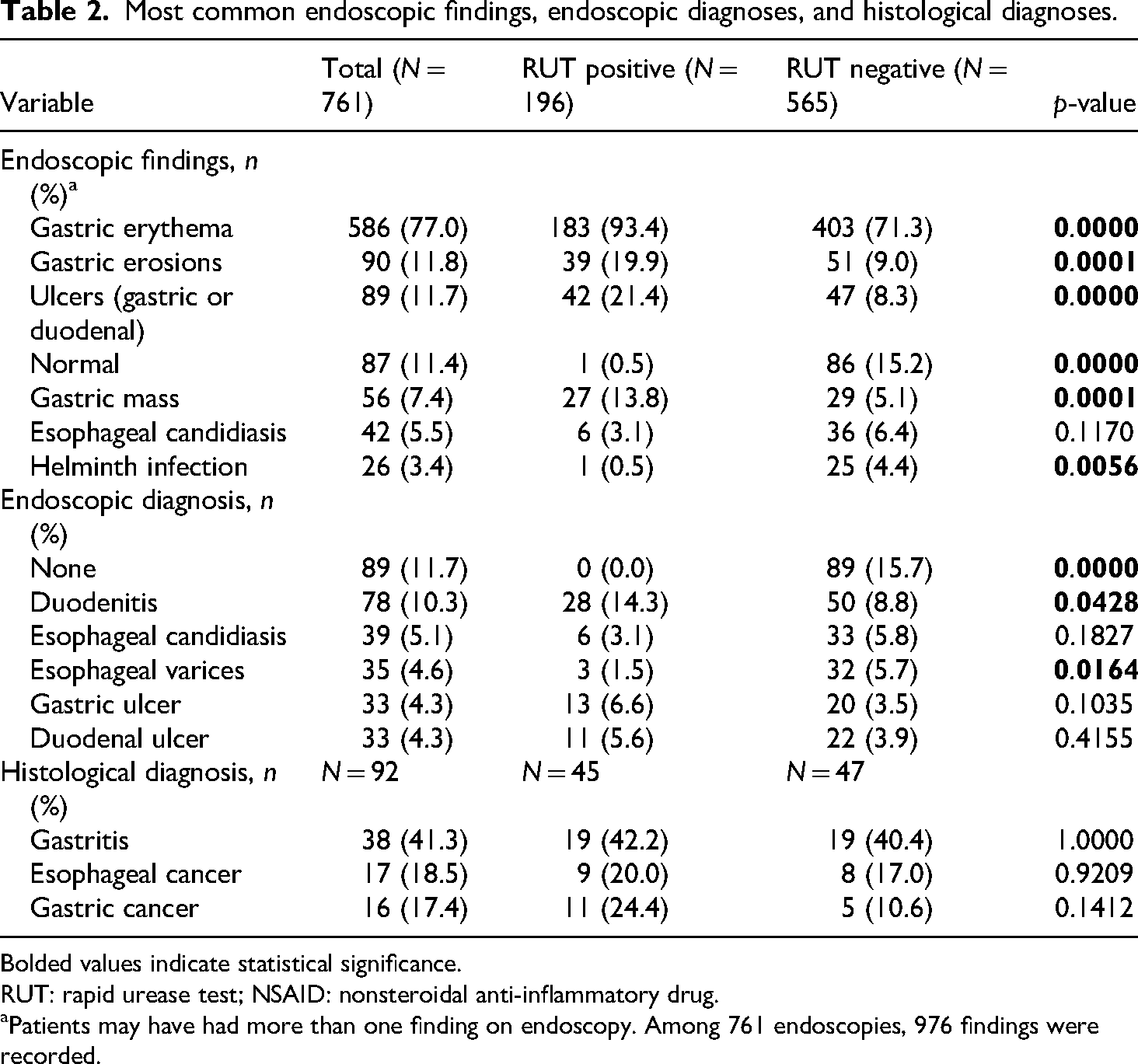
Bolded values indicate statistical significance.
RUT: rapid urease test; NSAID: nonsteroidal anti-inflammatory drug.
Patients may have had more than one finding on endoscopy. Among 761 endoscopies, 976 findings were recorded.
Within the study period, 36 patients who underwent endoscopy were diagnosed with cancer via histology. A summary of histological results and biopsy location is presented in Table 3. Cancer was identified and biopsied in the stomach (N = 18, 50.0%), esophagus (N = 9, 25.0%), gastroesophageal junction (N = 8, 22.2%), and duodenum (N = 1, 2.8%).
Cancer diagnosis, biopsy location, and histology.

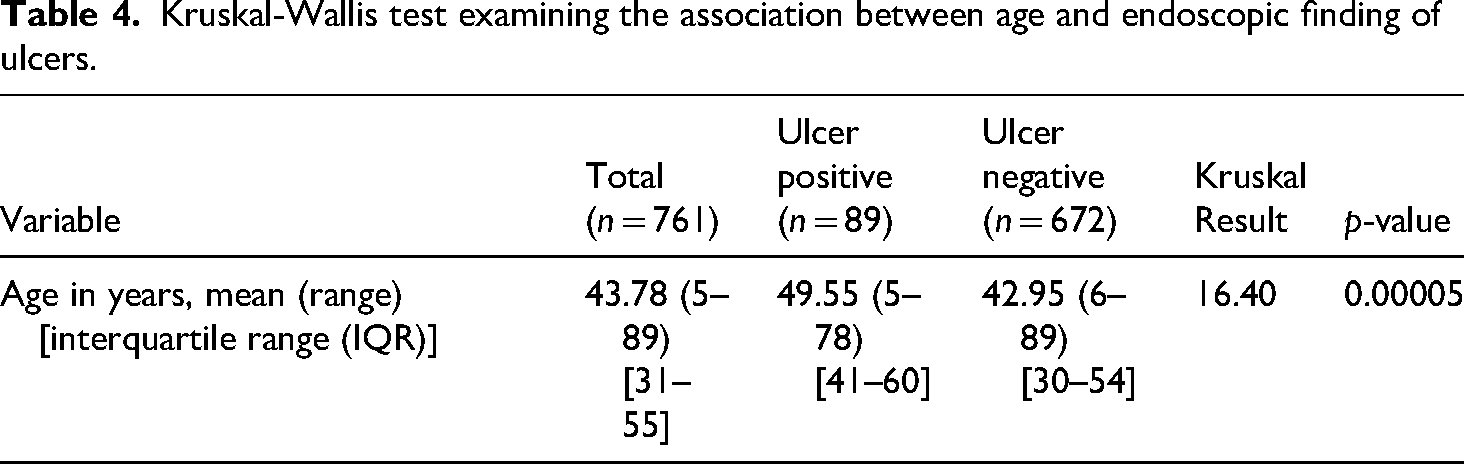
Age was found to differ significantly between patients with an endoscopic finding of ulcers and those without (p < 0.01). The mean age of patients with an endoscopic finding of ulcer was greater by 6.6 years. The results of this analysis are reported in Table 4.
Kruskal-Wallis test examining the association between age and endoscopic finding of ulcers.
NSAID usage and diagnosis
Overall, 41 patients (5.4%) had a history of upper gastrointestinal discomfort associated with NSAID use prior to endoscopy. 110 patients (14.5%) reported taking NSAIDs regularly. NSAID usage was not significantly associated with a diagnosis of gastric ulcer, duodenal ulcer, or duodenitis (Table 5).
Univariate analysis examining nonsteroidal anti-inflammatory drug (NSAID) usage with endoscopic diagnoses.

H. pylori management
A total of 292 patients were prescribed antibiotic treatment for H. pylori. 106 (36.3%) patients were prescribed 14-day regimens while 186 (63.7%) received a 7-day regimen. Among those treated for H. pylori, 213 (72.9%) had follow-up data available. Of these 213 patients, 138 (64.8%) underwent follow-up endoscopy, 37 (17.4%) were lost to follow-up, and 38 (17.8%) were not scheduled for repeat endoscopy. Among patients who did undergo repeat endoscopy, 125 also received a repeat RUT. The RUT was not performed on the remaining 13 patients either because these patients had a negative initial RUT result, or because the endoscopist focused on more pressing concerns such as variceal banding, stenting, diagnosis of cancer, or gastric outlet obstruction. 36 (28.8%) patients had a positive follow-up RUT result. 4 (11.1%) of these treatment failures were initially prescribed a 7-day treatment, while 32 (88.9%) had received the 14-day treatment.
Multivariable logistic regression
When controlling for age, sex, and province of origin, our regression model identified two variables significantly associated with an endoscopic diagnosis of duodenitis (Supplemental Table 1), namely the endoscopic findings of gastric erythema and erosions. Symptoms of upper gastrointestinal bleeding, including melena and hematemesis were significantly associated with an endoscopic finding of ulcers, as expected (Supplemental Table 2). Furthermore, an endoscopic diagnosis of erosions was associated with an endoscopic finding of erythema (Supplemental Table 3).
Discussion
This is the first comprehensive study of endoscopy from Solomon Islands. The sample was demographically diverse, including all nine provinces of Solomon Islands as well as patients with occupations ranging from subsistence farmer to politician; this is likely attributable to the centralization of endoscopic services in Solomon Islands.
A key finding was the high prevalence of gastrointestinal pathology observed. For instance, more than 20% of patients presented with symptoms of upper gastrointestinal bleeding, and ∼5% were diagnosed with upper gastrointestinal tract cancer. This likely results from delays in patient presentation, but it may also reflect effective triage for endoscopic assessment by local physicians. Solomon Islands has an approximate total population of 819,198 19 but has only 0.2 doctors per 1000 people according to World Bank data 20 and a limited workforce capacity for endoscopy. Therefore, NRH doctors must prioritize the most ill patients for endoscopy, as suggested by these findings.
Several challenges were noted in obtaining histological results for this cohort, as demonstrated by the comparatively limited number of histological results reported in this study. Currently, tissue samples from the NRH endoscopy unit are sent to Australia for histological analysis. Samples may be destroyed or lost in transit. Additionally, results are often delayed by lengthy transit times. The lack of local pathology labs may delay or even prevent diagnosis in cases of rapidly progressive neoplasms such as esophageal squamous cell carcinoma. These gaps may ultimately impair the delivery of timely care, thus negatively impacting patient outcomes.
The paucity of doctors in Solomon Islands ranks medical coverage in the country below other developing nations, such as Afghanistan and Sudan. 20 In other limited-resource contexts, delays in presentation have been associated with more advanced pathologies such as cancer. Despite the high mortality incidence ratio for cancer in Solomon Islands (0.87), 21 and the established benefits of H. pylori eradication for gastric cancer prevention, 22 if given in early adulthood (as is the practice in well-resourced high prevalence countries such as Japan), such a strategy is not currently feasible in Solomon Islands at present.
An important finding was the high prevalence of peptic ulcer disease—a condition that is cured in most cases by an inexpensive short course of H. pylori eradication therapy, thus preventing major morbidity and mortality and loss of productive years of life. 22 This is therefore an important target for local guidelines formulation regarding empirical diagnosis and treatment of ulcer disease, given the high prevalence identified in this study.
The positivity rate of H. pylori in this study was low at 25.8%, Other studies from the Pacific region have documented a much higher rate of H. pylori positivity, even above 90%.23,24 A recent meta-analysis suggested a pooled regional H. pylori prevalence of 46.8% in the Western Pacific region, 25 and prior research demonstrates H. pylori positivity is over 80% in duodenal ulcer disease. 26 The low RUT positivity in our cohort in general, and among patients with duodenal ulcer specifically (only 33%, N = 11), suggests that the RUT as used in the NRH endoscopy unit has a high false negative rate. Further evaluation of the in-house RUT against commercially available RUTs or other modalities of H. pylori detection are needed locally as the test has been validated elsewhere.14,27 As the test is unbuffered, the pH of the solution and, therefore, the accuracy of the test is affected by small variations in the formulation of reagents. Similarly, RUT sensitivity is affected by how the test is stored and how the biopsy is placed in the RUT tube. Shaking the tube for example may lead to false negative interpretation as the color plume that indicates a positive result may be rapidly dissipated. It is very unlikely that the high rate of ulcer prevalence identified in this study is due to any other cause than H. pylori, especially as NSAID use was quite low. By way of contrast, the test was initially validated in a region of similarly high ulcer prevalence in India. There, the RUT correlated well with commercial urease tests and the H. pylori rate was 77%. 28
Given limited access to endoscopy or non-invasive diagnostic tests for H. pylori, clinical guidelines for low-resource regions like Solomon Islands, the World Gastroenterology Organization recommends empirical eradication therapy in clinical settings where ulcer disease is highly likely based on typical symptoms and clinical course. 29
With regards to H. pylori management, we cannot determine in this retrospective study the rationale for clinical decisions regarding which patients to treat, nor on the choice of treatments in individual cases. While only 196 patients tested positive upon RUT, 292 were treated for H. pylori. The treatment of a large number of patients without a positive RUT result may reflect limited provider confidence in the results of RUT. Interestingly, current protocols within Solomon Islands prescribe 14-day therapy as a “first-line” treatment and 7-day therapy as a “second-line” therapy, 15 which is not consistent with current global guidelines. 29 Efforts to identify local antimicrobial resistance rates are required to determine the best choice of eradication therapy, but ensuring good adherence to established recommended therapies for resource-poor regions may be even more important. 29 Further efforts to improve record-keeping and record-sharing within and between medical centers may improve our understanding of H. pylori treatment practices in Solomon Islands. Additionally, research on H. pylori treatment outcomes in Solomon Islands and the feasibility of extending treatment to achieve a cure may help to refine current protocols and improve cure rates. Dissemination of current global guidelines, and other educational initiatives to improve H. pylori management appear warranted.
The aforementioned concerns regarding RUT insensitivity at the NRH likely also impacted the reported treatment failure rates, as RUT is the only outcome measure for H. pylori treatment in this setting. Thus, the actual number of patients who failed treatment is probably higher than the reported 28.8%. High rates of treatment failure are usually attributable to incomplete therapy adherence and antibiotic resistance. 29 In Solomon Islands, where comprehensive medical records do not exist, patients may undergo successive, incomplete antibiotic therapy, contributing to further bacterial resistance and treatment failure.
One potential approach to alleviating the burden of H. pylori infection in Solomon Islands is to decentralize testing and treatment modalities. In many countries, testing for and treating H. pylori in the general population offers a cost-effective intervention that can save both money and lives by detecting and curing ulcer disease, and by preventing gastric cancer development. 22 Community-based H. pylori screening and treatment has demonstrated usefulness in pilot programs in Indigenous communities in other Asia-Pacific countries. 30 Screening for H. pylori with a non-invasive 13C-urea breath test or stool antigen test combined with treatment of those who test positive may help reduce the burden of H. pylori in Solomon Islands while also providing better estimates of population-based prevalence of infection. Community-based screening may additionally help in detecting and treating cases of asymptomatic H. pylori infection. However, determining whether such a program is feasible in Solomon Islands, would have to be carefully evaluated with consideration as to whether it is practical, as well as whether it is the optimal use of resources against other competing health and societal needs.
Other community-based efforts should focus on mitigating the environmental risks of H. pylori infection. Overcrowding, substandard household sanitation, improper waste disposal, and poor water quality are associated with H. pylori prevalence in other resource-limited contexts.31,32 Public health efforts focusing on improving waste disposal, sanitation, and water quality in the country may aid downstream eradication efforts.
The creation of standardized follow-up protocols would also aid eradication efforts. Current recommendations advise the use of urea breath or H. pylori stool antigen testing to confirm eradication at least four weeks post-treatment. 33 Follow-up endoscopy for the sole purpose of demonstrating H. pylori eradication is unnecessary and poor use of limited endoscopic resources. The provision of urea breath or stool antigen tests and the implementation of treatment protocols that incorporate their use may offer superior cost-effective and non-invasive methods of confirming cure. 33
Limitations
The dataset used for this study reflects routine patient care at a single hospital. It is therefore limited by the accuracy and completeness of data collection practices and site-specific biases limiting generalizability. One notable challenge was the completeness of medical records—for example, occupation data were entered for only 35.0% of patients in this cohort.
Regarding statistical analysis, LASSO regression was used to identify the most relevant features of our dataset as it encourages sparsity in the statistical model. LASSO regression has some practical limitations, especially where the number of features considered vastly exceeds the number of samples in the dataset. In such cases, the number of features selected will always be less than the number of samples, thus possibly ignoring features of potential importance. Moreover, if there are many correlated features in the dataset, the LASSO regression will tend to select one of the variables and ignore all others. However, its wide use in multiple disciplines and strong practical performance make it appropriate in this setting.
Conclusion
This is the first study of endoscopy from Solomon Islands. Our findings of frequent advanced disease diagnosis suggest the need to increase access to endoscopic services in Solomon Islands, necessitating the collaboration of local health systems with international partners. The key finding in this study is the high prevalence of peptic ulcer disease, which, despite low local RUT sensitivity, is very likely related to H. pylori. Future research and interventions should focus on evaluating the poor sensitivity of locally-made RUTs, assessing the national prevalence of H. pylori infection, broadening access to endoscopy and H. pylori testing, determining local antimicrobial resistance patterns, improving follow-up mechanisms for patients undergoing antibiotic therapy, and developing local guidelines for H. pylori management.
Supplemental Material
sj-pdf-1-sci-10.1177_00368504251355383 - Supplemental material for Upper endoscopy in Solomon Islands: A four-year retrospective study
Supplemental material, sj-pdf-1-sci-10.1177_00368504251355383 for Upper endoscopy in Solomon Islands: A four-year retrospective study by Dylan M Bush, Stallone Kohia, Adrian Garcia Hernandez, Scott Siota, Elizabeth Wore, Rooney Jagilly, Augustin Melly, Peter H Katelaris, Mark W Norrie, Alexandra LC Martiniuk and Steven F Moss in Science Progress
Footnotes
Ethical considerations
Ethical approval was provided by the Solomon Islands Health Research Ethics Review Board, Honiara, Solomon Islands (Project number HRE004/23). As this study utilizes retrospective analysis of clinical data, the need for patient consent was waived by the Solomon Islands Health Research Ethics Review Board.
Author contributions
DMB and SK developed research questions and designed this study. SK led data collection. AGH led data analysis and contributed to the Methods section of this article. DB coordinated the writing of the Introduction, Results, Discussion, Limitations, and Conclusion sections of this article. SS, EW, RJ, and AM edited rough draft articles and provided further contextual information from the Solomon Islands endoscopy unit during the writing process. PHK and MWN assisted with data interpretation and presentation. ALCM and SFM supervised data analysis and writing. All authors contributed to the text and content of this article. All authors approve of the content of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.